
Your belly contains two completely different fats
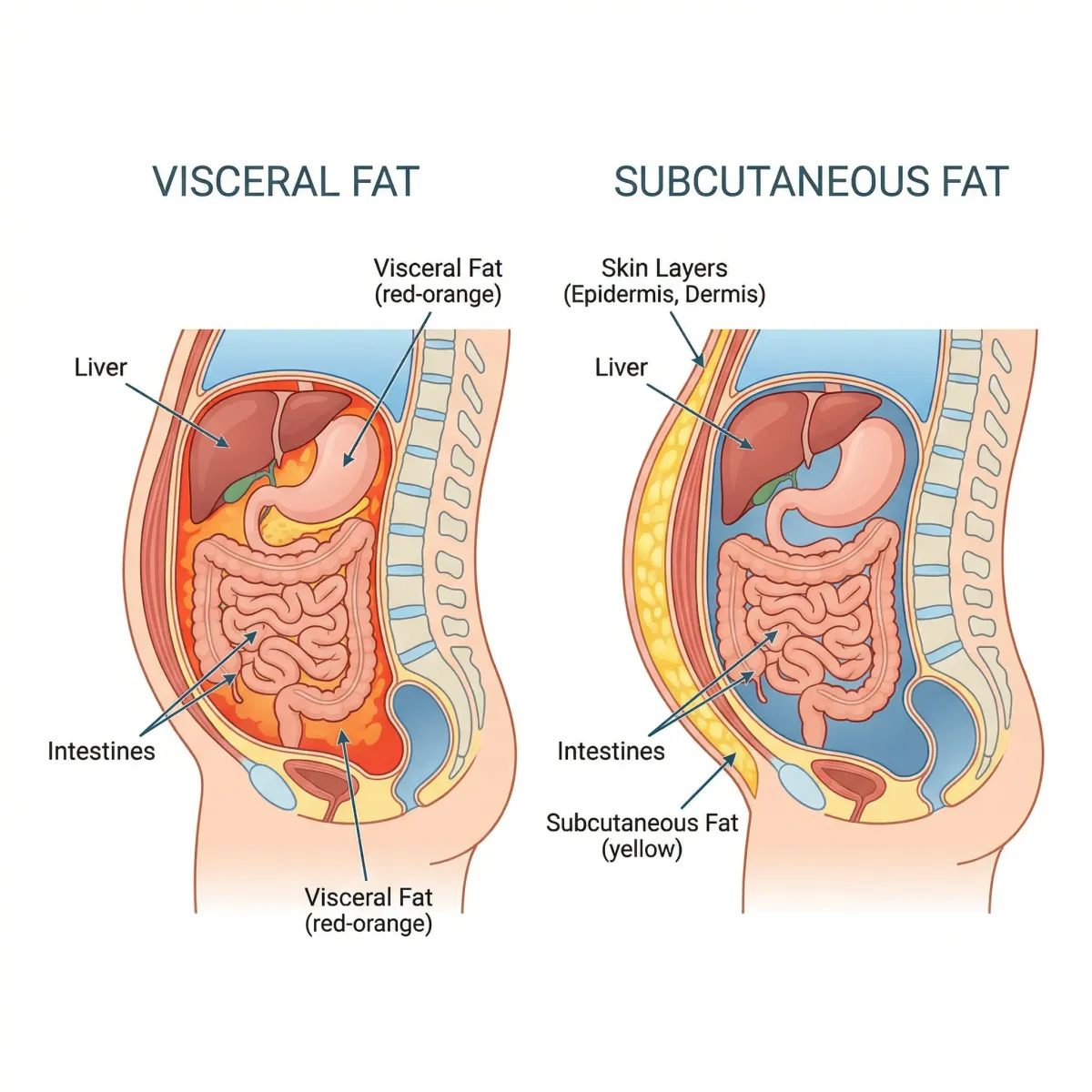
Pinch the skin around your midsection and you're grabbing subcutaneous fat — the padding that sits between your skin and muscle wall. It stores energy, insulates your body, and, in moderate amounts, is metabolically harmless. The fat you can't pinch is the one worth worrying about.
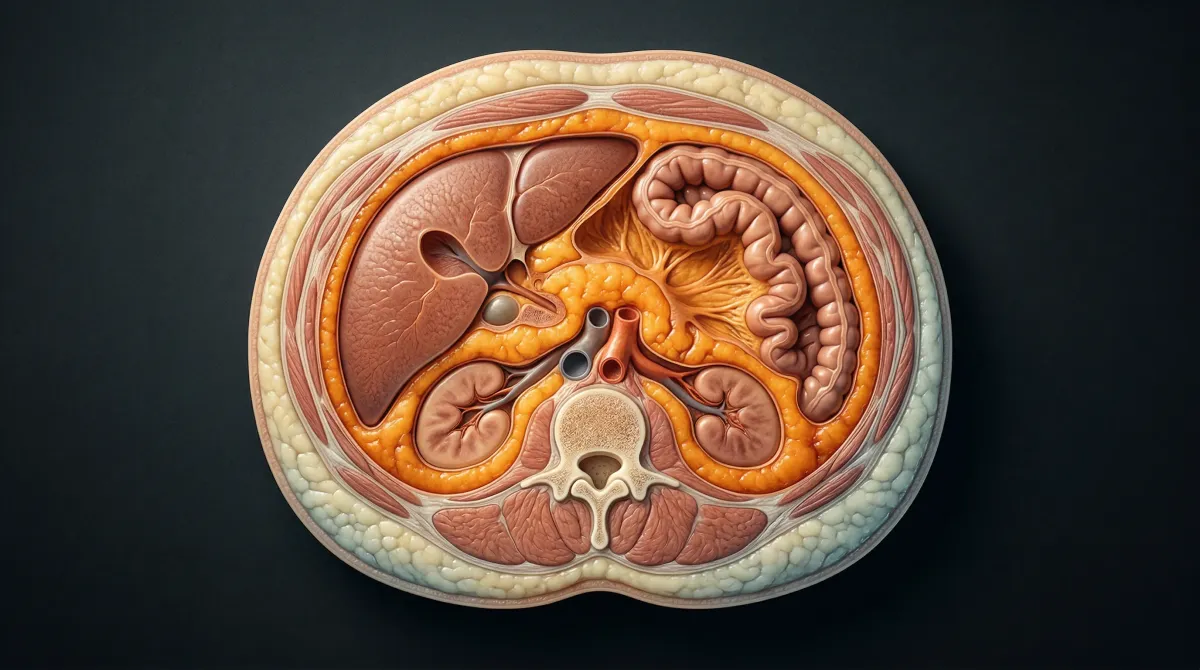
Visceral adipose tissue (VAT) lines your abdominal cavity and wraps around your liver, intestines, pancreas, and kidneys. A thin layer of it cushions and protects those organs. But when it accumulates beyond what your body needs, it shifts from protective padding to a metabolically active tissue that actively disrupts hormone signaling, promotes chronic inflammation, and drives insulin resistance.
A 2024 review in the International Journal of Molecular Sciences found that VAT is the single strongest adipose tissue predictor of type 2 diabetes, outperforming BMI, waist circumference, and waist-to-hip ratio. Among Korean men with high VAT, the odds ratio for diabetes was 15.9 compared with those with low VAT. Meanwhile, about 30% of Americans classified as obese by BMI never develop metabolic disease. Location of fat, it turns out, matters more than quantity.
| Feature | Visceral fat | Subcutaneous fat |
|---|---|---|
| Location | Deep abdominal cavity, around organs | Just beneath the skin |
| Can you feel it? | No | Yes (pinchable) |
| Cell size | Large adipocytes | Smaller adipocytes |
| Metabolic activity | High — rapidly releases free fatty acids | Low — acts as energy "buffer" |
| Insulin sensitivity | Resistant | Sensitive |
| Disease risk | Strong link to T2D, CVD, cancer | Weak or neutral |
| Ease of loss | Responds faster to exercise/diet | Slower to mobilize |
The cascade of damage that starts in your belly
Visceral fat cells behave more like a rogue endocrine organ than a passive energy depot. They pump free fatty acids (FFAs), inflammatory cytokines, and hormones into your bloodstream. Because visceral adipocytes are insulin-resistant, the normal brake on fat breakdown (lipolysis) doesn't work properly. FFAs pour into the portal vein, which delivers them straight to your liver.
Once those FFAs reach the liver, they fuel gluconeogenesis (glucose production), creating a feedback loop: more blood sugar, more insulin demand, more resistance. The same FFAs accumulate in skeletal muscle fibers and get converted into ceramides and diacylglycerols — metabolites that directly impair insulin signaling pathways, reducing glucose uptake into muscle tissue.
Visceral fat does not merely correlate with metabolic disease. It drives disease through specific pathways: free fatty acid release into the portal vein, chronic low-grade inflammation, and direct disruption of insulin signaling in muscle and liver tissue.
The cardiovascular damage is equally direct. A 2023 review in Frontiers in Cardiovascular Medicine detailed how VAT generates chronic low-grade systemic inflammation that accelerates atherosclerosis and contributes to residual cardiovascular risk even in patients already receiving standard treatments. Among 3,173 patients with type 2 diabetes, CT-measured visceral fat area showed a dose-response relationship with cardiovascular disease, with risk climbing progressively as visceral fat increased.
According to the Mayo Clinic, having a large amount of belly fat — regardless of overall weight — raises the risk of high blood pressure, unhealthy blood lipids, sleep apnea, heart disease, type 2 diabetes, certain cancers, fatty liver disease, and early death from any cause.
Consider this: as of 2019, 57.9% of type 2 diabetes-related deaths worldwide occurred in people whose BMI classified them as non-obese. Many of those people carried excessive visceral fat while appearing to be at a healthy weight.
| Condition | Mechanism linking visceral fat | Evidence strength |
|---|---|---|
| Type 2 diabetes | FFA-driven insulin resistance in liver and muscle | Strong (multiple systematic reviews) |
| Cardiovascular disease | Chronic inflammation, atherosclerosis acceleration | Strong (dose-response in large cohorts) |
| Fatty liver (NAFLD) | Portal vein FFA delivery, hepatic lipid accumulation | Strong |
| Certain cancers | Inflammatory cytokines, altered hormone metabolism | Moderate (epidemiological) |
| Sleep apnea | Mechanical pressure on diaphragm and airways | Moderate |
| Dementia | Neuroinflammation, vascular damage | Emerging |
Sex, genetics, and the "thin-fat" phenomenon
Where your body deposits fat depends on factors that are mostly out of your hands, at least at the outset.
Estrogen promotes subcutaneous fat storage by increasing antilipolytic receptors and enhancing adipogenesis in subcutaneous tissue. Women of reproductive age tend to store fat in their hips and thighs (the "pear" shape), keeping visceral deposits relatively low. After menopause, as estrogen drops, this protective pattern breaks down. Fat redistributes toward the abdomen, and women begin accumulating visceral fat at rates closer to men.
Men face a different challenge. Testosterone promotes lipolysis (fat breakdown), which sounds beneficial until you follow the freed fatty acids: they travel through the bloodstream and get re-absorbed by visceral fat deposits around the abdomen, creating the characteristic "apple" shape. Women can store roughly 0.37-0.42 micromol of FFAs per kilogram per minute in their subcutaneous tissue. For men, that number drops to 0.22-0.27 — meaning more FFAs overflow into visceral storage.
Researchers have also documented what they call the "thin-fat phenomenon" — individuals from East and South Asian backgrounds tend to carry more visceral fat relative to their BMI than those of European or African descent. One study found that Japanese-Americans had the highest mean visceral fat area among all ethnic groups studied, despite having an obesity prevalence rate of only 8.7% (compared with 49.5% among African Americans, who had the least visceral fat). This helps explain why 60-80% of type 2 diabetes cases in several Asian countries occur in non-obese individuals.
Aging makes all of this worse. Hormone levels shift, muscle mass declines, and the body's capacity to store fat subcutaneously shrinks. Fat that used to sit in the thighs or arms migrates toward the abdomen. That redistribution changes disease risk, not just clothing size.

How to measure visceral fat: from a tape measure to a full-body scan
You can't see visceral fat and you can't feel it, which makes measurement tricky. There are options ranging from free-at-home methods to clinical-grade imaging, each with different accuracy tradeoffs.
At-home measurements
Waist circumference is the simplest screening tool, and it's more useful than BMI for predicting visceral fat levels. Place a tape measure around your bare abdomen just above your hip bones, exhale normally, and read the number without sucking in.
| Measurement | Increased risk threshold (women) | Increased risk threshold (men) |
|---|---|---|
| Waist circumference | >35 inches (89 cm) | >40 inches (102 cm) |
| Waist-to-hip ratio | >0.85 | >0.90 |
| Waist-to-height ratio | >0.50 | >0.50 |
The Cleveland Clinic notes that waist-to-height ratio may be the most practical screening metric — your waist circumference should be no more than half your height. This ratio adjusts for body frame and has been shown in research to predict cardiometabolic risk better than waist circumference alone.
BMI remains widely used but has well-documented blind spots. Studies using bioelectrical impedance and DEXA scans found that 30% of men and 46% of women classified as "healthy" by BMI were actually obese by body fat percentage.
Clinical measurement methods
CT and MRI scans are the gold standard. Both produce cross-sectional images that can directly measure visceral fat area with high accuracy. CT uses X-ray attenuation to differentiate tissue types; MRI uses magnetic fields and radio waves. Neither is practical for routine screening — they're expensive, CT involves radiation exposure, and MRI is time-consuming.
DEXA (dual-energy X-ray absorptiometry) has become the most practical clinical tool. Originally designed for bone density scanning, DEXA also separates body composition into fat mass, lean mass, and bone mineral content. It can estimate visceral fat volume with a correlation of r=0.88 against MRI. It's faster, cheaper, and uses less radiation than CT. The catch: DEXA tends to overestimate visceral fat, particularly in people with very high or very low levels. For individuals with VAT exceeding 750 cm3 (women) or 1,500 cm3 (men), the overestimation becomes clinically meaningful.
Bioelectrical impedance analysis (BIA) is the least accurate of the clinical methods, with an R-squared of only 0.27-0.49 against gold standard imaging. Consumer scales and handheld devices that claim to measure "visceral fat rating" use BIA technology. Treat these numbers as rough trends rather than precise measurements.
You can't crunch your way to less visceral fat
The idea of spot reduction — targeting fat loss in a specific body part through localized exercise — persists despite decades of evidence against it. Ab exercises strengthen the muscles underneath your belly fat, but they don't preferentially burn the fat sitting on top of them.
The counterintuitive upside: visceral fat is easier to lose than subcutaneous fat. The Cleveland Clinic confirms that visceral fat responds faster to diet and exercise changes than the stubborn subcutaneous fat around your hips and thighs. Measurable visceral fat reduction can happen in two to three months of consistent effort.
Why? The same metabolic activity that makes visceral fat dangerous also makes it vulnerable. Its high rate of lipolysis means it mobilizes readily when you create conditions that demand fat burning — particularly through exercise and caloric adjustments. Subcutaneous fat, by contrast, holds on to stored energy more stubbornly.
What the research says about reducing visceral fat
Not all exercise works equally well against visceral fat, and diet strategies affect visceral and subcutaneous fat stores differently.
Exercise: intensity matters more than duration
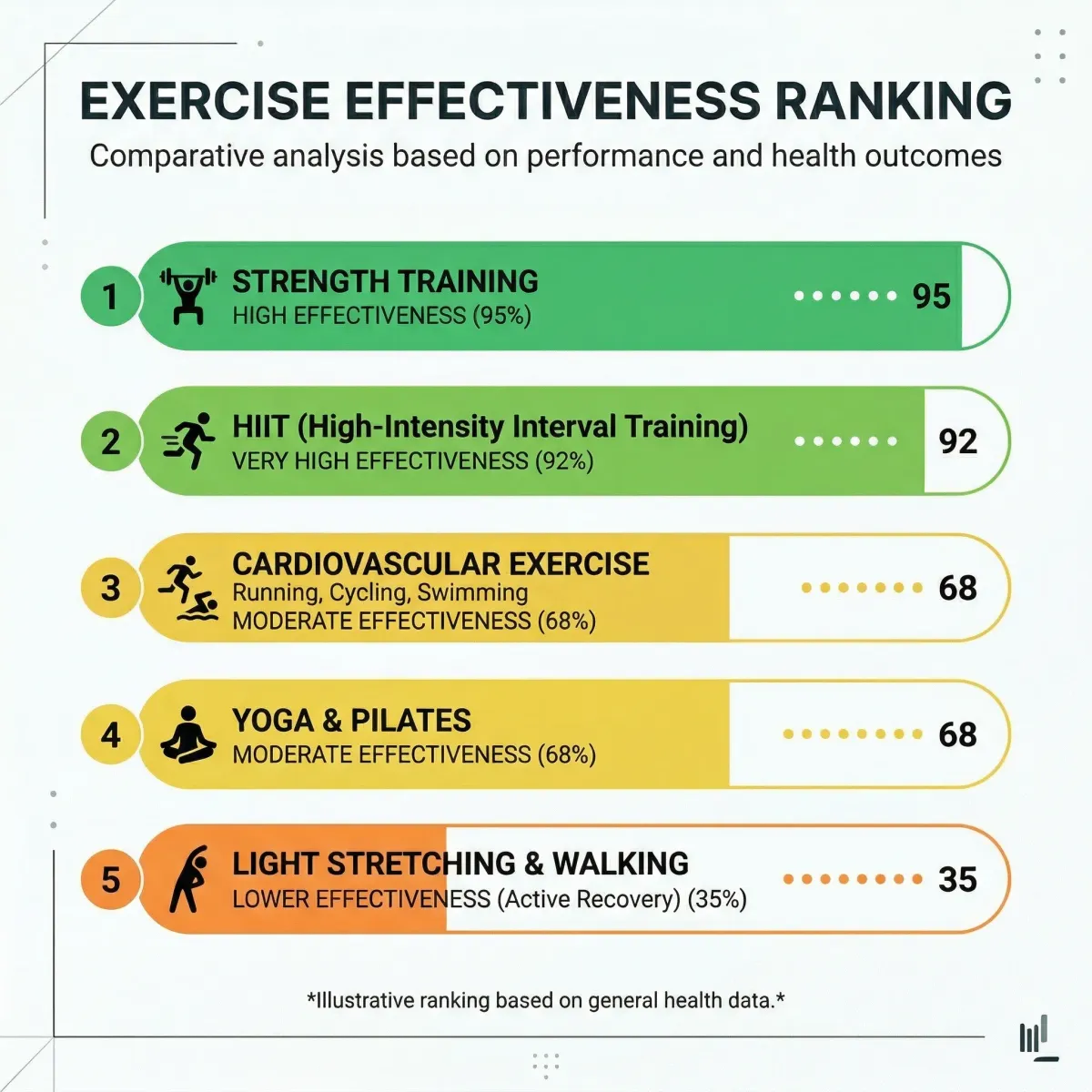
A 2024 network meta-analysis of 84 randomized controlled trials (4,836 participants) ranked exercise types by their effectiveness at reducing visceral adipose tissue. Vigorous aerobic exercise and HIIT consistently ranked highest. Resistance training alone ranked lowest for visceral fat reduction, though it still produced measurable improvements in men and people with a body fat percentage below 40%.
A separate systematic review and meta-analysis found that moderate-to-high intensity aerobic exercise reduced visceral fat by more than 30 cm2 in women and more than 40 cm2 in men on CT analysis — even without any dietary changes. After just 12 weeks. That's a clinically meaningful reduction from exercise alone.
For people already pursuing zone 2 cardio for longevity benefits, the message is clear: zone 2 builds your aerobic base, but adding periodic vigorous-intensity sessions or HIIT will produce faster visceral fat reduction.
| Exercise type | VAT reduction ranking | Key findings |
|---|---|---|
| Vigorous aerobic (70-85% HRmax) | Highest | Best probability of being #1 for VAT reduction |
| HIIT | Highest (tied) | Equally effective as vigorous aerobic in most outcomes |
| Moderate aerobic (50-70% HRmax) | Moderate | Effective but requires more time commitment |
| Combined aerobic + resistance | Moderate | Good for overall body composition |
| Resistance training alone | Lowest | Works for males and <40% BF; less effective for females |
Diet: what you eat changes where you lose fat
Johns Hopkins researchers compared low-carbohydrate and low-fat diets with identical calorie counts over six months. The low-carb group lost an average of 28.9 pounds versus 18.7 pounds in the low-fat group. Both groups lost similar amounts of lean tissue (2-3 pounds), meaning the low-carb diet produced a substantially higher percentage of fat loss.
The research also suggests specific dietary factors that directly promote visceral fat accumulation: fructose consumption is linked to VAT deposition (while glucose tends toward subcutaneous storage), ultra-processed foods are associated with age-related visceral fat growth, and saturated fatty acids promote both visceral and hepatic fat accumulation. A Mediterranean-style diet — rich in monounsaturated fats, fiber, and whole foods — addresses several of these factors simultaneously.
When diet is compared head-to-head with exercise, diet produces greater total weight loss, but exercise produces a proportionally greater reduction in visceral fat. Combining both yields the strongest results, which shouldn't surprise anyone but is worth stating plainly.
Sleep, stress, and the cortisol connection
Cortisol has a particular affinity for visceral fat cells. When cortisol stays elevated from poor sleep, chronic stress, or both, it promotes fatty acid storage in visceral adipocytes. Research on cortisol management shows that sleep quality and stress reduction have measurable effects on where your body stores fat. Seven hours of sleep minimum, according to most of the data.
Alcohol consumption also deserves mention. The "beer belly" stereotype has some basis in physiology — alcohol is calorie-dense, strains the liver (which is already dealing with portal vein FFA delivery from visceral fat), and has been independently associated with greater VAT accumulation.
Emerging pharmacological approaches
GLP-1 receptor agonists (semaglutide, liraglutide) have shown specific effects on visceral fat beyond their general weight loss benefits. Liraglutide in particular has been shown to reduce both VAT and inflammatory biomarkers in obese patients without diabetes. For people already using dietary strategies to boost GLP-1 levels naturally, the mechanism is related: GLP-1 appears to reduce visceral adipocyte inflammation directly.
Frequently Asked Questions
Can you have dangerous levels of visceral fat without looking overweight?
Yes. This is well-documented. Studies show that 30% of men and 46% of women with a "healthy" BMI are actually obese by body fat composition standards. The phenomenon is especially common in people of East and South Asian descent, where 60-80% of type 2 diabetes cases occur in people classified as non-obese. Waist circumference is a better screening tool than the scale or the mirror.
How quickly can you reduce visceral fat with exercise?
Research shows measurable reductions in as little as 12 weeks. A meta-analysis found that moderate-to-high intensity aerobic exercise reduced visceral fat by over 30 cm2 in women and over 40 cm2 in men on CT imaging — without dietary changes. Cleveland Clinic clinicians report that patients can start seeing visceral fat loss within two to three months of consistent exercise and dietary changes.
Is a DEXA scan worth it for measuring visceral fat?
DEXA provides a reasonable estimate with an r=0.88 correlation against MRI (the gold standard). It overestimates in people with very high VAT levels and underestimates in those with very low levels. For tracking trends over time, DEXA is more useful than for a single-point measurement. However, waist circumference is free, available immediately, and correlates well with cardiometabolic risk — so start there.
Does intermittent fasting specifically target visceral fat?
The Cleveland Clinic includes intermittent fasting among strategies that may help reduce visceral fat, as it encourages the body to burn stored fat. Some evidence supports that fasting-induced metabolic shifts (like those involved in autophagy) may preferentially affect visceral stores, but the evidence is less robust than for exercise intensity. The most consistent finding is that any approach creating a sustained caloric deficit will reduce visceral fat, with exercise intensity amplifying the effect.
Why is visceral fat easier to lose than subcutaneous fat?
The same metabolic activity that makes visceral fat dangerous also makes it vulnerable. Its rapid lipolysis and FFA release mean it responds quickly to interventions. When you exercise or create a caloric deficit, visceral fat mobilizes faster because its adipocytes are already primed for rapid turnover. Subcutaneous fat cells hold onto stored triglycerides more tenaciously.
Related Articles
- Inflammation and Chronic Disease: A Complete Guide to Anti-Inflammatory Living — Chronic inflammation is one of the primary mechanisms through which visceral fat drives disease.
- Zone 2 Cardio for Fat Burning and Longevity — Low-intensity aerobic exercise builds the foundation, but you'll need higher intensity for maximum visceral fat reduction.
- Akkermansia: The Next-Generation Probiotic for Metabolic Health — Gut microbiome composition influences metabolic health and may play a role in visceral fat accumulation.
- Resistant Starch: The Cheap Gut Health Hack for Blood Sugar and Metabolism — Blood sugar management is directly linked to insulin sensitivity and fat storage patterns.
- Autophagy: How to Trigger It Through Fasting, Exercise, and Diet — Fasting and exercise trigger cellular recycling processes that may complement visceral fat reduction strategies.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











