
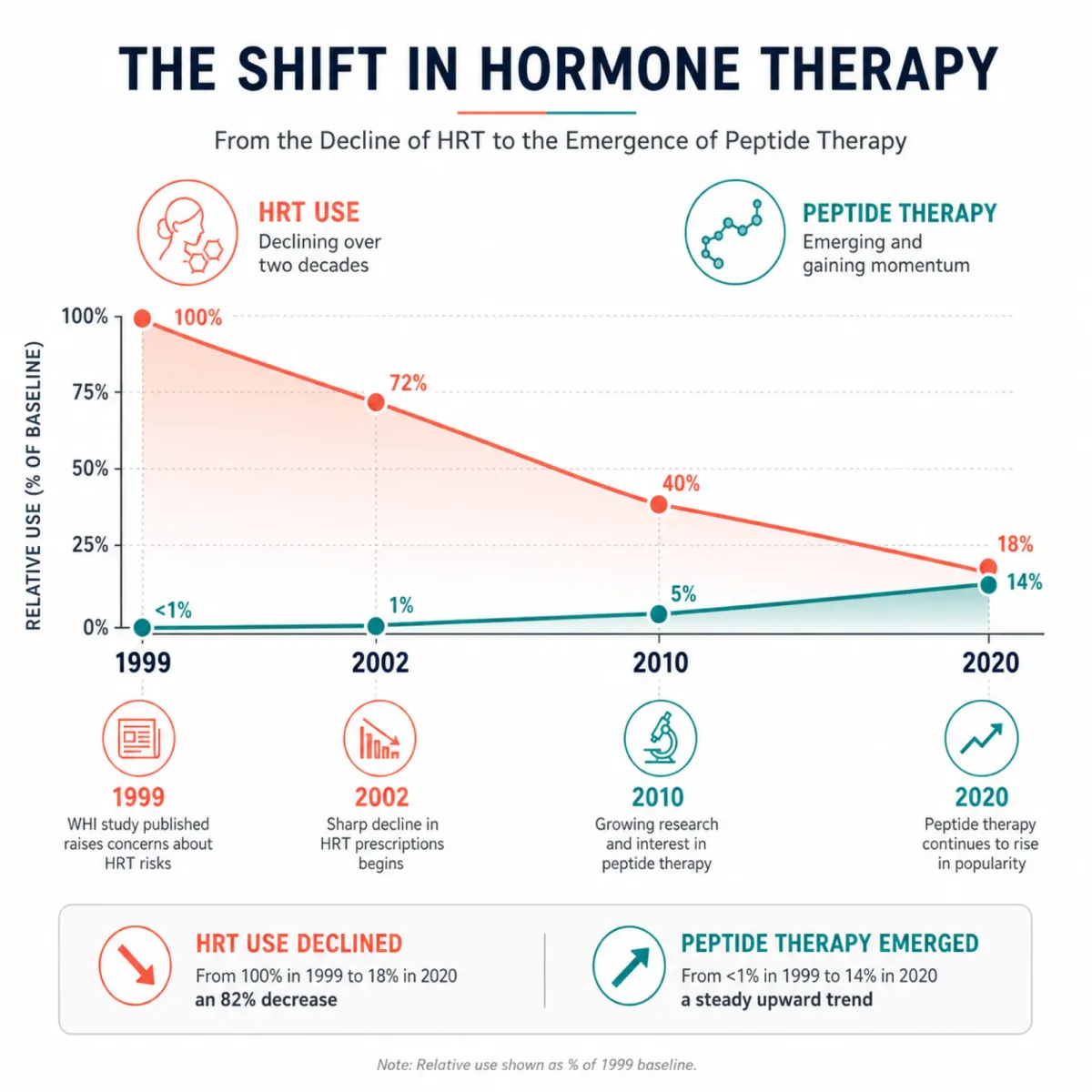
The 82% drop that reshaped how women think about menopause treatment
Between 1999 and 2020, menopausal hormone therapy use in the United States fell from 26.9% to 4.7% — a collapse driven almost entirely by the 2002 Women's Health Initiative trial, which suggested that HRT's health risks exceeded its benefits for chronic disease prevention. Among women aged 52 to 65, the decline was even steeper: an 88% prevalence reduction, from 34.9% down to 4.5%.
That fear never fully receded, even as subsequent analysis reframed the WHI findings. The 2022 NAMS position statement reaffirmed that hormone therapy remains the most effective treatment for vasomotor symptoms and genitourinary syndrome of menopause. The 2025 Korean Menopause Society guidelines put numbers on it: standard-dose MHT achieves roughly 75% reduction in hot flashes, and low-dose regimens still manage about 65%.
So why are women still looking elsewhere? Because perimenopause does not announce itself with a single symptom. It arrives as a tangle of sleep disruption, joint aches, brain fog, gut issues, declining libido, and anxiety that can precede the last menstrual period by a decade. HRT addresses the estrogen deficit at the center of that storm, but it does not touch the parallel decline in growth hormone, the gut-brain axis disruptions, or the neurological circuits governing desire and mood. Peptide therapy has entered that gap.
One caveat that shapes everything below: no peptide is FDA-approved for menopause symptom management. No completed human RCT has studied any peptide compound specifically as an adjunct to HRT in menopausal women. What follows is a report on what clinicians and patients are actually doing, grounded in what evidence exists for each compound — not a recommendation to replace a treatment that decades of data support.
CJC-1295/Ipamorelin: the growth-hormone duo clinics prescribe most
Growth hormone production drops roughly 14% per decade after age 30. Perimenopause accelerates that slide because estrogen and growth hormone share overlapping regulatory pathways. By the time a woman hits her mid-40s, she may be dealing with what endocrinologists call a "dual hormonal decline" — falling estrogen and falling GH simultaneously. HRT only addresses one of them.
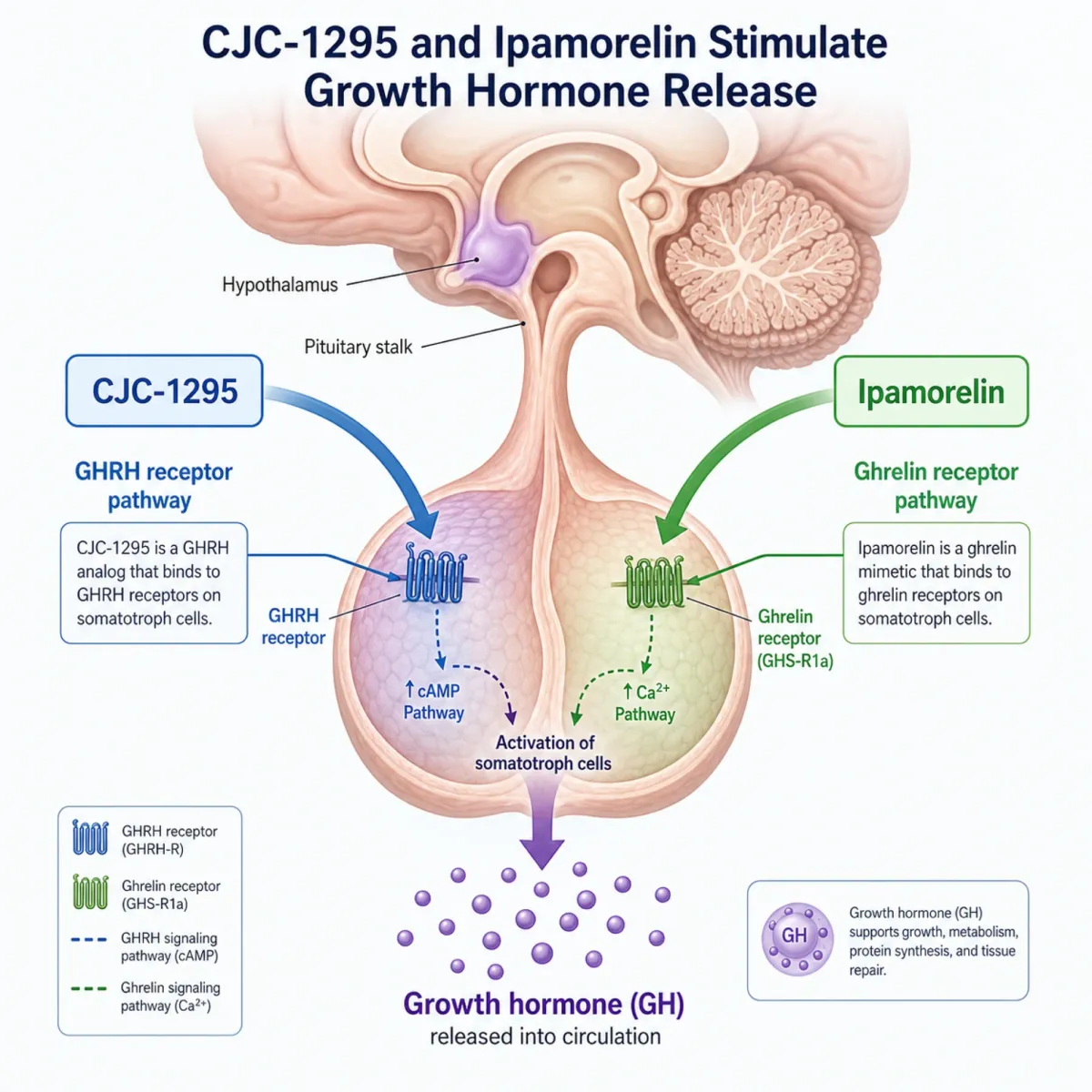
CJC-1295 is a synthetic analog of growth-hormone-releasing hormone (GHRH). Ipamorelin mimics ghrelin and signals the pituitary to release GH through a separate receptor. Combine them and you get a two-pronged stimulus. A 2006 study published in the Journal of Clinical Endocrinology and Metabolism showed that CJC-1295 produced sustained, dose-dependent increases in GH and IGF-1, with mean GH concentrations rising 2- to 10-fold and remaining elevated for six or more days.
Clinics promoting the combination report that patients see improved sleep quality and body composition over a 3-to-6-month protocol. The GH surge happens primarily during deep sleep, which is why many providers instruct evening dosing — the peptide piggybacks on the body's natural nocturnal GH pulse rather than overriding it.
The risks are real. Elevated IGF-1 levels are associated with increased cancer risk, particularly breast and colorectal cancers. The FDA has warned of immunogenicity and cardiovascular effects including increased heart rate. One clinical trial of CJC-1295 was discontinued after a participant's death. And as of April 2026, the FDA Pharmacy Compounding Advisory Committee recommended against including CJC-1295/Ipamorelin on the 503A bulk drug substances list, which could restrict compounding access going forward.
For a perimenopausal woman whose sleep has cratered and whose body composition has shifted despite consistent exercise, this combination targets something HRT cannot. But the cancer risk question has no satisfying answer yet, and the regulatory ground is shifting under this peptide as you read this.
BPC-157: the stomach-derived peptide that keeps showing up in clinic protocols
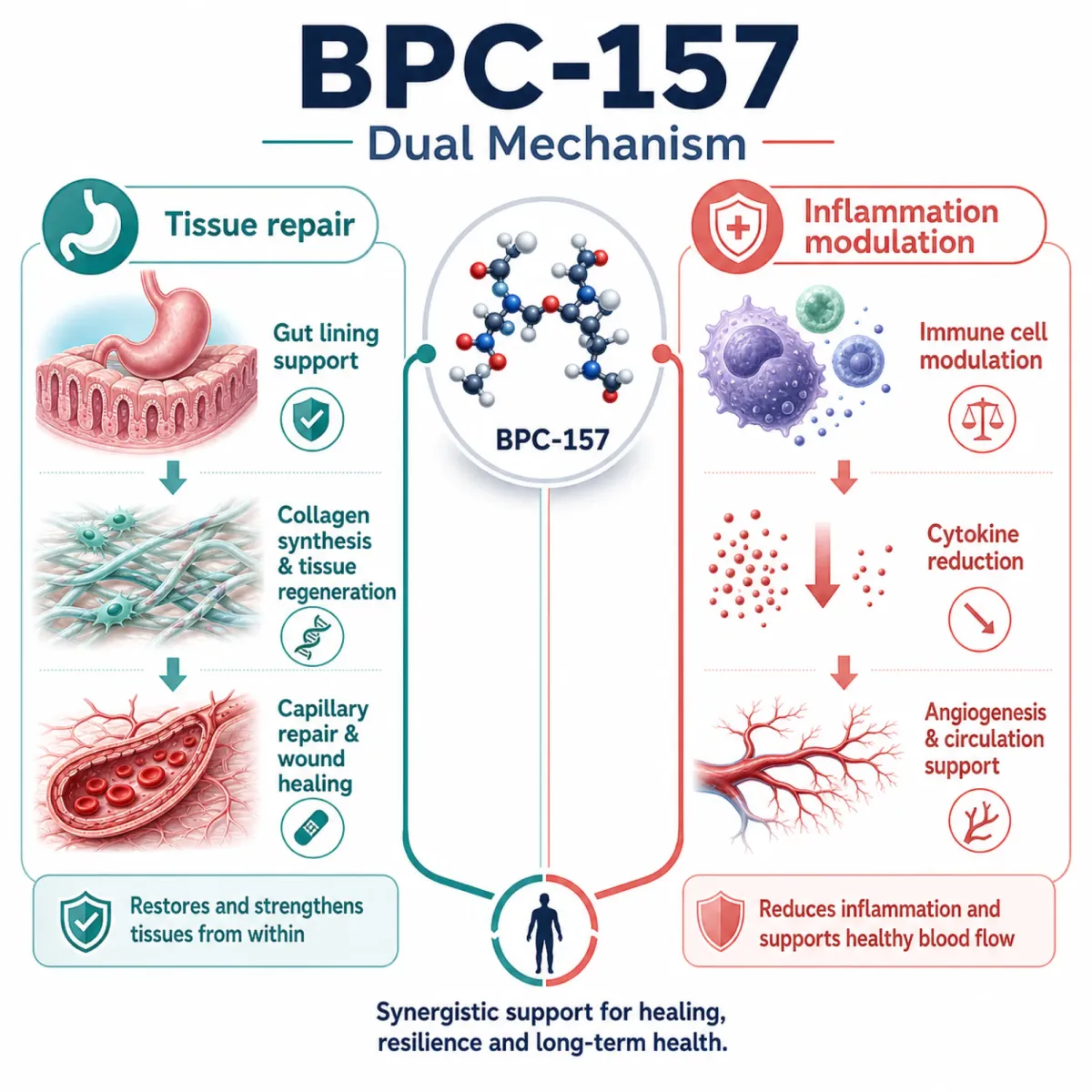
Perimenopause has a gut problem that does not get enough attention. Estrogen receptors line the GI tract, and as estrogen fluctuates, women report new-onset bloating, food sensitivities, and inflammatory bowel symptoms that their gastroenterologists struggle to explain. BPC-157 — a 15-amino-acid peptide originally isolated from human gastric juice — has become the peptide that functional medicine practitioners reach for when gut complaints accompany the hormonal transition.
The preclinical record is large. A review in Current Neuropharmacology documented that BPC-157 heals esophageal, gastric, duodenal, and intestinal lesions, recovers sphincter function, counteracts NSAID-mediated damage, and maintains GI mucosal integrity through what the authors describe as Robert's cytoprotection. The same paper reported that toxicity has not been observed in the research reviewed.
BPC-157 gets more interesting below the gut. Administered peripherally, it induces the release of serotonin in specific brain nigrostriatal regions and influences both dopaminergic and serotonergic systems. It repairs the gut lining while nudging the neurotransmitter systems that govern mood, two problems that travel together during perimenopause.
The honesty check: no clinical trials of BPC-157 in menopausal women exist. A 2024 systematic review in the American Journal of Sports Medicine concluded that clinical data remain limited and in-human safety is unknown. As of February 2026, BPC-157 is not eligible for 503A compounding, meaning no lawful U.S. compounding pathway exists. Women still obtain it through research-chemical channels, raising purity and dosing concerns.
Kisspeptin: the upstream signal that perimenopause scrambles
Every other peptide on this list works downstream — boosting growth hormone, repairing tissue, triggering desire circuits. Kisspeptin operates at the top of the cascade. It functions as what researchers call a "master switch" for the hypothalamic-pituitary-gonadal (HPG) axis, the hormonal command chain that governs GnRH release and, downstream, LH and FSH production.
The perimenopause connection: as estrogen declines, the inhibitory feedback on kisspeptin neurons is removed. The result is elevated kisspeptin and erratic GnRH pulsatility — a misfiring thermostat in the hypothalamus. Researchers believe this dysregulated kisspeptin signaling is a driver of hot flashes, not merely a bystander. The hypothalamus, struggling to interpret wildly variable estrogen signals, overreacts to temperature cues.
Kisspeptin research is promising but firmly in the academic phase. No menopause-specific randomized controlled trial has been published. The compound is not available through U.S. compounding for this indication, and there is no USP monograph establishing compounding eligibility. Women cannot walk into a clinic and request kisspeptin therapy the way they can with CJC-1295 or BPC-157.
The distinction matters: HRT replaces the estrogen that is missing, while kisspeptin research asks whether you can stabilize the brain's response to declining estrogen instead. That could eventually yield treatments for women who cannot or will not take hormones. We will cover kisspeptin's hot-flash-specific research in a forthcoming piece — for now, it is the most mechanistically interesting peptide on this list and the furthest from clinical availability.
PT-141: the only peptide here with Phase 3 trial data and an FDA nod
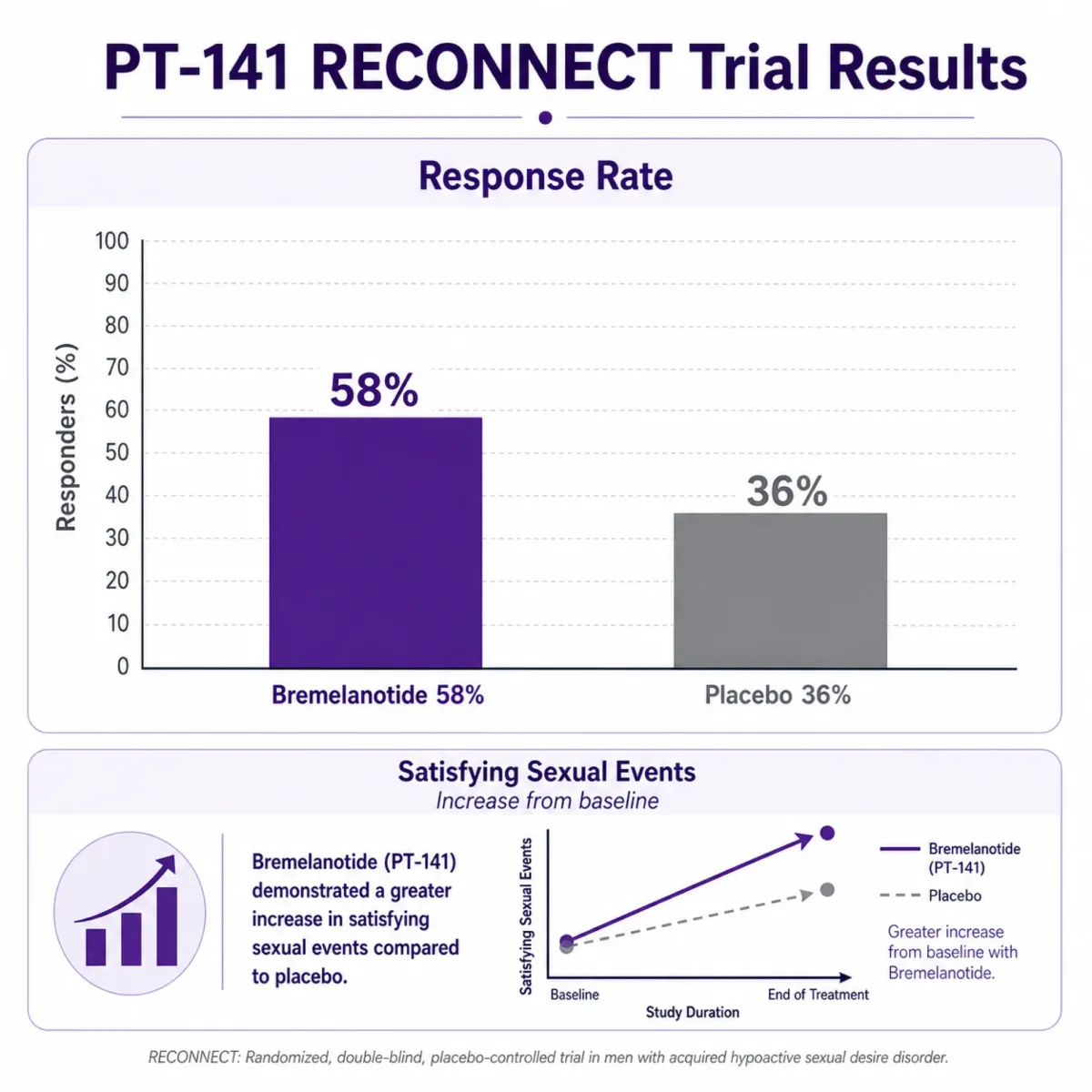
Every other peptide in this article operates in regulatory gray zones. PT-141 (bremelanotide, brand name Vyleesi) is different: it received FDA approval in 2019 for hypoactive sexual desire disorder in premenopausal women. That approval was built on actual large-scale clinical trials, not animal models or case series.
The RECONNECT Phase 3 trials enrolled approximately 1,247 premenopausal women with confirmed HSDD. The results: response rates of 58.3% and 58.2% for bremelanotide versus 36.1% and 35.4% for placebo, with satisfying sexual events increasing over twofold compared to placebo. An earlier Phase 2b dose-finding trial at 67 U.S. and Canadian sites found that the 1.75mg dose produced a statistically significant improvement in Female Sexual Function Index scores (p=0.0017) and a meaningful reduction in sexual distress (p=0.0014).
The mechanism is what separates PT-141 from hormonal approaches. It activates melanocortin receptors (primarily MC4R) in the hypothalamus, increasing dopamine release to brain regions regulating sexual motivation. HRT optimizes the tissue environment — vaginal health, blood flow, estrogen-mediated sensitivity. PT-141 works upstream of all that, in the desire circuits themselves. As one clinical resource puts it, it addresses the neurological component of desire that hormone therapy alone cannot reach.
Side effects are the trade-off. Nausea affects roughly 40% of users (versus 1.3% on placebo), flushing hits 20.3%, and headaches occur in 11.3%. Mean blood pressure increases of 3 to 6 mmHg are transient but make the drug contraindicated for women with uncontrolled hypertension. The recommended dose is 1.75mg subcutaneous injection at least 45 minutes before anticipated activity, with a maximum of eight doses per month.
The catch for perimenopausal women: clinical trials enrolled premenopausal participants. Approved treatments remain limited for postmenopausal HSDD, and PT-141 during the menopausal transition is technically off-label. Clinicians prescribe it anyway, reasoning that desire circuits do not change with menopausal status. The evidence gap is smaller than for any other peptide here, but it exists.
Selank: the Russian-developed peptide tackling perimenopausal anxiety without sedation
Anxiety during perimenopause is not garden-variety stress. Fluctuating estrogen directly disrupts GABA signaling in the brain, and women who never experienced clinical anxiety before their 40s suddenly find themselves unable to sleep, unable to quiet racing thoughts, and unable to explain why. Benzodiazepines work but carry dependence risk. SSRIs take weeks to reach efficacy. Selank occupies a different pharmacological niche.
Selank is a synthetic heptapeptide derived from human immunoglobulin G, developed at the Russian Academy of Sciences. Research published in Behavioural Brain Research found that its anxiolytic effect is comparable to low doses of benzodiazepine tranquilizers, but without sedation, muscle relaxation, tolerance development, or withdrawal syndrome. In a 14-day chronic stress model, rats receiving Selank combined with diazepam showed time in open arms 8.9 times higher than saline controls, suggesting the peptide enhances anxiolytic activity without amplifying the downsides.
The molecular story explains the clinical interest. A gene expression study in Frontiers in Pharmacology found that Selank altered the expression of 45 genes involved in neurotransmission within one hour of administration, including GABA receptor subunits that showed dramatic 20-fold changes. The peptide also modulates dopamine and serotonin receptors. Notably, hypocretin (orexin) gene expression increased 128.3-fold at three hours — a finding that may explain why Selank users report improved sleep quality without daytime drowsiness, since orexin regulates the sleep-wake boundary.
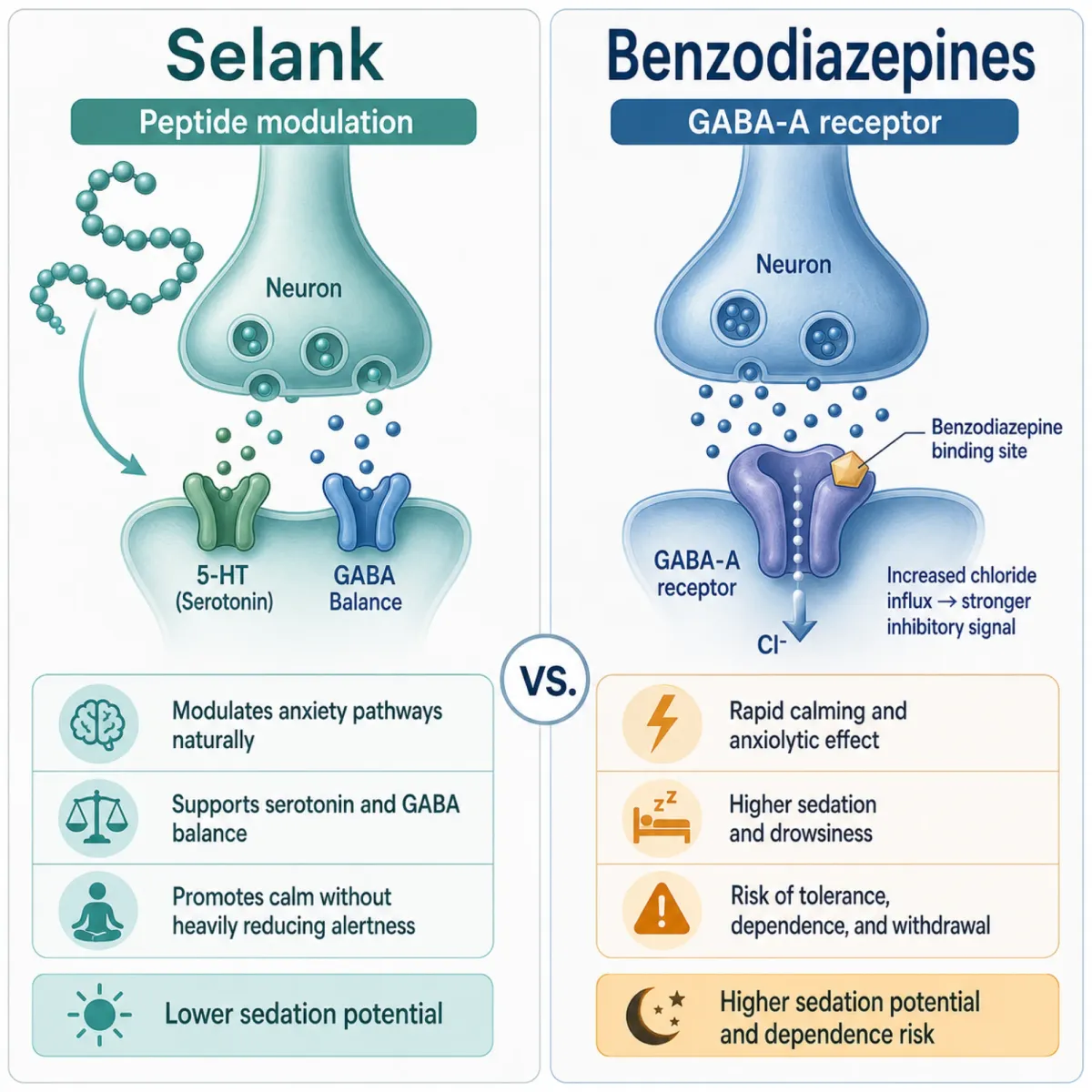
Selank works allosterically on GABA-A receptors rather than binding directly — a mechanism more like fine-tuning a radio dial than slamming a volume knob. This likely explains the absence of tolerance and withdrawal that plague benzodiazepine users.
The limitations are familiar: most research is preclinical. Selank is approved in Russia as a prescription anxiolytic but has not undergone FDA review. It is administered intranasally, which makes it more accessible than injectables, but sourcing reliable formulations outside Russian pharmacies is difficult. The mechanistic fit for perimenopausal GABA disruption is compelling. The evidence trail is not.
Where peptides fill gaps — and where they fall flat
Grouping these five peptides against standard HRT reveals a clear pattern: peptides target specific symptoms through specific mechanisms, while HRT addresses the root hormonal deficiency broadly. Neither approach covers the full perimenopausal experience alone.
| Symptom | HRT effectiveness | Peptide option | Evidence level |
|---|---|---|---|
| Hot flashes/night sweats | 75% reduction (standard dose) | Kisspeptin (theoretical) | No human RCT |
| Body composition changes | Indirect (estrogen preserves lean mass) | CJC-1295/Ipamorelin | Phase 2 in aging adults; no menopause RCT |
| GI disruption/inflammation | Not addressed | BPC-157 | Animal studies only; no human menopause trials |
| Low libido/desire | Partial (tissue health, not desire circuits) | PT-141 (Bremelanotide) | Phase 3 RCT; FDA-approved for premenopausal HSDD |
| Anxiety/mood disruption | Partial (estrogen stabilizes GABA indirectly) | Selank | Animal studies; approved in Russia only |
| Bone loss | 4.5% lumbar spine improvement (WHI) | None directly | N/A |
| Genitourinary syndrome | Gold standard | None directly | N/A |
The 2025 Menopausal Hormone Therapy Guidelines provide the context that peptide advocates sometimes omit. Standard-dose HRT improved bone mineral density by 4.5% at the lumbar spine and 3.7% at the femoral neck in the WHI study. Women who initiated MHT within 10 years of menopause saw a 32% risk reduction in coronary artery disease. These are large-scale, replicated findings. No peptide on this list has anything comparable.
Dr. Eric Topol, writing in his Ground Truths newsletter, was blunter: there is "no evidence from randomized trials in humans that any of these peptides provide the benefits that are advocated." He notes that growth hormone peptides like CJC-1295 and Ipamorelin carry a potential cancer risk through broad cell growth induction, and that BPC-157's pro-angiogenic properties raise theoretical concerns about tumor promotion.

Women gravitating toward peptides are often dealing with symptoms HRT does not fully address: gut issues, vanished libido despite adequate estrogen, anxiety that SSRIs flatten rather than resolve. The responsible approach is not replacement but layering: optimize HRT first, then consider targeted peptides for residual symptoms under medical supervision.
The bottom line: HRT remains the evidence-backed foundation for perimenopausal symptom management. Peptides may eventually earn a role as targeted adjuncts for symptoms HRT misses, but only PT-141 has Phase 3 trial data behind it. The other four operate on preclinical promise, regulatory uncertainty, and the desperation of women whose symptoms outpace what conventional medicine currently offers.
Frequently Asked Questions
Can peptides actually replace HRT during perimenopause?
Not based on current evidence. Both the NAMS 2022 position statement and the 2025 Menopause Society guidelines confirm HRT remains the most effective treatment for vasomotor symptoms and genitourinary syndrome. No peptide has been tested in a menopause-specific RCT. Women are using them as targeted complements for symptoms HRT misses, not as direct replacements.
Which of these five peptides has the strongest clinical evidence?
PT-141 (bremelanotide), by a wide margin. It has Phase 3 trial data from the RECONNECT trials (~1,247 premenopausal women) and FDA approval for HSDD. The other four rely on preclinical research or mechanistic data without large-scale human validation.
Are peptides safe to use alongside hormone therapy?
No clinical trial has studied any peptide as an HRT adjunct in menopausal women. The main concern is CJC-1295/Ipamorelin's potential to elevate IGF-1, which is associated with increased breast and colorectal cancer risk. Any combination should be supervised by a physician who can monitor relevant biomarkers.
Why is BPC-157 increasingly difficult to obtain legally?
The FDA has progressively tightened BPC-157's regulatory status. It was classified as a Category 2 bulk drug substance, and as of February 2026, it is not eligible for 503A compounding, meaning there is no lawful U.S. compounding pathway. Women still obtain it through research-chemical suppliers, but those products lack pharmaceutical-grade quality controls and carry unknown purity risks.
What should a perimenopausal woman try before considering peptides?
The physician perspective from multiple sources in our research is consistent: optimize foundational health first. That means adequate sleep, nutrition, exercise, and stress management. Then evaluate whether HRT is appropriate with a qualified provider. Peptides should be considered only after those foundations are in place and specific residual symptoms remain — and only under medical supervision with realistic expectations about the evidence gaps.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











