
What separates anxiety from everyday stress
Everyone feels stressed. A work deadline, a financial surprise, a difficult conversation with a friend. These situations produce real physical tension that fades once the situation passes. That's your nervous system working as intended.
Anxiety is a different animal. According to the American Psychological Association, clinical anxiety persists even when there's no identifiable external threat. The worry keeps running after the exam is over, after the bill is paid, after the conversation ended hours ago. The DSM-5-TR sets a specific diagnostic threshold: for generalized anxiety disorder (GAD), you need excessive worry occurring more days than not for at least six months.
About 359 million people worldwide meet criteria for an anxiety disorder, making it the single most common class of mental health condition on the planet. The difference between normal stress and a clinical problem isn't just intensity. It's persistence, proportion, and how much it interferes with your ability to function at work, in relationships, and in daily life.
Quick fact: The DSM-5-TR and ICD-11 both classify anxiety disorders as distinct clinical conditions, not personality traits or emotional weaknesses. They involve measurable changes in brain chemistry and nervous system function.
Seven signs your stress has crossed the line
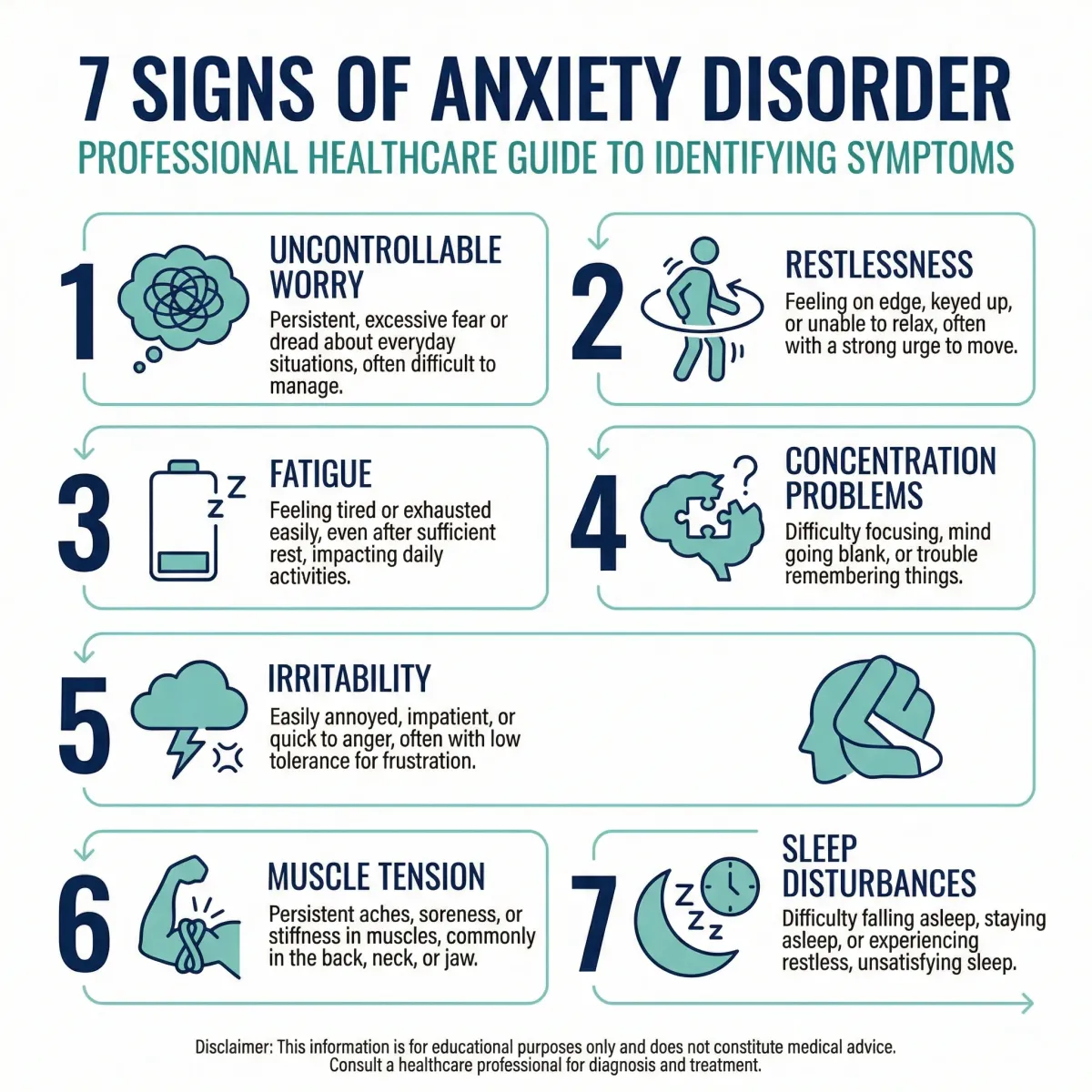
The American Psychiatric Association identifies seven primary markers that separate clinical anxiety from ordinary stress. If several of these have been present for months and are disrupting your daily life, it may be time to talk to a doctor.
1. Worry that won't shut off. Not the productive kind that helps you prepare. This is cyclical, repetitive thinking about finances, health, work, or family that you recognize as out of proportion but can't stop. Your brain runs worst-case scenarios on repeat.
2. Feeling "keyed up" or on edge. A persistent internal restlessness that goes beyond feeling a bit nervous. You can't sit still, you fidget constantly, and you have an unshakeable sense that something bad is about to happen. Your nervous system is stuck on high alert, scanning for threats that aren't there.
3. Fatigue that doesn't match your activity level. This one surprises people. Maintaining constant neurological hypervigilance burns through energy. The continuous output of stress hormones and the cognitive effort of managing intrusive thoughts leave you drained even when you haven't done much physically.
4. Concentration problems or your mind going blank. Anxiety hijacks working memory. Because your brain is busy running threat-detection routines in the background, it struggles to focus on the conversation in front of you, the paragraph you're reading, or the task at hand. During acute anxiety, your mind can go completely blank.
5. Irritability with a short fuse. When your nervous system is already running at maximum capacity, even minor things trigger disproportionate reactions. A loud noise, a small inconvenience, or a casual question from a family member can set off a response that feels out of character.
6. Chronic muscle tension. Anxiety is a whole-body condition. Your brain sends sustained "fight or flight" signals that keep muscles contracted. Because the perceived threat never resolves, the tension never releases. Over months and years, this shows up as chronic neck, shoulder, and back pain, and often jaw clenching or teeth grinding.
7. Sleep disturbances. Racing thoughts make it hard to fall asleep. Even when you do sleep, it tends to be shallow and unrefreshing. The brain can't clear metabolic waste or reset emotional circuits properly, which means you wake up more anxious than when you went to bed. If sleep has become a struggle, evidence-based sleep strategies can help alongside professional treatment.
Why anxiety hurts: the physical toll
Anxiety gets mischaracterized as a purely emotional problem. It isn't. When chronic anxiety takes over the brain's command center, the downstream effects hit multiple organ systems. This is why so many people with undiagnosed anxiety first show up at an emergency room convinced they're having a heart attack or a neurological event.
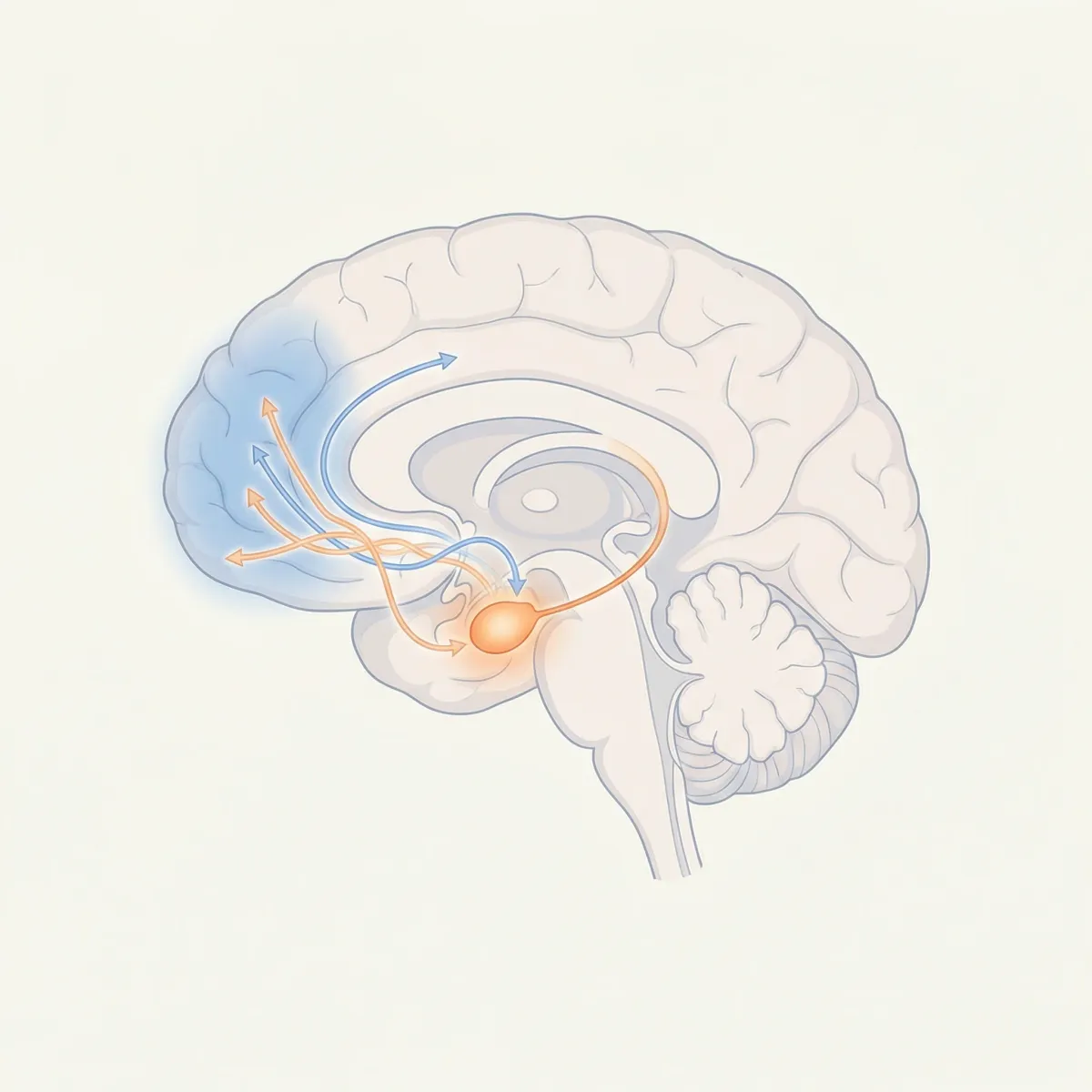
The chain reaction starts in the amygdala, an almond-shaped structure deep in the brain that processes threat signals. When the amygdala fires, it sends a distress signal to the hypothalamus, which triggers the hypothalamic-pituitary-adrenal (HPA) axis. This releases cortisol and adrenaline throughout the body. In a healthy stress response, a feedback loop shuts this down once the threat passes. In clinical anxiety, the feedback loop is broken. The system stays activated.
| Symptom type | What it looks like | What's driving it |
|---|---|---|
| Physical | Muscle tension, tremors, fatigue, headaches, stomach problems (nausea, IBS), rapid heartbeat, hyperventilation, sweating, numbness or tingling | Chronic HPA axis activation; elevated cortisol and adrenaline; altered vagal tone and blood flow diversion from the gut |
| Cognitive | Difficulty concentrating, memory problems, mind going blank, catastrophic thinking, rumination, hypervigilance | Disrupted connectivity between the prefrontal cortex and amygdala; working memory overload |
| Emotional | Sense of dread, irritability, feelings of impending doom, emotional numbness, feeling detached from reality | Hyperactive amygdala; depleted serotonin and GABA levels |
The cardiovascular strain is real. Persistent adrenaline surges cause elevated heart rate and blood vessel constriction. Hyperventilation throws off your blood oxygen-CO2 balance, producing dizziness and tingling in your hands and face. The gut takes a hit too: the gut-brain axis means chronic anxiety commonly produces nausea, cramping, and a high overlap with irritable bowel syndrome. Over time, this accumulated biological wear increases your risk for cardiovascular disease, hypertension, and metabolic problems.
The worry trap: why your brain won't let go
Here's a genuine paradox: if worry feels terrible, why do anxious brains do it constantly? If you've ever told yourself "stop worrying" and found it completely useless, the Contrast Avoidance Model developed by researchers Michelle Newman and Sandra Llera explains why.
The theory works like this: people with chronic anxiety aren't just afraid of bad things happening. They're terrified of the emotional whiplash of being caught off guard. Feeling happy or relaxed and then being hit with bad news is, for the anxious brain, worse than the bad news itself. So the brain uses worry to keep you at a steady baseline of mild misery. If you're already braced for the worst, nothing can blindside you.
This creates a self-reinforcing loop. If something bad does happen, you feel validated ("see, I was right to worry"). If nothing bad happens, you feel relief, and your brain credits the worrying for preventing the disaster. Either way, the worry gets reinforced. Recent clinical research confirms this mechanism isn't limited to GAD. It shows up in depression-related rumination and social anxiety avoidance patterns too.
Brain imaging studies of people caught in severe worry show something specific: the prefrontal cortex, which normally acts as a brake on the amygdala's alarm signals, fails to do its job. The amygdala stays hyperactive. The logical brain can't shut off the emotional alarm. That's not a character flaw. It's a measurable circuit malfunction.
When perfectionism and procrastination hide the real problem
Avoidance is how anxiety does its real damage to your life. In social anxiety, avoidance looks obvious: skipping events, dreading phone calls. But in generalized anxiety, avoidance wears a much better disguise.
Procrastination is one of them. It gets labeled as laziness, but clinical research shows it's often anxiety-driven avoidance. You don't start the project because the fear of doing it badly is so overwhelming that not starting at all provides temporary emotional relief. Of course, the deadline still comes, and the resulting panic makes the next project even harder to begin.
Then there's "high-functioning anxiety." It's not a formal DSM diagnosis, but clinicians at New York-Presbyterian and Mayo Clinic describe it as a recognizable pattern: outwardly successful people who are internally falling apart. The perfectionism, the over-preparation, the obsessive organization aren't signs of ambition. They're control strategies driven by fear. Beneath the achievements, there's constant racing thoughts, an inability to relax, and severe muscle tension.
To screen for anxiety severity, clinicians use the GAD-7 scale, a seven-question self-assessment covering the past two weeks.
| GAD-7 score | Severity | What it means |
|---|---|---|
| 0-4 | Minimal | Within normal range. No clinical intervention needed. |
| 5-9 | Mild | Monitor symptoms. Consider lifestyle changes and stress management. |
| 10-14 | Moderate | Likely clinically significant. A score of 10+ has 89% sensitivity and 82% specificity for identifying GAD. |
| 15-21 | Severe | Active treatment strongly recommended. Indicates significant distress and functional impairment. |
Is anxiety written in your DNA?
Anxiety doesn't have a single cause. It sits at the intersection of genetics, brain chemistry, and life experience.
Large-scale twin studies and genome-wide association studies estimate heritability at 30% to 60%. That means roughly half your risk comes from your genetic makeup. But there's no single "anxiety gene." The architecture is polygenic: hundreds or thousands of small genetic variations each contribute a tiny amount of risk. Many of these same variants overlap with genes linked to depression, insomnia, and neuroticism, which explains why these conditions so frequently travel together.
| Disorder | Estimated heritability | Notable genetic characteristics |
|---|---|---|
| Generalized Anxiety Disorder | 32-40% | High genetic overlap with major depression. In women, shared family environment also contributes. |
| Panic Disorder | 40-43% | Strongest familial clustering among anxiety subtypes. |
| Specific Phobias | 40-60% | Blood-injury phobias show highest heritability (up to 60%). Animal phobias are lower (~45%). |
| Social Anxiety Disorder | 28-40% | Genetics influence baseline behavioral inhibition. Environmental factors like childhood bullying interact heavily. |
These genetic predispositions shape how your brain's chemical systems operate. GABA, the brain's primary calming neurotransmitter, is often underactive in people with anxiety disorders. Without enough GABA signaling, the brain can't apply the brakes on fear responses. Meanwhile, variations in serotonin transporter genes (specifically the 5-HTTLPR polymorphism) are linked to increased amygdala reactivity when someone faces stress. Genetics loads the vulnerability. Environment pulls the trigger.
The epidemic most people never treat
The individual suffering is bad enough. The population-level numbers are staggering. According to the WHO's 2024 Mental Health Atlas, anxiety disorders affect approximately 4.4% of the global population. Women are diagnosed at significantly higher rates than men. And unlike many chronic diseases that appear in middle age, anxiety typically takes hold early: the average age of onset is about 21, with some subtypes emerging before age 15. That means the disorder disrupts education, career formation, and relationship development during the years that matter most.
The economic cost is staggering. The WHO and The Lancet estimate that depression and anxiety together cost the global economy $1 trillion annually, mostly through lost productivity rather than direct medical costs. People miss work. People show up but can't perform. People drop out of the workforce entirely. Without intervention, projections put the total cost of all mental disorders at $16 trillion by 2030.
Despite all this, only about 1 in 4 people with an anxiety disorder receives appropriate treatment. The reasons are familiar: underfunded mental health systems, too few trained professionals, and persistent stigma that tells people they should just "toughen up." For practical tools to manage symptoms between appointments, our guide to daily mental health management covers evidence-based approaches.
What actually works: treatments backed by evidence
In 2023, the U.S. Preventive Services Task Force recommended routine anxiety screening for all adults under 65 in primary care settings. This was a major shift. Because anxiety so often presents as physical symptoms, your family doctor may be the best person to catch it early.
Once identified, treatment rests on two pillars:
Cognitive Behavioral Therapy (CBT) remains the gold standard. Meta-analyses consistently show long-term effectiveness that matches or beats medication. CBT works by dismantling the thought patterns that sustain anxiety. You learn to identify catastrophic thinking, challenge it with evidence, and gradually face feared situations through exposure therapy. The brain literally rewires: the prefrontal cortex regains its ability to regulate the amygdala's alarm signals. Breathing techniques and meditation practices can supplement formal therapy as daily coping tools.
Medication is effective when symptoms are severe enough to prevent engagement with therapy. SSRIs (like sertraline and escitalopram) and SNRIs (like venlafaxine and duloxetine) are the first-line pharmacological treatments. They increase serotonin and norepinephrine availability in the brain, gradually reducing amygdala hyperactivity over several weeks. These medications are not addictive. Benzodiazepines (Xanax, Valium) are a different story: they work fast but carry significant dependence risk and are now reserved for short-term crisis management only.
Key takeaway: CBT and SSRIs/SNRIs both show moderate-to-large effect sizes for GAD, social anxiety, and panic disorder. The best outcomes often combine both approaches, tailored to the individual.
Common anxiety myths vs. clinical reality
| Myth | Clinical reality |
|---|---|
| Anxiety is just an overreaction or personal weakness | Anxiety disorders involve measurable brain circuit changes, HPA axis dysregulation, and genetically mediated neurotransmitter disruptions. They don't discriminate by personality type. |
| Avoiding stressful situations is the best way to cope | Avoidance reinforces the brain's false belief that the avoided situation was genuinely dangerous. Exposure-based therapies deliberately reverse this pattern and are among the most effective treatments available. |
| Anxiety will eventually go away on its own | Untreated anxiety is chronic and rarely remits spontaneously. Without treatment, long-term cortisol elevation worsens both the psychiatric condition and physical health. |
| Psychiatric medication is dangerous and addictive | First-line anxiety medications (SSRIs, SNRIs) are not chemically addictive. They carry different risks than benzodiazepines, which are the class actually associated with dependence. CBT alone is also highly effective. |

Frequently Asked Questions
What is the difference between a panic attack and an anxiety attack?
A "panic attack" is a specific clinical event defined in the DSM-5-TR: an abrupt surge of intense fear that peaks within minutes, with symptoms like pounding heart, shortness of breath, chest pain, and a terrifying sense of losing control. Panic attacks can occur without any obvious trigger. "Anxiety attack" is a colloquial term (not a formal diagnosis) that people use to describe prolonged periods of severe worry and physical tension, usually tied to an anticipated event or situation.
Can caffeine cause or worsen anxiety?
Yes. Caffeine is a central nervous system stimulant that blocks adenosine receptors and promotes adrenaline release. Clinical evidence shows a dose-dependent anxiogenic effect: consuming more than 400 mg daily (roughly four cups of coffee) can trigger tachycardia, restlessness, and insomnia, and may precipitate panic attacks in people who are biologically vulnerable.
How is "high-functioning anxiety" different from GAD?
"High-functioning anxiety" isn't a formal DSM diagnosis. It describes people who meet the internal criteria for an anxiety disorder but maintain outward success through exhaustive perfectionism, chronic over-preparation, and obsessive control strategies. Unlike typical GAD presentations where impairment is visible (job loss, social withdrawal), high-functioning anxiety hides behind a facade of competence while the person suffers from racing thoughts, sleep problems, and constant tension.
Are anxiety disorders inherited from parents?
Anxiety carries a significant genetic component, with twin studies estimating heritability between 30% and 60%. There is no single "anxiety gene." The risk comes from hundreds of small genetic variants that combine to create neurobiological vulnerability. This inherited blueprint then interacts with environmental factors (chronic stress, childhood adversity, major life events) to trigger the actual onset of the disorder.
When should someone seek professional help for anxiety?
If anxiety symptoms have persisted for several months, are difficult to control, and are interfering with work, relationships, sleep, or daily activities, it's time to see a healthcare provider. A GAD-7 score of 10 or above during screening is a strong indicator. The U.S. Preventive Services Task Force now recommends routine anxiety screening for all adults under 65 as part of standard primary care visits.
Related Articles
- Anxiety and Burnout: Understanding the Biological Damage - A clinical look at how chronic anxiety and burnout compound to damage your body's stress response systems.
- Workplace Mental Health Workbooks Guide - Practical workbook-based approaches for managing anxiety and mental health challenges in professional settings.
- Dealing With Depression: 5 Simple Steps - Because anxiety and depression share genetic roots and frequently occur together, these evidence-based depression strategies complement anxiety treatment.
- Yoga for a Healthy Mind - Research on how yoga practice reduces anxiety symptoms through parasympathetic nervous system activation and mindfulness.
- Depression: Complementary Health Approaches - Evidence-based alternative and complementary therapies that address the anxiety-depression overlap.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











