
TL;DR: Perimenopause typically starts in your mid-40s and can drag on for 4 to 10 years. Up to 80% of women get hit with hot flashes, plus sleep problems, mood changes, and irregular periods. Exercise, Mediterranean-style eating, mind-body practices, and targeted nutrient support can all help, but they work best alongside medical guidance when symptoms are severe.
What Happens During Perimenopause
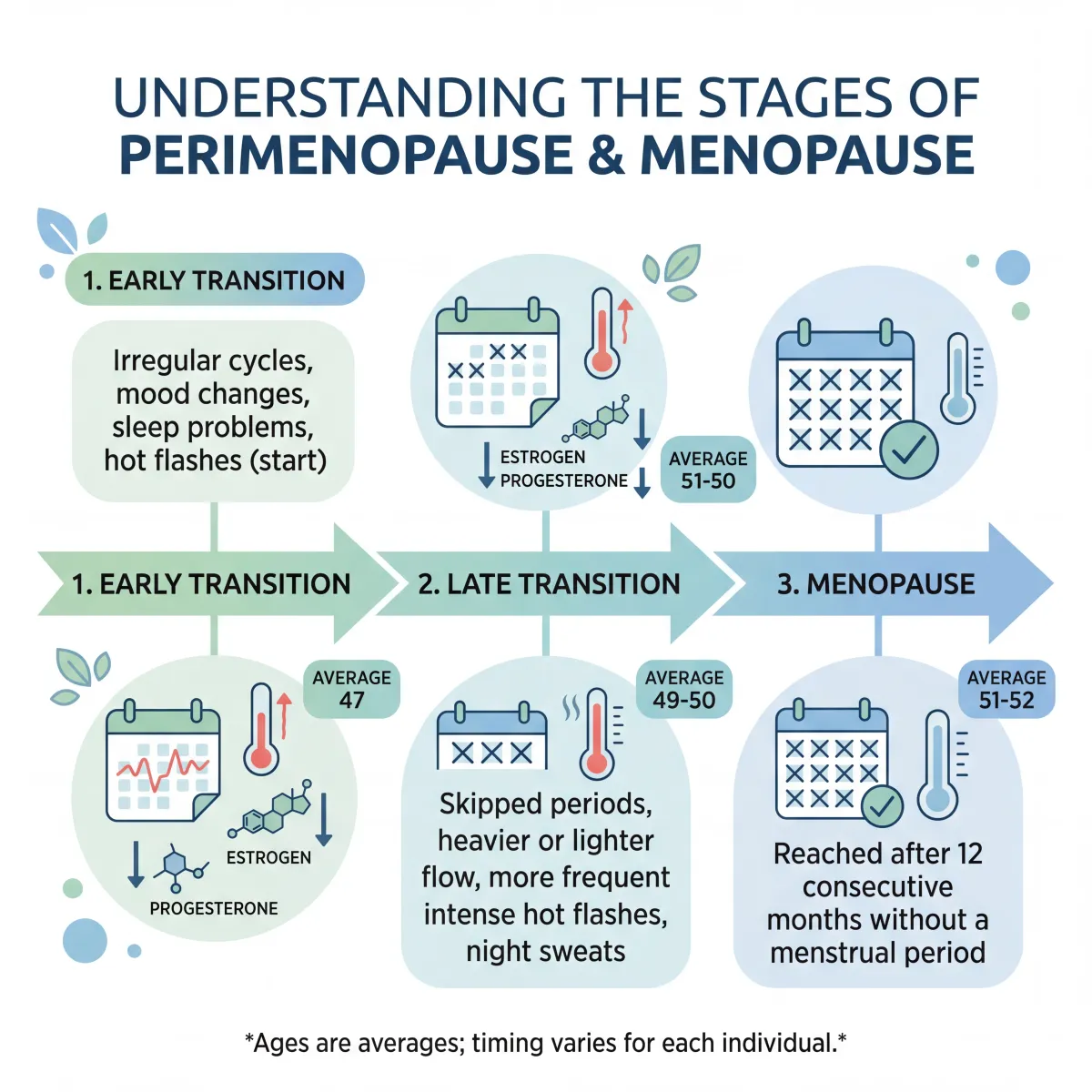
Perimenopause isn't a switch that flips. It's a slow transition that plays out over years as your ovaries gradually wind down hormone production. The Study of Women's Health Across the Nation (SWAN), one of the largest longitudinal studies on the topic, found the median onset is around age 47. The final menstrual period usually arrives between 51 and 52.
The transition breaks into two stages. In the early stage, your menstrual cycles start to vary by seven or more days. In the late stage, you skip periods entirely, with gaps of 60 days or longer. Once you go a full 12 months without a period, you've reached menopause.
Here's the part most people get wrong: it's not simply about "running out of estrogen." The earliest detectable shift is a decline in inhibin B, a peptide produced by ovarian follicles that normally keeps follicle-stimulating hormone (FSH) in check. As inhibin B drops, FSH rises. Estrogen levels stay relatively normal at first. The steep estrogen drops most women associate with menopause come later, during the late transition, when you start having more anovulatory cycles.
How long this takes depends on your body, your background, and your habits. SWAN found that African American women had the longest vasomotor symptom duration (median 10.1 years), compared to 6.5 years for non-Hispanic white women and 4.8 years for Japanese women. Women who started their transition younger tended to have a longer, rougher ride overall.
Common Symptoms That Signal the Transition
Perimenopause can sneak up on you. Some women notice nothing beyond irregular periods. Others get hit with multiple overlapping symptoms that mess with work, sleep, and relationships. According to Cleveland Clinic, the experience varies widely from person to person.
Hot flashes and night sweats
Up to 80% of women experience hot flashes during perimenopause. They come on fast, usually as a sudden wave of heat across your face, neck, and chest, often followed by chills and sweating. The SWAN cohort tracked prevalence rising from 39% in early perimenopause to 67% overall. And here's the number that surprises most people: hot flashes don't just last a year or two. Recent SWAN data shows median durations of 7 to 10 years. Women who start having symptoms before or during perimenopause face the longest stretch, with a median of 11.8 years.
Sleep problems
SWAN found that 37% of women between 40 and 55 reported difficulty sleeping. Night sweats play a part, but they don't explain everything. Hormonal fluctuations independently mess with sleep architecture in ways researchers are still working to fully understand. One clear finding: if you slept poorly before perimenopause, you'll likely sleep worse during it.
Mood changes and mental health
This one deserves more attention than it typically gets. Three major longitudinal studies (SWAN, Penn Ovarian Aging Study, Harvard Study of Moods and Cycles) all found that women were 2 to 4 times more likely to experience a major depressive episode during perimenopause. That held true even after researchers controlled for prior depression history, medications, and stressful life events. The risk of adverse mood symptoms jumped from 20% before perimenopause to 62% by early transition. These aren't "just in your head." They're driven by biological changes.
Vaginal and urinary changes
Declining estrogen thins vaginal tissue, reduces elasticity, and raises vaginal pH. Between a third and half of women develop what clinicians now call genitourinary syndrome of menopause. SWAN noted a decline in sexual functioning starting about 20 months before the final menstrual period, with the steepest drop during the late transition. Unlike hot flashes, these symptoms don't tend to get better on their own.
| Symptom | Prevalence | Typical Duration |
|---|---|---|
| Hot flashes | Up to 80% | 7-10 years (median) |
| Sleep disruption | 37% of women 40-55 | Stabilizes post-menopause |
| Mood changes/depression | 2-4x increased risk | Peaks in early transition |
| Irregular periods | 82% experience changes | Throughout transition |
| Vaginal dryness | 33-50% | Progressive without treatment |
| Bone density loss | Accelerated in all women | Most rapid first 5 years post-menopause |
Evidence-Based Natural Management Approaches
Before reaching for any supplement or remedy, you should know what the research actually supports and where it falls short. The 2023 position statement from The North American Menopause Society (NAMS) reviewed nonhormone treatments for vasomotor symptoms and sorted them by evidence quality. The results might surprise you.
For hot flashes specifically, NAMS recommended cognitive-behavioral therapy and clinical hypnosis based on Level I evidence (good, consistent scientific data). Weight loss got a recommendation with Level II-III evidence. But exercise, yoga, and dietary supplements? Not recommended for hot flashes. The evidence was too inconsistent.
That distinction matters a lot. Exercise and yoga may not cool down your hot flashes, but they have solid evidence for just about everything else perimenopause throws at you: sleep, mood, bone density, cardiovascular health, body composition. So the smarter approach is using each tool where the evidence actually supports it.

Structured exercise
Exercise is probably the single most broadly useful thing you can do during perimenopause. It won't eliminate hot flashes, but it directly helps with sleep, mood, bone preservation, and metabolic health. A randomized study on exercise and dietary interventions for perimenopausal women found improvements in metabolic markers, body composition, and overall quality of life.
The Mayo Clinic recommends weight-bearing exercises like walking, hiking, and strength training. Resistance training is worth special attention here because it directly counteracts the accelerated bone and muscle loss that starts during this transition. As estrogen drops, bone density declines faster, and lifting heavy things is one of the best ways to fight back.
| Exercise Type | Primary Benefits | Recommended Frequency |
|---|---|---|
| Resistance training | Bone density, muscle mass, metabolic rate | 2-3 sessions per week |
| Aerobic exercise | Cardiovascular health, mood, sleep | 150 minutes moderate/week |
| Mind-body exercise | Anxiety, depression, sleep, bone density | 2-3 sessions per week |
| Flexibility/stretching | Joint mobility, injury prevention | Daily or most days |
Cognitive-behavioral therapy
CBT is one of the few nonhormone interventions that NAMS backs with Level I evidence specifically for vasomotor symptoms. CBT for hot flashes works by reframing how you think about and respond to symptoms, and by breaking behavioral patterns (like avoiding sleep or social situations) that make the cycle worse. It doesn't actually reduce the number of hot flashes. What it does is significantly change how bothersome they feel and how much they interfere with your life. For some women, that shift makes all the difference.
Weight management
Body weight and perimenopause symptoms have a complicated relationship. Women with higher BMI tend to report worse hot flashes during the transition, though those same symptoms may ease up after menopause. NAMS recognized weight loss as helpful for vasomotor symptoms based on Level II-III evidence. Beyond symptom relief, keeping weight in a healthy range during perimenopause lowers your cardiovascular risk, which climbs as estrogen declines. SWAN found that higher BMI was linked to a slower hormonal decline but a worse overall symptom burden. Slower doesn't mean easier.
Nutrition and Dietary Strategies That Support Hormonal Health
A 2025 review in Frontiers in Nutrition pulled together 42 high-quality studies on dietary interventions for menopausal women. The takeaway: what you eat has a measurable effect on both symptoms and long-term disease risk.
The Mediterranean diet has the strongest track record
Of all the dietary patterns studied for menopause, the Mediterranean diet comes out on top. Meta-analyses show higher adherence is linked to less severe vasomotor symptoms, better lipid profiles, lower blood pressure, and better bone mineral density. The likely mechanism: the diet is loaded with polyphenols and omega-3 fatty acids, both of which tamp down the inflammatory pathways that ramp up during perimenopause.
In practice, that means lots of vegetables, fruits, legumes, whole grains, olive oil, nuts, and moderate fish. This pattern also tends to be high in fiber, which research links to lower vasomotor symptom severity. If you're looking for a starting point, Mediterranean-style eating is a solid one.

Nutrients that matter more right now
A 2023 review in Nutrients identified several micronutrients that become more important during perimenopause. The general rule: get them from food first, and only supplement when there's a documented deficiency.
| Nutrient | Daily Target | Best Food Sources | Why It Matters |
|---|---|---|---|
| Calcium | 1,200 mg | Dairy, leafy greens, fortified plant milks | Counteracts accelerated bone loss |
| Vitamin D | 800-2,000 IU | Fatty fish, eggs, fortified foods, sunlight | Helps calcium absorption, supports bone density |
| Protein | 1.1-1.5 g/kg body weight | Lean meats, legumes, nuts, dairy | Preserves muscle mass, supports metabolic rate |
| Magnesium | 320 mg | Nuts, seeds, whole grains | Reduces inflammation, improves sleep quality |
| Omega-3 fatty acids | 1-2 g EPA+DHA | Fatty fish, walnuts, flaxseed | Lowers triglycerides, reduces inflammation |
Magnesium is worth calling out because deficiency is so common and the symptoms overlap with perimenopause itself: muscle cramps, poor sleep, mood swings. Magnesium glycinate tends to be the go-to for sleep and anxiety because of its calming effect and good absorption.
Protein needs also go up. As your metabolic rate slows and muscle mass drops, you need more protein just to maintain what you have. The Frontiers review recommends 1.1 to 1.5 grams per kilogram of body weight daily. The key is spreading it across your meals rather than loading it all into dinner.
What to cut back on
Cleveland Clinic flags sugary foods, saturated fat, excess alcohol, and caffeine as symptom amplifiers. Alcohol affects thermoregulation and can trigger hot flashes. Caffeine disrupts sleep that's already fragile. And saturated fat feeds the low-grade inflammation that kicks up during perimenopause.
Mind-Body Practices That Deliver Measurable Relief
A 2024 meta-analysis published in Menopause looked at 11 randomized controlled trials involving 1,005 women and found that mind-body exercises produce real, measurable improvements across multiple perimenopause symptoms.
The researchers pooled data from studies on tai chi, yoga, Pilates, qigong, baduanjin, and mindfulness-based stress reduction. Compared to control groups, they found statistically significant improvements in five areas:
- Bone mineral density improved (SMD 0.41, P = 0.001)
- Sleep quality improved (SMD -0.48, P = 0.002)
- Anxiety reduced (SMD -0.80, P = 0.0002)
- Depression reduced (SMD -0.80, P < 0.0001)
- Fatigue reduced (SMD -0.67, P < 0.0001)
To put those numbers in context: an SMD of 0.80 is considered a large effect size. That's comparable to what some pharmaceutical interventions achieve for anxiety and depression. The bone density improvements are more modest but still notable, especially given that these practices carry essentially no risk.
If you already do yoga or have been thinking about starting, perimenopause is a good time to make it a regular habit. The combination of movement, breathwork, and mindfulness hits several symptom clusters at once.
Clinical hypnosis
This one catches people off guard: clinical hypnosis earned a Level I recommendation from NAMS for hot flashes. In controlled trials, it cut hot flash frequency by about 74% compared to structured attention control. To be clear, this isn't stage hypnosis. It's a therapeutic technique involving guided relaxation and focused attention, usually delivered by a trained therapist over about 5 sessions.
Stress management
Perimenopause turns up the volume on your stress response. The hormonal fluctuations interact with the hypothalamic-pituitary-adrenal axis in ways that make everyday stressors feel harder to handle. Chronic stress, in turn, worsens hot flashes, sleep problems, and mood symptoms. It becomes a feedback loop. Techniques like meditation, progressive muscle relaxation, and deep breathing won't eliminate hot flashes, but they help break that cycle.
Myths vs Facts About Perimenopause
| Myth | Fact |
|---|---|
| Perimenopause starts at 50 | The median onset is age 47, and some women notice changes in their mid-30s |
| Hot flashes last 1-2 years | Median duration is 7-10 years. Women who start early can deal with them for 11+ years |
| You can't get pregnant during perimenopause | If you're still getting periods, even irregular ones, ovulation can still happen |
| A blood test can confirm perimenopause | Hormones fluctuate too much for a single test to be reliable. Diagnosis is based on symptoms and menstrual history |
| Herbal supplements reliably stop hot flashes | The 2023 NAMS review did not recommend supplements or herbal remedies for vasomotor symptoms. Evidence shows limited effectiveness |
| Mood changes are "all in your head" | Three large longitudinal studies confirmed a 2-4x increased risk of major depressive episodes during perimenopause, driven by biological hormonal shifts |
| Androgens plummet during perimenopause | Multiple cohort studies show testosterone stays relatively stable or even rises due to declining SHBG, with up to 80% increases in free androgen index |
When to Talk to Your Doctor
Lifestyle strategies help, but some situations need medical attention, not just self-management:
- Severe hot flashes that disrupt your work, relationships, or sleep even after lifestyle changes. Hormone therapy is still the most effective treatment for vasomotor symptoms, and it's worth talking to your provider about.
- Heavy or prolonged bleeding if you're changing pads or tampons every 1-2 hours, bleeding for more than 7 days, or spotting between periods. According to a clinical review in Open Life Sciences, 19% of women with shortened menstrual cycles had histological findings that included precancerous changes. Get it checked.
- New or worsening depression or anxiety that gets in the way of daily life. The increased risk of major depressive episodes during perimenopause is biologically real, and treatment with low-dose antidepressants or hormone therapy can help a lot.
- Vaginal symptoms causing real discomfort. Unlike hot flashes, these tend to get worse over time without treatment. Topical vaginal estrogen works well and carries very little systemic risk.
- Bone density concerns, especially if you're petite, have a smoking history, family history of osteoporosis, or have used steroids long-term.
- Cardiovascular risk factors. SWAN linked frequent vasomotor symptoms to higher cardiovascular disease risk over 14 years. Perimenopause is a good time to get your blood pressure, cholesterol, and metabolic markers checked.
Your doctor can help sort out what's normal perimenopause and what might be something else. Thyroid disorders are a common mimic and should be ruled out. The best outcomes come from combining lifestyle strategies with medical support where it's needed.

Frequently Asked Questions
What is the difference between perimenopause and menopause?
Perimenopause is the transition period when your ovaries are winding down estrogen production and your cycles become irregular. Menopause is the point when you've gone 12 straight months without a period. Most women reach menopause between 51 and 52, while perimenopause usually starts around 47 and lasts a median of 4 years, though some women spend much longer in it.
Can exercise stop hot flashes during perimenopause?
Not reliably. The 2023 NAMS position statement classified exercise as "not recommended" specifically for vasomotor symptom treatment based on Level II evidence. But exercise helps with nearly everything else perimenopause throws at you: mood, sleep, bone density, cardiovascular health, and body composition. It's still one of the most worthwhile things you can do during this time.
Which supplements actually help with perimenopause symptoms?
Evidence supports calcium (1,200 mg/day) and vitamin D (800-2,000 IU/day) for bone health, omega-3 fatty acids for cardiovascular protection and lowering inflammation, and magnesium for sleep and muscle cramps. But the 2023 NAMS review didn't find enough evidence to recommend herbal supplements, soy isoflavones, or black cohosh for hot flashes. Generally, getting nutrients from food is better than relying on pills.
How do I know if what I'm experiencing is perimenopause or something else?
Doctors diagnose perimenopause based on age, symptoms, and menstrual history, not blood tests. If you're in your 40s and your periods are becoming irregular, especially alongside hot flashes, sleep changes, or mood shifts, perimenopause is the likely explanation. But thyroid problems, depression, and sleep apnea can look similar, so it's worth seeing a provider if your symptoms are severe or don't fit the typical pattern.
Does perimenopause affect heart health?
Yes. Declining estrogen leads to unfavorable cholesterol changes: LDL goes up, HDL goes down. SWAN found that women with frequent hot flashes had higher cardiovascular disease risk over 14 years of follow-up, particularly when symptoms started later in the transition. That makes perimenopause an important window for getting your cardiovascular risk factors checked and managed.
Related Articles
- Magnesium Types Explained: Glycinate, Citrate, and Threonate — A breakdown of different magnesium forms and which ones work best for sleep, anxiety, and muscle recovery.
- Omega-3 Benefits, Sources, and Supplements — How EPA and DHA support heart health, reduce inflammation, and protect brain function during hormonal transitions.
- Anti-Inflammatory Eating Patterns: Mediterranean vs DASH vs Plant-Based — Compare evidence-based dietary approaches that reduce chronic inflammation and support overall health.
- Vitamin D Benefits, Deficiency Warnings, and Precautions — Why vitamin D matters for bone health and immune function, with guidance on testing and safe supplementation.
- Chronic Stress, Hormones, and HPA Axis Recovery — How chronic stress disrupts hormonal balance and evidence-based strategies for recovery.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











