
Your heartbeat tells a bigger story than you think
Most people assume a steady, metronomic heartbeat is the hallmark of cardiovascular health. The opposite is true. A healthy heart speeds up and slows down constantly, adjusting its rhythm in response to breathing, posture changes, emotions, and dozens of other signals your body processes every second. The time gaps between consecutive heartbeats — measured in milliseconds — fluctuate in complex, nonlinear patterns. That fluctuation is heart rate variability, or HRV.
HRV has moved from an obscure cardiology metric to mainstream health tracking in the last decade, partly because wearables like the Apple Watch, WHOOP band, and Oura ring now estimate it overnight. But the science behind it goes back further than any smartwatch. Researchers first noticed in 1965 that fetal distress shows up as reduced HRV before heart rate itself changes. By the 1970s, cardiologists were using HRV to predict autonomic neuropathy in diabetic patients before symptoms appeared. And a landmark finding showed that reduced HRV after a heart attack was a stronger predictor of death than most other known risk factors.
HRV reflects the real-time interplay between your sympathetic and parasympathetic nervous systems. When those systems can rapidly shift gears, accelerating your heart for a sprint and then calming it for sleep, HRV tends to be high. When that flexibility erodes through chronic stress, poor sleep, or disease, HRV drops. It is a readout of your body's capacity to adapt.
Two branches, one nervous system
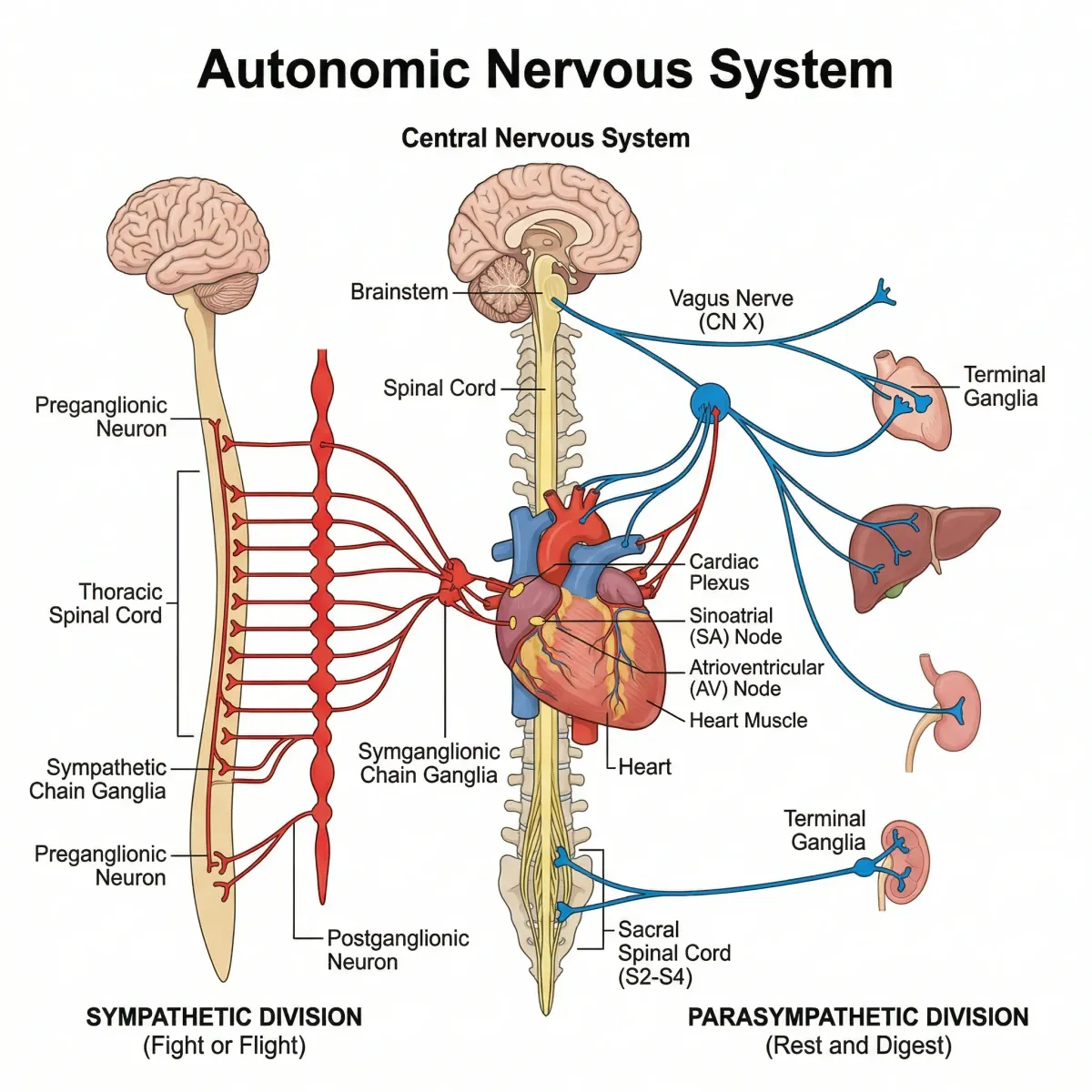
The autonomic nervous system (ANS) runs in the background of every moment of your life, regulating heart rate, blood pressure, digestion, and breathing without conscious effort. It splits into two branches: the sympathetic nervous system (SNS), which accelerates your heart when you face a challenge, and the parasympathetic nervous system (PNS), which slows it down during rest and recovery.
The common "teeter-totter" analogy oversimplifies the relationship. These two branches do not operate as a simple zero-sum game. After a hard workout, for example, parasympathetic reactivation begins while sympathetic activity is still elevated — both branches active simultaneously. Slow breathing during high-stress moments can also engage both systems at once, increasing respiratory sinus arrhythmia (the natural speeding and slowing of heart rate with each breath cycle) even while sympathetic drive remains high. Shaffer and Ginsberg described this as analogous to a Formula 1 driver accelerating through a turn while feathering the brake — a technique called left-foot braking.
The speed difference between these two branches matters for HRV. Parasympathetic signals through the vagus nerve reach the heart in under one second. Sympathetic signals take five seconds or longer to produce a steady effect. Because the vagus nerve acts so fast, any beat-to-beat change in heart rate — the kind of rapid fluctuation that HRV captures — is overwhelmingly parasympathetic in origin. This is why HRV is often called an index of vagal tone, even though the full picture is more complicated.
Quick fact: An average resting heart rate of 73 bpm in healthy adults reflects parasympathetic dominance. Without any autonomic input (as in a denervated transplanted heart), the heart's intrinsic pacemaker fires at roughly 100 bpm.
What your HRV numbers actually mean
Open any HRV app and you will see numbers like RMSSD, SDNN, or a simplified "HRV score." These are not interchangeable metrics, and understanding their differences prevents misinterpretation.
| Metric | What it measures | Best recording window | What it reflects |
|---|---|---|---|
| RMSSD | Beat-to-beat variability (root mean square of successive differences) | 1-5 minutes | Parasympathetic (vagal) activity |
| SDNN | Overall variability (standard deviation of all normal intervals) | 5 min or 24 hours | Both sympathetic and parasympathetic input; total regulatory capacity |
| HF power (0.15-0.4 Hz) | High-frequency oscillations linked to breathing | 5 minutes | Vagal modulation of heart rate |
| LF power (0.04-0.15 Hz) | Lower-frequency oscillations | 2-5 minutes | Baroreflex activity (not purely sympathetic, despite old claims) |
| LF/HF ratio | Ratio of low to high frequency power | 5 minutes | Controversial — not a reliable marker of "sympathovagal balance" |
Most consumer wearables report RMSSD because it reliably tracks vagal activity from short overnight recordings. The metric can be validly estimated from as little as 60 seconds of clean data, according to research that validated ultra-short-term HRV measurements against the standard 5-minute benchmark.
SDNN is the clinical gold standard when measured over 24 hours. In a study of cardiac patients, those with 24-hour SDNN values above 100 milliseconds had a 5.3 times lower risk of mortality compared to those below 50 ms. The clinical breakdown works like this:
| 24-hour SDNN range | Classification | Clinical meaning |
|---|---|---|
| Above 100 ms | Healthy | Strong autonomic regulatory capacity |
| 50-100 ms | Compromised | Reduced adaptability; higher risk |
| Below 50 ms | Unhealthy | Severely depressed HRV; elevated mortality risk |
These numbers come from 24-hour ambulatory recordings, not 5-minute snapshots. Short-term and 24-hour values correlate poorly and have different physiological meanings, so comparing a morning RMSSD reading from your smartwatch to clinical 24-hour SDNN cutoffs is not valid.
Age and sex shape your baseline
HRV declines with age. A study tracking 166 healthy volunteers found the sharpest drop between the 20s and 30s, followed by a gradual decline. A meta-analysis of over 296,000 healthy participants revealed that women have higher resting heart rates but greater high-frequency power (an indicator of vagal dominance) compared to men, while men show higher low-frequency power and overall sympathetic predominance. In practical terms, comparing your HRV to a generic population average without accounting for age and sex misses the mark.

How to track HRV without a lab coat
Clinical HRV measurement uses electrocardiography (ECG) with electrodes on the chest. That remains the gold standard. But consumer-grade photoplethysmography (PPG) — the green LED sensor on the back of your smartwatch — has closed the gap substantially. One validation study found that ECG and PPG methods produced discrepancies of less than 6% for most HRV measures, though pNN50 (the percentage of successive intervals differing by more than 50 ms) showed a wider 29.9% gap.
What matters more than the sensor type is when and how you measure. HRV fluctuates throughout the day in response to food, caffeine, stress, and physical activity. The most reliable tracking window is during sleep or first thing in the morning, in the same position (ideally lying down), for at least 60 seconds. Trends over weeks and months reveal far more than any single reading.
| Device type | Sensor | HRV metrics | Best for |
|---|---|---|---|
| Chest strap (Polar H10, Garmin HRM-Pro) | ECG | RMSSD, SDNN, frequency-domain | Most accurate; real-time biofeedback |
| Smartwatch (Apple Watch, Garmin) | PPG | RMSSD (overnight average) | Passive daily tracking; long-term trends |
| Ring (Oura) | PPG | RMSSD, HRV balance | Sleep-focused tracking; comfort |
| Band (WHOOP) | PPG | RMSSD (rolling average) | Recovery scoring; strain tracking |
| HRV apps (Elite HRV, HRV4Training) | Camera/chest strap | RMSSD, lnRMSSD, weekly trends | Structured morning readings; guided protocol |
A few practical points: chest straps paired with dedicated HRV apps still beat wrist-based sensors for accuracy during active measurements. Wrist PPG sensors struggle when you move, which is why most wearables only calculate HRV during sleep. If you want clean data for biofeedback training, a chest strap is the way to go.
Evidence-based ways to raise your HRV
HRV responds to intervention. Several approaches have measurable effects on autonomic regulation, and the research behind them is more specific than most wellness content suggests.
Slow breathing and HRV biofeedback
Breathing at approximately 6 breaths per minute — roughly a 5-second inhale and 5-second exhale — produces a distinctive spike in LF power centered around 0.1 Hz. This corresponds to the cardiovascular system's resonance frequency, a rate at which the baroreflex loop between your heart and brain amplifies heart rate oscillations. HRV biofeedback training uses real-time feedback (typically from a chest strap connected to a screen) to help people find and sustain their personal resonance frequency. The resonance frequency varies slightly between individuals, typically falling between 4.5 and 7.5 breaths per minute.
Breathing at resonance frequency simultaneously engages both sympathetic and parasympathetic branches, producing large swings in heart rate within each breath cycle. It is not a relaxation technique in the conventional sense. Over weeks of regular practice, studies on HRV biofeedback show improvements in SDNN and RMSSD that persist even when not actively doing the breathing exercise.
Mind-body exercise: yoga and tai chi
A meta-analysis of 17 randomized controlled trials found that tai chi and yoga produce measurable improvements in HRV parameters. The analysis showed a moderate effect on the LF/HF ratio (Hedge's g = -0.58, indicating a shift toward parasympathetic dominance) and a large effect on perceived stress (Hedge's g = -0.80). Yoga had stronger evidence than tai chi in this particular analysis. The minimum effective dose appeared to be 60 minutes per week, though larger LF/HF ratio improvements correlated with greater weekly training volume.
Both practices share elements that likely drive the effect: controlled diaphragmatic breathing, sustained postures that challenge balance, and deliberate mental focus. The breathing component may be the primary mechanism, given how strongly respiratory patterns influence HRV.
Aerobic exercise
Regular aerobic training is one of the most robust HRV boosters in the literature. It works partly by lowering resting heart rate — a slower heart rate provides more time between beats for variability to occur (a phenomenon called cycle length dependence). Trained athletes typically show SDNN and RMSSD values well above age-matched sedentary peers. In a study of 145 elite track-and-field athletes, both male and female athletes showed substantially elevated HRV time-domain measures compared to the general population norms reported in a meta-analysis of over 21,000 healthy adults.
You do not need to be an elite athlete. Moderate aerobic exercise — 150 minutes per week of brisk walking, cycling, or swimming — improves HRV in previously sedentary adults. The key is consistency over months, not intensity of individual sessions.

Sleep quality
HRV reaches its highest values during deep sleep, particularly in the early part of the night. Disrupted sleep timing and poor sleep architecture reliably depress overnight HRV. The relationship runs both directions: poor sleep lowers HRV, and low HRV predicts poor sleep quality. Practical steps include maintaining a consistent sleep schedule, keeping the room cool and dark, and limiting alcohol — even moderate drinking reduces overnight HRV by suppressing parasympathetic activity during the first half of sleep.
Nutrition and supplements
Omega-3 fatty acids from fish oil have shown modest HRV improvements in clinical trials, likely through anti-inflammatory and membrane-stabilizing effects on cardiac cells. Magnesium plays a role in cardiac electrical stability, and deficiency has been linked to reduced HRV. A diet rich in polyphenol-containing foods — berries, dark chocolate, green tea — may also support HRV through antioxidant and anti-inflammatory pathways, though the direct evidence is still emerging.
Cold exposure and sauna
Cold water immersion acutely increases sympathetic activation, but repeated cold exposure over weeks has been associated with improved parasympathetic tone at rest. Sauna use has also shown promise for HRV improvement. Evidence from clinical trials suggests that Waon therapy (a form of infrared sauna used with chronic heart failure patients) improved autonomic nervous system activity. Both practices likely work by training the autonomic system to shift rapidly between states — the same adaptive capacity that HRV measures.
What consistently lowers HRV
Chronic psychological stress, inadequate sleep, excessive alcohol, overtraining without adequate recovery, and sedentary behavior all reduce HRV. Inflammation — whether from chronic illness, poor diet, or persistent infections — independently depresses HRV. Low VLF power (the very-low-frequency band) has been associated with all-cause mortality more strongly than either LF or HF power, and is linked to both high inflammation and low testosterone levels.
HRV myths versus reality
| Myth | Reality |
|---|---|
| Higher HRV is always better | Not always. Cardiac conduction abnormalities like atrial fibrillation can artificially inflate HRV readings. Pathologically elevated HRV, particularly in the elderly, is linked to increased mortality risk. |
| The LF/HF ratio measures sympathetic vs. parasympathetic balance | This interpretation has been widely challenged. At rest, LF power primarily reflects baroreflex activity, not sympathetic drive. Breathing rate alone can shift LF power dramatically without any change in actual sympathetic nervous system activity. |
| A single morning HRV reading tells you whether to train hard today | One data point is noise. HRV naturally fluctuates day to day. Trends over 7-14 days are far more informative than any isolated number. |
| You can compare HRV scores across different apps and devices | Different algorithms, sensor types, and measurement windows make cross-device comparisons unreliable. Pick one device and track your own trend. |
| HRV and heart rate are the same thing | They measure different phenomena. Two people with identical resting heart rates of 60 bpm can have vastly different HRV values, reflecting different levels of autonomic flexibility. |
Frequently Asked Questions
What is a good HRV for my age?
There is no single universal "good" number because HRV varies widely among healthy individuals. The most useful approach is to track your own trend over time rather than benchmarking against population averages. That said, RMSSD values in healthy adults under 40 typically range from 25 to 45 ms in short-term recordings, declining with each decade. A meta-analysis of over 21,000 healthy adults found average short-term SDNN values between 50 and 80 ms with very wide individual variation.
Can I improve my HRV in just a few weeks?
Some interventions produce measurable changes relatively quickly. HRV biofeedback (slow breathing at resonance frequency) can shift LF power within a single session and produce sustained RMSSD improvements within 4-6 weeks of regular practice. Yoga practiced at 60 minutes per week has shown significant autonomic changes in studies lasting 8-16 weeks. Aerobic fitness improvements tend to require a longer timeline of 8-12 weeks of consistent training.
Should I check my HRV every day?
Daily tracking is useful for building a personal baseline and spotting trends, but do not react to individual readings. Normal day-to-day fluctuation is expected. If your average HRV over a 7-day rolling window drops noticeably (more than one standard deviation below your personal mean) and stays low, that signals something worth investigating — illness, accumulated stress, overtraining, or insufficient recovery.
Does fasting affect HRV?
Short-term fasting (16-24 hours) tends to increase parasympathetic activity in some studies, potentially raising HRV. The relationship depends on individual stress response to the fast. If fasting causes significant psychological stress or cortisol elevation, any parasympathetic benefit may be offset. For people already under high stress, aggressive fasting protocols can lower rather than raise HRV.
Is a chest strap really more accurate than a wrist sensor for HRV?
For resting and sleep measurements, wrist-based PPG sensors are adequate for tracking RMSSD trends over time. During movement or active biofeedback sessions, chest-strap ECG sensors are considerably more accurate. One comparison found less than 6% discrepancy between ECG and PPG for most HRV measures at rest, but accuracy degrades with motion. If you are doing structured HRV biofeedback training, a chest strap paired with a dedicated app provides the cleanest data.
Related Articles
- Vagus nerve and heart health — The vagus nerve is the primary parasympathetic pathway that drives HRV; learn how it connects your brain and cardiovascular system.
- Sleep timing, heart health, and circadian rhythm — Sleep architecture directly shapes overnight HRV, making consistent sleep one of the strongest interventions for autonomic health.
- Best magnesium for heart health — Magnesium supports cardiac electrical stability and has been linked to improved HRV in supplementation studies.
- Polyphenol-rich foods for heart health — Anti-inflammatory and antioxidant compounds in polyphenol-rich diets may support autonomic function over time.
- Autophagy, fasting, exercise, and diet — Fasting and exercise both influence HRV, though their effects depend on individual stress tolerance and recovery capacity.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











