
The Hidden Cost of Eating Less on GLP-1 Medications
Semaglutide, tirzepatide, and other GLP-1 receptor agonists do exactly what they promise. They reduce appetite, slow gastric emptying, and help people eat significantly less food. That last part, though, carries a nutritional consequence that gets far less attention than the weight loss headlines.
When you reduce your calorie intake by 16 to 39 percent, as most people on these medications do, you are not just eating fewer calories. You are eating fewer vitamins, minerals, and essential nutrients. Your body still needs the same amounts of iron, vitamin D, magnesium, and B vitamins it always did. But the vehicle for delivering them, food, has gotten much smaller.
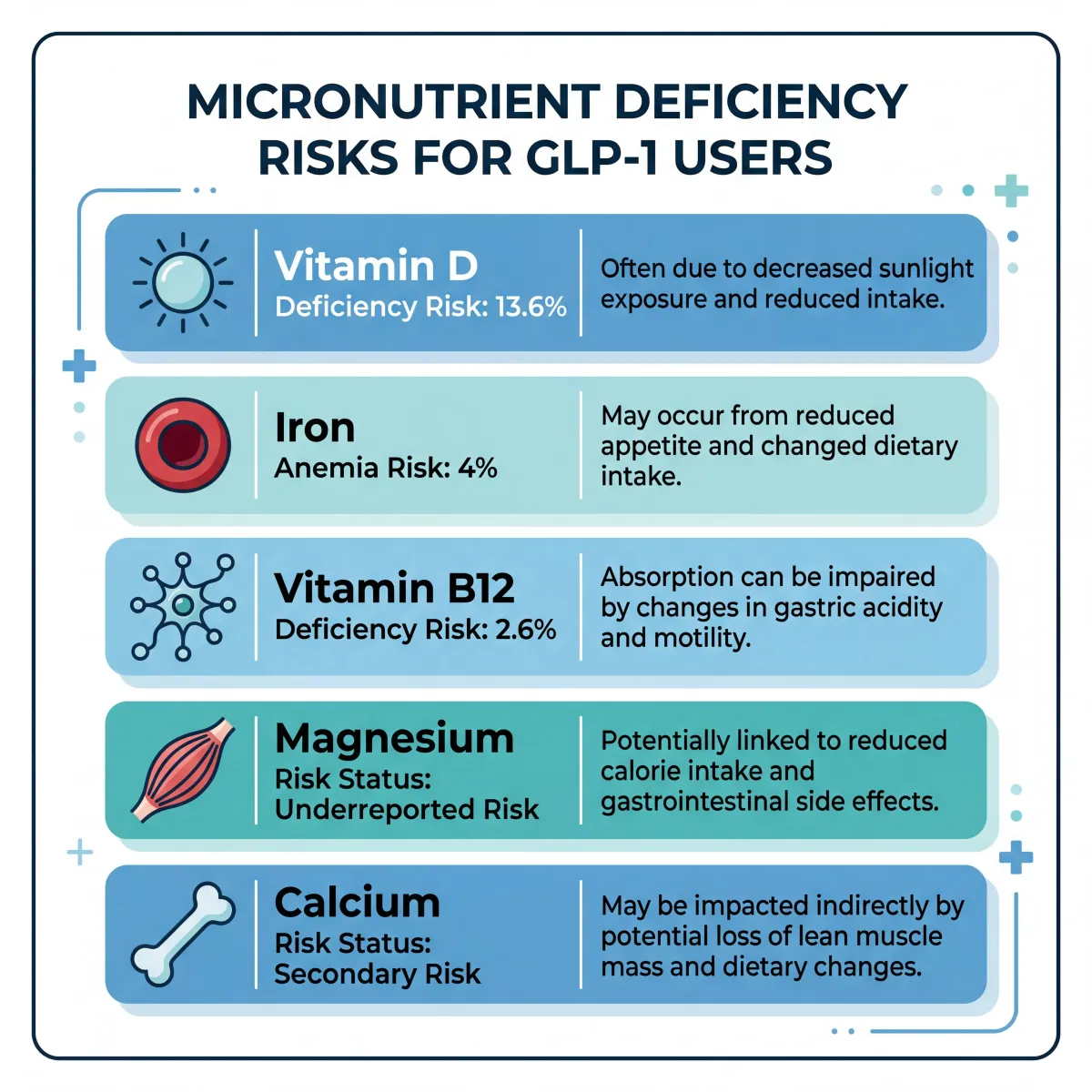
A retrospective study of over 461,000 adults prescribed GLP-1 receptor agonists found that 22.4 percent developed a diagnosed nutritional deficiency within their first year on treatment. That is nearly one in four people. Vitamin D deficiency led the pack at 13.6 percent, followed by nutritional anemia at 4 percent and B vitamin deficiencies at 2.6 percent.
Key takeaway: GLP-1 medications reduce how much you eat, but your micronutrient requirements remain the same. The gap between what your body needs and what it receives through a reduced diet is where targeted supplementation becomes valuable.
The gastrointestinal side effects compound the problem. Nausea affects 25 to 44 percent of users, diarrhea hits 19 to 30 percent, and vomiting occurs in 8 to 24 percent. These symptoms do not just make eating unpleasant. They can actively impair nutrient absorption and reduce the variety of foods people are willing to eat. Someone battling persistent nausea is not going to force down a plate of iron-rich spinach and salmon.
A joint advisory from four major medical societies, including the American Society for Nutrition and the Obesity Medicine Association, put it plainly: people on GLP-1 therapy need proactive nutritional monitoring and, in many cases, targeted supplementation to fill the gaps that a reduced diet creates.
Which Micronutrients Are Most at Risk?
Not every nutrient is equally vulnerable during GLP-1 therapy. Some face a double hit: reduced intake from eating less plus impaired absorption from the medication's effects on your digestive system. Understanding which nutrients are most affected helps you prioritize what to supplement rather than blindly taking everything on the shelf.
Vitamin D
Vitamin D deficiency is the single most common nutritional shortfall in people taking GLP-1 medications, and it was already widespread before these drugs entered the picture. People with obesity are roughly 35 percent more likely to be deficient compared to those at normal weight because vitamin D gets sequestered in fat tissue and becomes less bioavailable. When you add reduced dietary intake on top of that baseline disadvantage, the numbers get concerning fast. A narrative review of supplement considerations during GLP-1 therapy recommended therapeutic dosing of approximately 7,100 IU daily or 50,000 IU weekly, well above the standard recommended daily allowance. At these levels, vitamin D also supports muscle quality and reduces low-grade inflammation, both relevant when you are losing weight rapidly.
Iron
Iron faces a uniquely difficult situation with GLP-1 medications. It is not just that people eat less iron-rich food. A pilot study from the University Hospital Dubrava tested iron absorption directly in 51 patients before and after starting semaglutide. The results were striking: the median increase in serum iron after an oral absorption test dropped from 19 percent before treatment to just 8 percent after ten weeks on the medication. Nearly one in five participants showed a clinically significant impairment of 30 percent or more in their iron absorption capacity. The mechanism likely involves semaglutide's effect on gastric emptying and intestinal transit, which changes how long iron sits in the optimal absorption zone of the upper small intestine.
B Vitamins
Vitamin B12 levels showed a meaningful decline in patients tracked over 12 months on semaglutide, dropping from a mean of 567 to 494 micrograms per deciliter. Thiamine (B1) is another concern flagged by the joint advisory, particularly in patients who experience frequent vomiting, as the body has limited storage capacity for water-soluble B vitamins and depletes them faster during GI distress.
Magnesium, Calcium, and Electrolytes
The electrolyte story is perhaps the most underappreciated risk. A published case report detailed a 73-year-old woman on semaglutide whose magnesium dropped to undetectable levels, sending her to the hospital after collapsing. Her calcium plummeted alongside it because the body cannot properly regulate calcium when magnesium is critically low. She recovered within hours of intravenous replacement, and reported that muscle cramps she had been experiencing for months, which she had not connected to a deficiency, disappeared entirely once she started oral supplements. The balance between sodium, potassium, and magnesium matters for everything from heart rhythm to muscle function, and GI side effects like vomiting and diarrhea can drain electrolytes faster than a reduced diet replaces them.
| Nutrient | Deficiency Rate (12 months) | Primary Risk Factor | Suggested Supplement Form |
|---|---|---|---|
| Vitamin D | 13.6% | Fat sequestration + reduced intake | D3 (cholecalciferol), 4,000-7,000 IU/day |
| Iron | 4% (anemia) | Impaired absorption + reduced intake | Ferrous bisglycinate or iron polysaccharide |
| Vitamin B12 | 2.6% (B vitamins) | Reduced dietary intake + GI effects | Methylcobalamin, 1,000 mcg/day |
| Magnesium | Underreported | GI losses + reduced intake | Magnesium glycinate or citrate, 200-400 mg/day |
| Calcium | Secondary to magnesium | Reduced intake + impaired absorption | Calcium citrate, 500-600 mg/day |
| Zinc | Flagged as at-risk | Reduced intake from protein foods | Zinc picolinate, 15-30 mg/day |
Protein Supplementation and the Muscle Protection Problem
Here is the number that should concern every person considering or currently taking a GLP-1 medication: in the landmark STEP-1 trial of semaglutide, 39 percent of the total weight lost came from lean body mass, not fat. Tirzepatide performed somewhat better at 24 percent lean mass loss, but that still means roughly a quarter of the weight you lose on these medications can come from the muscle, bone, and organ tissue your body needs.
To put that in perspective, researchers have estimated that the lean mass lost during a 68-week course of GLP-1 therapy can approximate two decades of age-related muscle loss compressed into just over a year. That is a serious trade-off, and it is why protein supplementation is not optional for most people on these medications. It is a core part of making the therapy safe long-term.

The joint advisory from the American Society for Nutrition and three other organizations set the protein target at 1.2 to 1.6 grams per kilogram of body weight daily during active weight loss, translating to roughly 80 to 120 grams per day for most adults. Yet data from GLP-1 user cohorts show that only about 43 percent manage to hit even the lower end of that target. When your appetite is suppressed and nausea makes large meals unappealing, getting enough protein through whole foods alone becomes genuinely difficult.
That is where supplementation becomes practical. Whey protein, at 20 to 40 grams per serving, delivers a concentrated dose of leucine, the amino acid that most directly stimulates muscle protein synthesis. For people who cannot tolerate dairy, plant-based blends that combine pea and rice protein offer a comparable amino acid profile. The key is consistency: hitting your daily target matters more than the specific protein source.
Two additional supplements deserve attention. Creatine monohydrate at 5 grams daily adds roughly 1.1 kilograms of lean body mass when paired with resistance training. Beta-hydroxy-beta-methylbutyrate (HMB) at 3 grams daily activates the mTOR pathway driving muscle protein synthesis while inhibiting breakdown. HMB evidence is still emerging, but the mechanistic rationale has earned it a place in several recommended protocols.
The non-negotiable pairing: Protein supplementation alone is unlikely to preserve muscle mass without concurrent resistance training. A case series of patients on GLP-1 medications who combined high protein intake with structured resistance training three to five days per week not only prevented lean tissue loss but actually gained muscle, even while losing 13 to 33 percent of their body weight.
| Supplement | Dose | Evidence Level | Key Benefit |
|---|---|---|---|
| Whey protein | 20-40 g/day | Strong | Preserves lean body mass, high leucine content |
| Creatine monohydrate | 5 g/day | Moderate | +1.1 kg lean mass with resistance training |
| HMB | 3 g/day | Emerging | Stimulates mTOR, inhibits muscle breakdown |
| Total protein target | 1.2-1.6 g/kg/day | Strong (advisory) | 80-120 g/day absolute for most adults |
Supporting Your Gut Through the Adjustment Period
The GI side effects of GLP-1 medications do more than cause temporary discomfort. Delayed gastric emptying, altered intestinal transit, and reduced food variety shift the composition of your gut microbiome, with downstream effects on nutrient absorption and immune function.
Fiber
Most GLP-1 medication users average about 14.5 grams of fiber daily, roughly half the recommended 25 to 38 grams. Fiber feeds beneficial bacteria that produce short-chain fatty acids like butyrate, supporting the intestinal lining and regulating inflammation. Research shows fiber supplementation above 10 grams daily for at least four weeks significantly improves stool frequency and consistency, directly addressing the constipation that affects up to 24 percent of users. Psyllium husk is a well-tolerated option. Start with a small dose, increase gradually, and always pair with additional water.
Probiotics
Probiotic supplementation serves a dual purpose during GLP-1 therapy. Lactobacillus and Bifidobacterium strains improve bowel regularity and reduce bloating, addressing immediate digestive discomfort. But these bacteria also produce butyrate that stimulates GLP-1 secretion from intestinal L-cells, potentially supporting the medication's own mechanism. Doses of 10 to 30 billion CFUs daily appear effective. Look for multi-strain formulations rather than single-strain products.
Omega-3 Fatty Acids
Omega-3 supplementation at a minimum of 1 gram daily received strong evidence ratings. Beyond cardiovascular protection, omega-3s protect skeletal muscle through anti-inflammatory pathways, which becomes relevant when rapid weight loss triggers systemic inflammation. They also support gut lining integrity. If you are eating less of everything, as most GLP-1 users are, supplementation fills an important gap. For a deeper look at omega-3 benefits and how to choose the right supplement, check our full guide.
Bone Health: The Concern Nobody Talks About
Your skeleton adapts to carry a certain load. When that load drops rapidly, bone remodeling shifts toward resorption, removing more bone than it builds. A randomized trial of 195 adults with obesity compared exercise alone, liraglutide alone, the combination, and placebo. Liraglutide alone decreased bone mineral density at the hip and spine. But combining exercise with liraglutide preserved bone density at all three sites, despite this group losing the most weight at nearly 17 kilograms.
For supplementation, calcium citrate is preferred over carbonate for GLP-1 users because it does not require stomach acid for absorption, and delayed gastric emptying reduces available acid. Split calcium into two doses of 500 to 600 milligrams for better absorption. Vitamin K2 also deserves consideration: it directs calcium into bones rather than arteries, an important distinction when supplementing calcium. Learn more about this mechanism in our article on vitamin K2 and arterial calcification.
| Bone Support Factor | GLP-1 Alone | GLP-1 + Exercise + Supplements |
|---|---|---|
| Hip BMD | Decreased | Preserved |
| Spine BMD | Decreased | Preserved |
| Forearm BMD | No significant change | Slight increase |
| Total weight loss | 13.7 kg | 16.9 kg |
| Fracture risk | Potentially elevated | Mitigated |
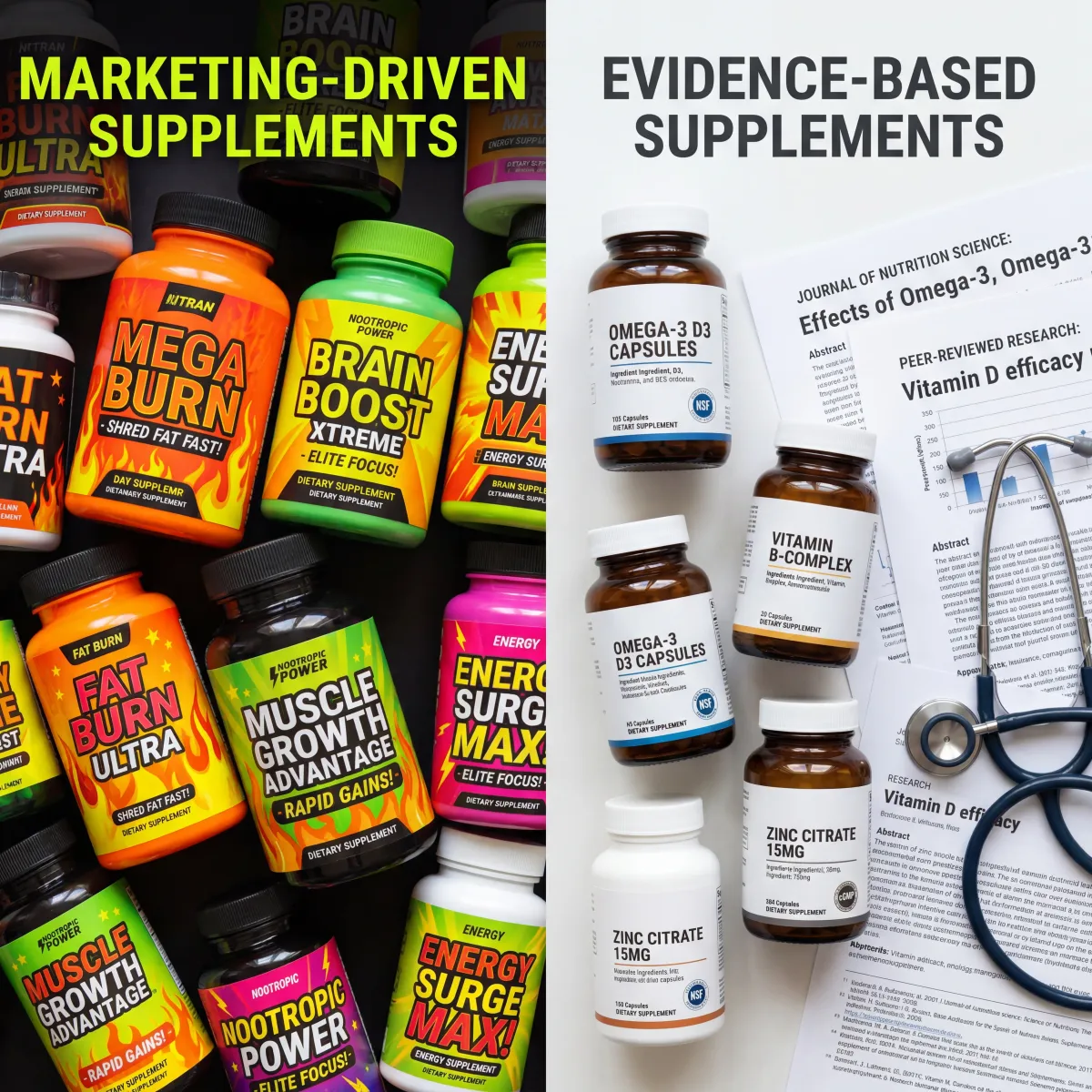
Myths vs. Evidence: What You Actually Need vs. What Gets Marketed
Millions of new customers worried about nutritional gaps create a lucrative market, and supplement claims have gotten ahead of the science. Here is where the evidence actually stands.
| Claim | Reality | Evidence |
|---|---|---|
| You need a specialized GLP-1 supplement pack | No clinical trials support branded GLP-1 supplement bundles over standard targeted supplementation | No direct evidence |
| Biotin prevents hair loss on GLP-1 meds | Hair thinning on GLP-1 drugs is likely telogen effluvium from rapid weight loss, not biotin deficiency. No evidence biotin supplements help | Weak |
| Collagen supplements prevent skin sagging | Some evidence for skin elasticity, but no studies specifically during GLP-1 weight loss | Indirect only |
| You should avoid all supplements with GLP-1 meds | Most supplements are safe, but timing matters: take supplements 1-2 hours before GLP-1 injection day or during meals when tolerated | Clinical guidance |
| Detox supplements help GLP-1 side effects | No evidence. GI side effects are caused by the medication mechanism, not toxins | No evidence |
| Thermogenic fat burners boost GLP-1 results | Caffeine and green tea extract may increase energy expenditure by about 5%, but no studies show additive benefit with GLP-1 meds | Limited, not GLP-1 specific |
The supplements with the strongest evidence base, vitamin D, protein, omega-3s, fiber, and a basic multivitamin-mineral, are not exotic or expensive. The fancy formulations marketed specifically for GLP-1 users often repackage these same ingredients at premium prices. Meanwhile, research found that while 96 percent of consumers were taking supplements, only 12 percent had received any provider recommendation about what to take. Your money is better spent on straightforward, well-dosed versions of the nutrients the research actually identifies as being at risk.
Building a Practical Supplement Stack
Here is a tiered approach based on evidence strength. Start with the foundation and add layers based on your situation, lab work, and how your body responds.
Foundation (Recommended for Most GLP-1 Users)
A quality multivitamin-mineral covers the broad spectrum of at-risk nutrients. Look for one with adequate vitamins A, C, D, E, K, B-complex, iron, zinc, and magnesium in a bioavailable form.
Calculate protein needs at 1.2 to 1.6 grams per kilogram daily. For an 80-kilogram person, that is 96 to 128 grams per day. Track your food intake, supplement the gap with whey protein, and add creatine monohydrate at 5 grams daily alongside resistance training.
Targeted Additions (Based on Lab Work or Symptoms)
Vitamin D3 at 4,000 to 7,000 IU daily if blood levels are below 40 ng/mL. Iron if labs show low ferritin or hemoglobin, using ferrous bisglycinate for better absorption. Vitamin B12 at 1,000 mcg daily if levels are trending down. Calcium citrate at 500 to 600 mg twice daily if intake is low or bone density warrants it.
GI Support (As Needed)
Fiber starting at 5 grams daily, increasing toward 15 to 20 grams for constipation. Probiotics at 10 to 30 billion CFUs daily for digestive regularity. Omega-3 fish oil at 1 gram or more daily for anti-inflammatory and muscle-protective benefits.
Timing tip: GLP-1 medications slow gastric emptying, which can affect how quickly supplements dissolve and get absorbed. Taking your supplements with a meal when possible improves tolerance and absorption. If nausea is a problem around injection days, consider taking your supplements at the opposite end of the day from when symptoms tend to peak.
Frequently Asked Questions
Can I take supplements at the same time as my GLP-1 injection?
Yes, there are no known direct interactions between GLP-1 receptor agonists and standard supplements. Because these medications slow gastric emptying, oral supplements may take longer to absorb. Taking them with a meal helps. If you experience nausea around injection days, space supplements to a different time.
How soon after starting a GLP-1 medication should I begin supplementing?
Ideally, from the start. The joint advisory recommends baseline nutritional screening before initiating therapy. Since deficiency rates climb significantly between six and twelve months, starting a multivitamin, adequate protein, and vitamin D from day one is a reasonable preventive strategy.
Is a multivitamin enough or do I need individual supplements?
A multivitamin covers the basics but typically falls short on the nutrients most at risk. Most contain only 400 to 1,000 IU of vitamin D versus the 4,000 to 7,000 IU the evidence supports, and none provide meaningful protein, omega-3s, or fiber. Think of the multivitamin as a safety net and add targeted supplements based on your labs and symptoms.
Will supplements interfere with how well my GLP-1 medication works for weight loss?
No. These supplements support your health without counteracting the medication's appetite-suppressing mechanism. Protein adds calories, but those calories preserve muscle, which improves long-term metabolic outcomes and makes it easier to maintain weight loss after the medication is reduced or stopped.
Should I be worried about hair loss on GLP-1 medications, and can supplements help?
Hair thinning during rapid weight loss is usually telogen effluvium, a temporary condition that resolves within six to twelve months. Biotin is heavily marketed for this, but no evidence supports it when a true deficiency is absent. Ensuring adequate protein, iron, and zinc through the foundational strategy above addresses the most likely nutritional contributors to hair health.
Related Articles
- How to Prevent Muscle Loss on GLP-1 Medications - A deep dive into resistance training protocols and protein strategies specifically designed for people on semaglutide and tirzepatide.
- GLP-1 Weight Loss Drugs Safety Guide - Everything you need to know about the safety profile, side effects, and monitoring requirements for GLP-1 receptor agonists.
- Electrolytes: Understanding Sodium, Potassium, and Magnesium - A comprehensive guide to the electrolytes most at risk during GLP-1 therapy and how to keep them balanced.
- Vitamin D Benefits, Deficiency Warnings, and Precautions - Why vitamin D deficiency is the most common nutritional shortfall on GLP-1 medications and how to address it.
- Omega-3 Benefits, Sources, and Supplements - The anti-inflammatory and muscle-protective benefits of omega-3s that make them especially valuable during rapid weight loss.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











