Your body needs only tiny amounts of vitamin B12 each day. About 2.4 micrograms, barely visible as a speck of dust. But that microscopic quantity keeps a lot going: building DNA, protecting nerve fibers, producing healthy red blood cells, even helping regulate your mood. When B12 runs short, the fallout touches almost every system in your body, sometimes in ways that look like other conditions entirely.
B12 deficiency rarely announces itself with one clear symptom. It creeps in gradually. A bit more fatigue here, some tingling in the fingers there, and by the time you notice, the damage may already be significant. An estimated 5 to 7 percent of younger adults carry low B12 levels, while functional deficiency affects between 10 and 30 percent of people over 65. And certain groups face far steeper odds than the general population.
Below, we cover what B12 actually does, the symptoms that signal a shortfall, which groups face the highest risk, and what you can do about it.
Why B12 Matters More Than You Think
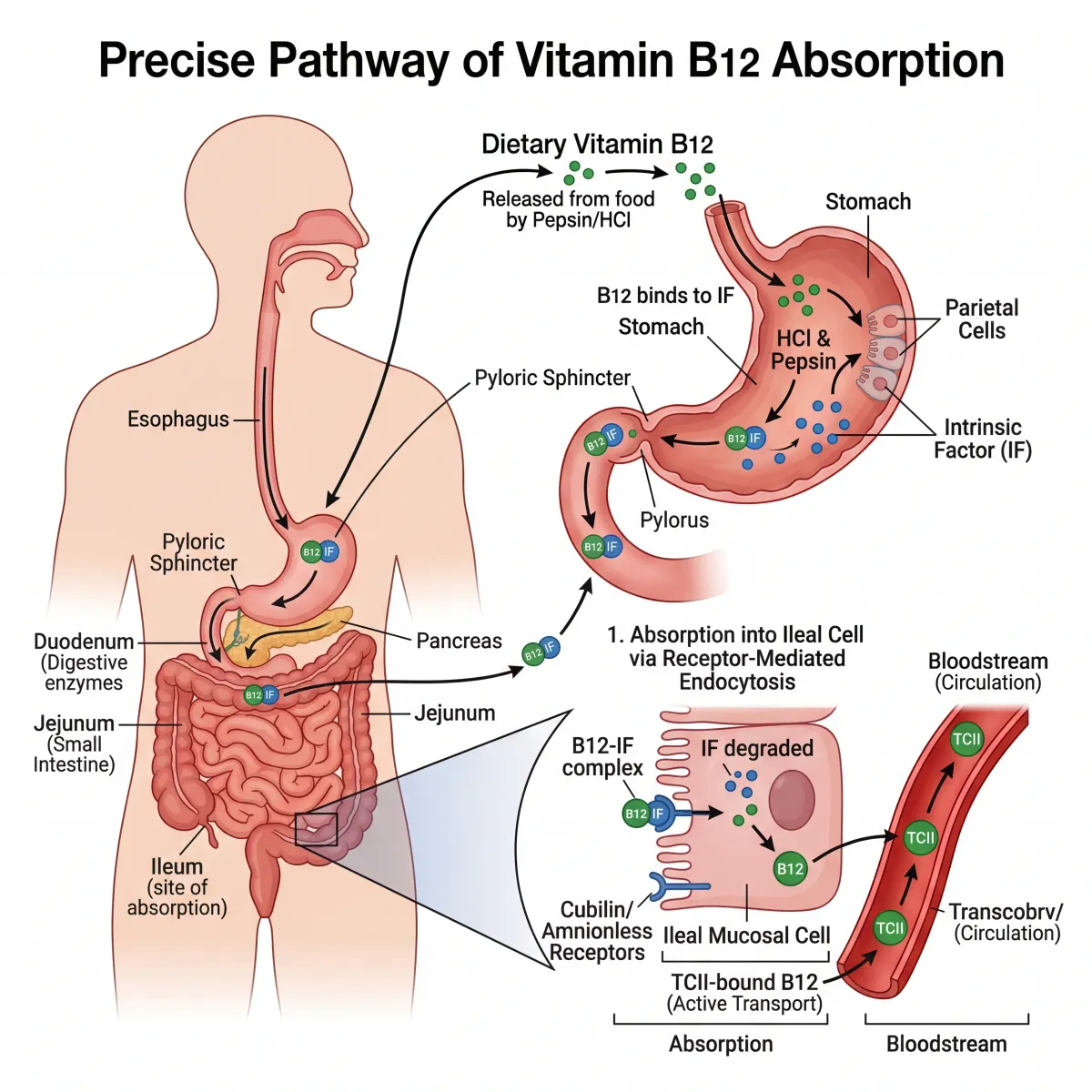
Vitamin B12 (also called cobalamin) is a water-soluble vitamin found in animal-based foods: meat, fish, eggs, and dairy. What makes B12 unusual is its absorption pathway. It depends on stomach acid, a specialized protein called intrinsic factor, and a healthy small intestine. Break any one of those three links and you have a problem.
Once absorbed, B12 does two things that matter a lot. First, it works as a cofactor for methionine synthase, the enzyme that converts homocysteine into methionine. This reaction is essential for DNA synthesis. Without it, your body cannot produce new cells at normal speed, which is why B12-deficient people often develop oversized, immature red blood cells (megaloblastic anemia). The homocysteine that piles up when this conversion stalls is also independently linked to cardiovascular risk.
Second, B12 is required for myelin production, the fatty sheath that insulates your nerve fibers and lets electrical signals travel efficiently. When B12 is insufficient, myelin degrades, and nerve communication slows or misfires. This is why neurological symptoms can be among the earliest and most serious consequences of deficiency, sometimes appearing years before any blood abnormality shows up on routine testing.
Key point: Your liver stores enough B12 to last 3 to 5 years. This is why deficiency develops slowly and why someone can eat a B12-depleted diet for a long time before symptoms surface.
| B12 Function | What It Does | What Goes Wrong Without It |
|---|---|---|
| DNA synthesis | Enables cell division and growth | Megaloblastic anemia, impaired cell production |
| Myelin maintenance | Protects nerve fibers | Neuropathy, balance problems, cognitive decline |
| Homocysteine regulation | Converts homocysteine to methionine | Elevated homocysteine, cardiovascular risk |
| Red blood cell formation | Supports normal erythropoiesis | Fatigue, pallor, shortness of breath |
| Neurotransmitter support | Involved in serotonin and dopamine pathways | Depression, irritability, mood disturbances |
The Warning Signs Your Body Sends When B12 Runs Low
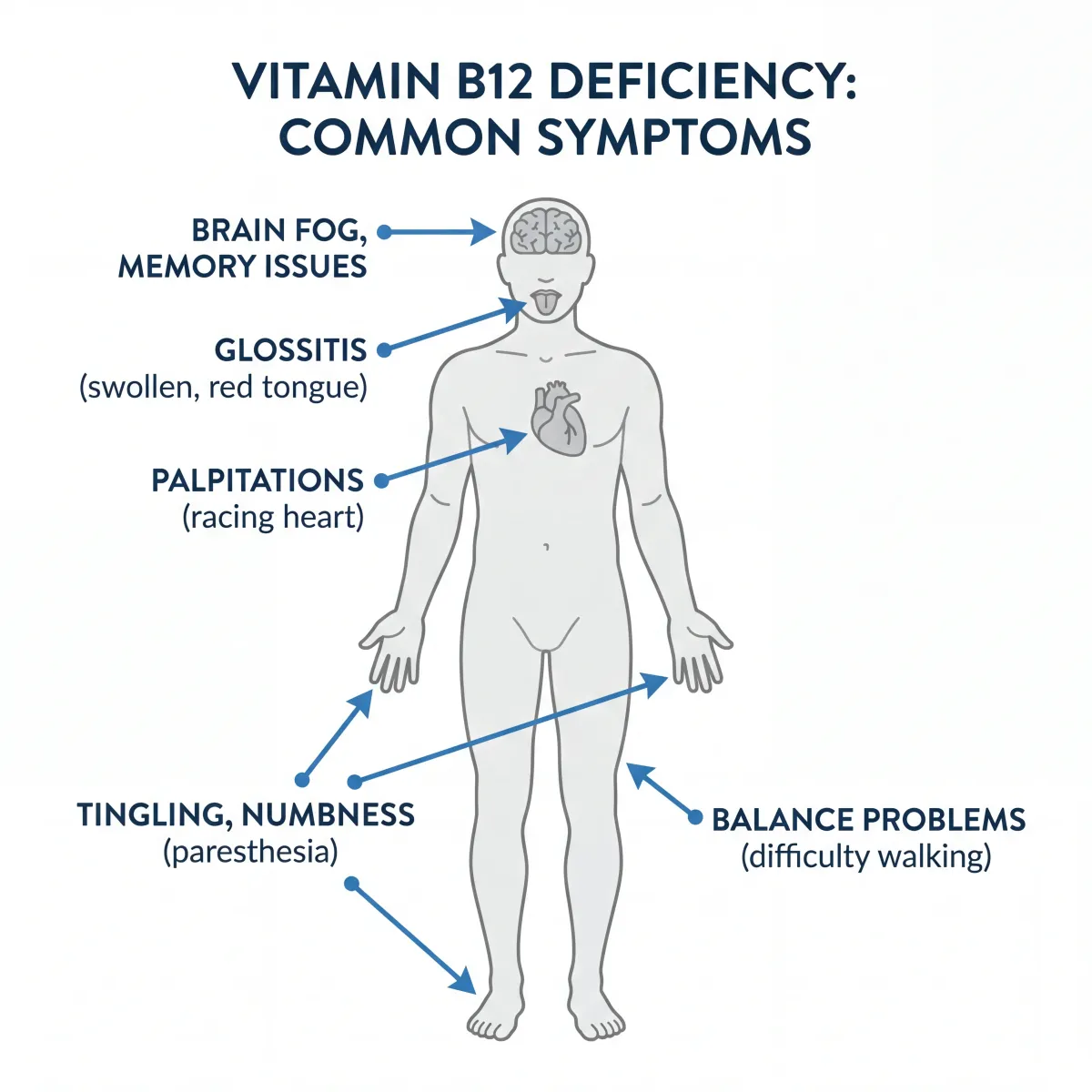
B12 deficiency symptoms fall into three overlapping categories: blood-related, neurological, and psychological. The tricky part is that they look like dozens of other conditions. You might write off fatigue as poor sleep, tingling hands as carpal tunnel, brain fog as stress, and never think to check B12 levels.
The clinical presentations of vitamin B12 deficiency are "highly variable", according to NICE evidence reviews, which makes awareness of the full symptom spectrum especially important.
Blood-Related Symptoms
Because B12 is essential for DNA synthesis in rapidly dividing cells, red blood cells are among the first casualties. Deficiency produces abnormally large red blood cells that cannot carry oxygen efficiently, leading to:
- Persistent fatigue and weakness
- Pale or yellowish skin (jaundice from increased red blood cell breakdown)
- Shortness of breath, especially during physical activity
- Heart palpitations
- Glossitis (a smooth, swollen, sometimes painful tongue)
Neurological Symptoms
Nerve-related symptoms can be the most concerning because they may become permanent if left untreated. The degradation of myelin, a process called subacute combined degeneration of the spinal cord, affects the dorsal columns and lateral tracts of the spinal cord, producing:
- Numbness or tingling in the hands and feet (peripheral neuropathy)
- Difficulty walking or maintaining balance (ataxia)
- Loss of proprioception (trouble sensing where your limbs are in space)
- Vision changes from optic nerve damage
- Muscle weakness
Cognitive and Psychological Symptoms
B12's role in neurotransmitter production means deficiency can mimic psychiatric conditions:
- Memory problems and difficulty concentrating
- Depression and irritability
- Confusion and disorientation
- In severe, prolonged cases: hallucinations, delusions, and dementia-like symptoms
Critical finding: Neurological symptoms from B12 deficiency can precede hematological anomalies by years. This means you can have significant nerve damage with a normal-looking blood count.
| Symptom Category | Early Signs | Advanced Signs |
|---|---|---|
| Blood-related | Fatigue, pallor, mild shortness of breath | Severe anemia, jaundice, heart failure |
| Neurological | Tingling in extremities, mild balance issues | Loss of proprioception, spinal cord degeneration, paralysis |
| Cognitive | Brain fog, difficulty concentrating | Dementia-like symptoms, personality changes, psychosis |
| Gastrointestinal | Glossitis, appetite changes | Weight loss, diarrhea, mouth sores |
Who's Most at Risk for B12 Deficiency?
B12 deficiency hits some groups much harder than others. Knowing who is most vulnerable can mean catching it early instead of dealing with irreversible damage.
Vegans and Vegetarians
Since B12 is found almost exclusively in animal products, anyone following a plant-based diet without supplementation faces the highest dietary risk. A scoping review of 70 studies found that 52 percent of vegan individuals had deficient B12 concentrations compared to just 1 percent of omnivores. Subnormal B12 status affects between 50 and 70 percent of vegetarians and vegans across studies from six countries.
A separate literature review analyzing 18 studies found that vegetarian pregnant women had a 62 percent deficiency rate, and vegetarian children showed rates between 25 and 86 percent. The researchers concluded that "vegetarians develop B12 depletion or deficiency regardless of demographic characteristics, place of residency, age, or type of vegetarian diet."
A strict vegan diet can deplete the body's B12 reserves within approximately three years if no supplementation is used.
Adults Over 65
Aging itself creates B12 absorption challenges. Stomach acid production declines with age, and gastric acid is necessary to liberate B12 from the food proteins it's bound to. Atrophic gastritis, a thinning of the stomach lining that reduces acid output, affects a significant portion of older adults and further impairs absorption. Functional B12 deficiency affects between 10 and 30 percent of individuals over 65.
People Taking Certain Medications
Several commonly prescribed drugs interfere with B12 absorption or metabolism:
| Medication | Mechanism of B12 Interference | Risk Level |
|---|---|---|
| Metformin (diabetes) | Reduces B12 absorption in the ileum; higher doses and longer treatment increase risk | Well-established |
| Proton pump inhibitors | Suppress stomach acid needed to release B12 from food | Moderate (with long-term use) |
| H2 receptor blockers | Reduce gastric acid secretion | Moderate |
| Some antiseizure drugs | Reduce circulating B12 levels through unclear mechanisms | Under investigation |
People With Gastrointestinal Conditions
Conditions that damage the stomach or small intestine directly impair B12 absorption: Crohn's disease (especially involving the terminal ileum), celiac disease, and chronic inflammatory bowel conditions. Surgical procedures including gastric bypass, sleeve gastrectomy, and ileal resection also reduce or eliminate absorption capacity.
People With Autoimmune Conditions
Pernicious anemia, the classic autoimmune cause of B12 deficiency, occurs when the immune system attacks the stomach cells that produce intrinsic factor. It typically affects people aged 60 to 80 of Northern European descent, with an estimated prevalence of 151 per 100,000 in the United States. People with other autoimmune conditions like thyroid disease including Hashimoto's, Sjögren's syndrome, and type 1 diabetes also face elevated risk.
Recreational Nitrous Oxide Users
An increasingly recognized risk group: nitrous oxide inactivates B12 by oxidizing its cobalt center, rendering the vitamin non-functional even when blood levels appear normal. Evidence reviews have flagged this as "a significant public health issue" because standard serum B12 tests may miss the functional deficiency entirely.

How B12 Deficiency Is Actually Diagnosed
Diagnosing B12 deficiency is less straightforward than running a single blood test. The standard serum B12 test has significant limitations that both patients and clinicians should understand.
Serum B12 Levels: The Starting Point
A basic serum B12 test provides a general snapshot:
| Serum B12 Level | Interpretation | Next Steps |
|---|---|---|
| Above 300 pg/mL | Normal | No further testing typically needed |
| 200-300 pg/mL | Borderline (gray zone) | Functional testing recommended |
| Below 200 pg/mL | Deficient | Treatment and cause investigation |
The problem is that serum B12 has been described in clinical literature as "a late, relatively insensitive and unspecific biomarker". It can appear normal even when your cells are already starving for functional B12.
Functional Biomarkers: The Better Picture
For a more accurate assessment, clinicians can measure:
- Methylmalonic acid (MMA): Elevated when cells cannot use B12 properly. More specific to B12 than homocysteine and useful in the "gray zone" of borderline serum B12.
- Homocysteine: Also rises in B12 deficiency but can be elevated by folate deficiency too, so it is less specific on its own.
- Holotranscobalamin (holoTC): Considered the "earliest marker of vitamin B12 deficiency", measuring the biologically active fraction of B12 in blood. Not yet standard in all clinical settings.
If both MMA and homocysteine are elevated while serum B12 sits in the borderline range, functional B12 deficiency is very likely — even if a standard blood panel looks unremarkable.
Finding the Cause
Once deficiency is confirmed, identifying the underlying cause matters for treatment. Anti-intrinsic factor antibody testing can confirm pernicious anemia. A complete dietary history, medication review, and evaluation for GI conditions like celiac or Crohn's disease round out the workup.
Myths vs Facts About Vitamin B12
| Myth | Fact |
|---|---|
| "If your blood count is normal, you can't have B12 deficiency." | Neurological damage from B12 deficiency can develop years before anemia appears on blood tests. A normal CBC does not rule out B12 deficiency. |
| "B12 deficiency only affects vegans." | While vegans face the highest dietary risk, older adults, people on metformin or PPIs, those with GI conditions, and people with autoimmune disorders are all at elevated risk regardless of diet. |
| "You'd know if you were B12 deficient — the symptoms are obvious." | Symptoms develop gradually over months to years. Many people attribute fatigue, tingling, or mood changes to aging, stress, or other conditions and never suspect B12. |
| "Oral supplements can't work if you have absorption problems." | Research shows that high-dose oral B12 (1,000-2,000 mcg daily) can be effective even in people with impaired intrinsic factor, because approximately 1% of B12 is absorbed through passive diffusion regardless of intrinsic factor. |
| "Energy drinks and B12 shots will boost energy in everyone." | B12 supplementation improves energy only if you are actually deficient. In people with adequate B12 levels, extra B12 provides no additional energy boost. |
Treating and Preventing B12 Deficiency
How you treat B12 deficiency depends on why it developed. The two main routes are oral supplements and intramuscular injections, and the choice between them is less rigid than older guidelines suggested.
For Dietary Deficiency
If the cause is inadequate intake (vegans, vegetarians, restrictive diets), oral supplementation is straightforward and effective. A daily dose of 50 to 100 micrograms is generally recommended for maintenance and prevention. For those who prefer less frequent dosing, a weekly dose of 2,000 mcg is an alternative approach.
Fortified foods — nutritional yeast, fortified plant milks, fortified cereals — can contribute but are difficult to rely on as a sole source because intake amounts are inconsistent.
For Absorption-Related Deficiency
When the problem is intrinsic factor deficiency (pernicious anemia) or GI surgery, the traditional approach uses intramuscular injections of 1,000 mcg: weekly for the first four weeks to replenish stores, then monthly for maintenance. Many people with pernicious anemia require lifelong injections.
However, emerging evidence has challenged the assumption that injections are always necessary. At sufficiently high oral doses (1,000 to 2,000 mcg daily), enough B12 crosses the intestinal wall through passive diffusion (about 1 percent of the dose) to achieve therapeutic levels even without intrinsic factor. This approach is gaining acceptance in clinical practice, though injections remain the standard when rapid repletion is needed.
Forms of B12
Supplements come in several forms: cyanocobalamin (the most stable and well-studied), methylcobalamin (a naturally occurring form), hydroxocobalamin (used in injections in many countries), and adenosylcobalamin. Cyanocobalamin remains the most commonly recommended for supplementation due to its stability and extensive safety data.
Prevention for At-Risk Groups
Prevention is simpler and safer than treating established deficiency after nerve damage has already set in. If you fall into any high-risk category:
- Vegans and vegetarians: Supplement with B12 daily (50-100 mcg) or take a weekly larger dose (2,000 mcg). Non-negotiable.
- Adults over 65: Discuss B12 screening with your clinician. Because absorption from food declines with age, supplementation may be warranted even with an omnivorous diet.
- Long-term metformin users: Request periodic B12 monitoring (every 2-3 years at minimum).
- Long-term PPI users: Same monitoring recommendation.
- Post-bariatric surgery patients: Lifelong B12 supplementation and monitoring is standard care.
If you are concerned about your own nutritional status, a conversation with your healthcare provider about targeted blood work is the most reliable starting point.
Frequently Asked Questions
How long does it take for B12 deficiency symptoms to appear?
Because the liver stores 3 to 5 years' worth of B12, symptoms typically develop gradually over several years after intake or absorption drops. Some people remain asymptomatic for even longer before noticeable problems emerge, which is why deficiency is often caught late.
Can B12 deficiency cause permanent damage?
Yes. If neurological symptoms like peripheral neuropathy, balance problems, or cognitive changes go untreated for too long, the nerve damage can become irreversible. Younger patients and those treated early generally recover more fully than older patients with long-standing deficiency.
Is a blood test enough to diagnose B12 deficiency?
A standard serum B12 test is a reasonable first step, but it can miss functional deficiency — especially in the borderline range (200-300 pg/mL). Methylmalonic acid and homocysteine tests provide a more complete picture. If your serum B12 is borderline and you have symptoms, ask about these additional markers.
Do I need B12 injections, or will pills work?
For most people with dietary deficiency, oral supplements are effective. Even people with absorption problems can often respond to high-dose oral B12 (1,000-2,000 mcg daily) because a small percentage crosses the intestinal wall through passive diffusion. Injections are preferred when rapid repletion is urgent or when oral compliance is a concern.
Can you take too much B12?
Vitamin B12 has no established upper intake limit because excess is excreted in urine. Toxicity from B12 supplementation is extremely rare. However, "more is better" does not apply if you are not deficient — supplementing when your levels are already adequate provides no additional benefit.
Related Articles
- Iron Deficiency in Women: Symptoms, Testing, and Recovery — Another common nutritional deficiency with overlapping symptoms like fatigue and weakness.
- Magnesium Types Explained (Glycinate, Citrate, Threonate) — Which to Take and When — Understanding different supplement forms matters for B12 too.
- Gut-Brain Axis: How Your Microbiome Affects Mood and Cognition — The gut plays a central role in B12 absorption and neurological health.
- Thyroid Health and Hashimoto's: Symptoms, Diet, and Natural Support — Autoimmune thyroid conditions increase B12 deficiency risk.
- Electrolytes Explained: Sodium, Potassium, Magnesium for Hydration — Nutritional balance extends beyond B12 to other essential micronutrients.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











