
Your nose does more than you think while you sleep
Nasal breathing is not just a preference. Your body was designed for it. Humans breathe through their noses from birth, and the reasons run deeper than most people realize.
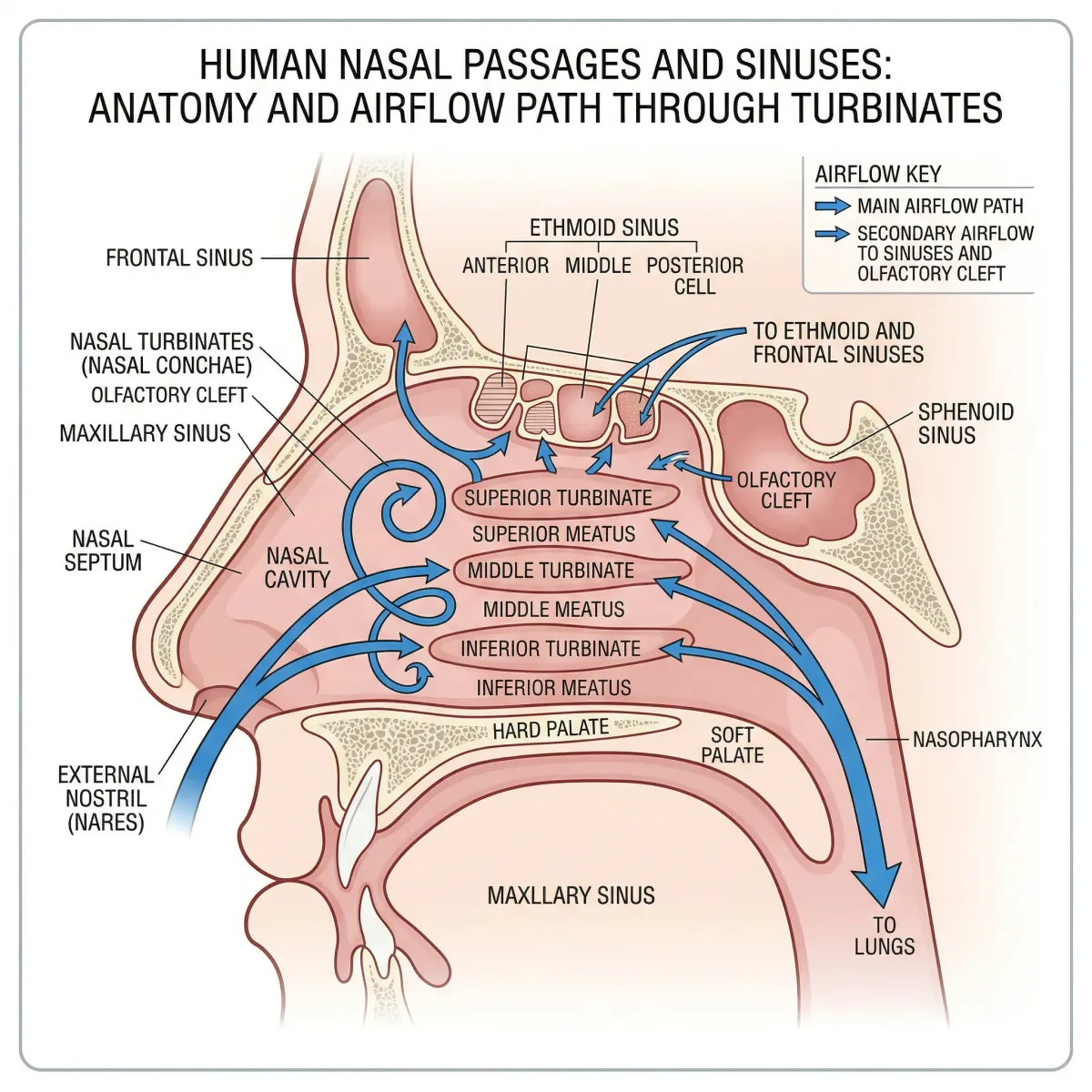
Your nasal passages warm and humidify incoming air before it reaches your lungs. The cilia lining your nose trap particulates, bacteria, and allergens, sending them down your throat to your stomach rather than into delicate lung tissue. Your mouth offers none of these protections. When you breathe through your mouth at night, air arrives at your lungs cold, dry, and unfiltered.
The most surprising function is not filtration at all. Your paranasal sinuses continuously produce nitric oxide (NO) at concentrations around 10 parts per million. During nasal inhalation, this NO is carried into your bronchi and lungs, where it acts as a vasodilator (opening blood vessels), a bronchodilator (opening airways), and an antimicrobial agent. NO also activates ciliary movement and mucus secretion, increasing the removal of dust and pathogens from your respiratory tract.
A study in Acta Physiologica Scandinavica measured something surprising: transcutaneous oxygen was roughly 10% higher during nasal breathing compared to oral breathing in six of eight healthy subjects. Ten percent more oxygen, just from breathing through your nose instead of your mouth.
Mouth breathers miss all of this. Research shows they have lower levels of nitric oxide within their respiratory tracts compared to nasal breathers, and studies suggest that people who breathe through their mouths during sleep are more prone to upper respiratory tract infections.
What mouth taping actually involves
The concept could not be simpler: you stick a strip of medical-grade adhesive tape across your lips before bed to keep your mouth closed, routing all breathing through your nose. Social media pushed this practice into the mainstream, with claims ranging from better sleep to jawline improvements to anti-aging effects.
Most proponents recommend hypoallergenic surgical tape, specifically 3M silicone tape cut to about 4 centimeters, placed vertically on the philtrum spanning upper and lower lips. The tape should be easy to remove. You should be able to open your mouth if necessary, even with the tape in place. Some dedicated mouth-tape products use porous materials that allow limited airflow if the lips part slightly.
The reasoning holds together on paper: mouth breathing worsens sleep, nasal breathing improves it, so keeping the mouth shut should help. But does the evidence back it up? And for whom?
What the studies actually found
The honest answer starts with a caveat. A 2025 systematic review published in PLOS ONE screened 120 articles and found only 10 that met inclusion criteria, encompassing 213 total patients. Every one of those 10 studies was rated poor quality on the Newcastle-Ottawa Scale. That is the evidence base we are working with.
The positive results
The most-cited study comes from Chang Gung Memorial Hospital in Taiwan. Lee and colleagues enrolled 20 mouth-breathers with mild obstructive sleep apnea (OSA) and had them use 3M silicone tape for one week. Their median apnea-hypopnea index (AHI) dropped from 8.3 to 4.7 events per hour, a 47% reduction. The snoring index fell from 303.8 to 121.1 events per hour. Oxygen desaturation improved. Thirteen of 20 patients (65%) were classified as responders, meaning their snoring index dropped by at least half.
An earlier pilot study by Huang and colleagues using porous oral patches showed similar results: AHI dropped from 12 to 7.8 in 30 patients with mild OSA. Sleepiness scores and snoring severity also improved.
The strongest evidence came in late 2025 from a randomized crossover trial in the Journal of Clinical Sleep Medicine. Meksukree and colleagues studied 62 patients using mouth tape alongside CPAP therapy. Average CPAP use increased by 51.8 minutes per day, and the odds of achieving good CPAP adherence were 4.5 times higher with mouth tape. Daytime sleepiness, snoring, and throat dryness all improved. But this was mouth tape as a CPAP add-on, not a standalone treatment.
The limits of those results
The two standalone mouth-taping studies (Lee and Huang) only included patients with mild OSA. An AHI shift from 8.3 to 4.7 moves someone from "mild" to "borderline normal," which is a meaningful improvement for that specific person but raises questions about clinical significance more broadly. Both studies excluded anyone with nasal obstruction, meaning the patients could already breathe through their noses adequately. And both lacked control groups.
Three other studies in the systematic review found no significant AHI improvement from mouth taping alone. One study by Labarca and colleagues only saw AHI improvement when mouth tape was combined with a mandibular advancement device. A 2024 randomized controlled trial by Osman and colleagues found no significant difference between mouth taping and placebo.
| Study | Patients | AHI before | AHI after | Significant? |
|---|---|---|---|---|
| Lee et al. 2022 | 20 (mild OSA) | 8.3 | 4.7 | Yes (p=0.0002) |
| Huang et al. 2015 | 30 (mild OSA) | 12.0 | 7.8 | Yes (p<0.01) |
| Labarca et al. 2022 | 14 | Tape alone: no change | MAD+tape: 5.6 vs 10.5 | Only with MAD |
| Osman et al. 2024 | 71 | 47 (mean) | No change | No |
| Bhat et al. 2015 (chinstrap) | 26 | Various | No change | No |
The systematic review's conclusion was blunt: "The existing data does not support mouth taping or oral occlusion as a sound clinical intervention for the general population with sleep disordered breathing."
Of 10 studies examining mouth taping for sleep, only 2 showed meaningful AHI improvement, both in mild OSA patients without nasal obstruction. All 10 studies were rated poor quality. Four explicitly discussed risks of asphyxiation.
| What mouth taping may help | What mouth taping does not help |
|---|---|
| Mild OSA in confirmed mouth-breathers | Moderate to severe OSA |
| Snoring in people with adequate nasal airways | OSA caused by nasal obstruction |
| CPAP adherence (mouth leak reduction) | Sleep-disordered breathing in general population |
| Morning dry mouth from mouth breathing | Structural airway problems (palatal prolapse) |

Your mouth stays open 97% of the night (and it matters)
The case for mouth taping is shaky. The case against habitual mouth breathing at night is not.
Researchers at Taipei Veterans General Hospital used infrared cameras and airflow sensors during polysomnography to measure how much time people actually spend with their mouths open at night. The numbers are hard to ignore: OSA patients spent 96.7% of total sleep time with their mouths open, compared to 26.7% for healthy controls. Time spent in complete mouth breathing was 14.1% vs. 2.7%.
That open mouth costs the body water. OSA patients with more mouth breathing showed greater nocturnal increases in hematocrit (a measure of blood thickness), losing an estimated 5.5% of plasma volume overnight versus 3.7% for controls. This kind of hemoconcentration is a recognized risk factor for cardiovascular events, and the researchers flagged a possible connection to the pattern of nocturnal ischemic heart attacks in sleep apnea patients.
Mouth breathing also changes the physical dimensions of your airway. When your mouth opens during sleep, your mandible drops and your soft palate shifts backward, narrowing both the retropalatal and retroglossal spaces. Multiple studies using CT imaging and drug-induced sleep endoscopy have confirmed that upper airway collapsibility and resistance are significantly higher in mouth breathers compared to nasal breathers. The narrowing creates a feedback loop: mouth breathing worsens airway collapse, which worsens OSA, which leads to more mouth breathing.
Beyond the airway, chronic mouth breathing at night contributes to:
- Dry mouth and subsequent dental problems (cavities, gingivitis, halitosis)
- Reduced deep sleep and increased daytime fatigue
- In children, associations with ADHD-like symptoms and abnormal craniofacial development
- Increased susceptibility to respiratory infections due to bypassing nasal filtration
People who should steer clear
Cleveland Clinic sleep specialist Dr. Brian Chen is direct about the contraindications. Mouth taping should not be attempted by anyone with:
- Nasal obstruction or chronic congestion
- Chronic allergies or sinus infections
- Enlarged tonsils or adenoids
- A deviated septum
- Moderate to severe obstructive sleep apnea
- Heart conditions
- Anxiety disorders (especially around breathing)
The logic is simple: if your nose cannot handle 100% of your breathing load, sealing your mouth is dangerous. The systematic review found that four of ten studies explicitly discussed the risk of asphyxiation in the presence of nasal obstruction or regurgitation.
A 2024 study by Yang and colleagues, published in JAMA Otolaryngology, revealed something specific and useful. They measured airflow in 54 OSA patients during drug-induced sleep endoscopy. For patients with moderate mouth breathing, mouth closure increased inspiratory airflow by 2.0 L/min. But for patients with high baseline mouth breathing (above 2.2 L/min), closing the mouth actually reduced airflow by 1.86 L/min. The dividing line was soft palate collapse. If the palate is part of the obstruction, taping the mouth compounds the problem.
| Baseline mouth breathing level | Effect of mouth closure on airflow | Recommendation |
|---|---|---|
| Near-zero (<0.05 L/min) | No significant change (+0.9 L/min) | No benefit expected |
| Moderate (0.05-2.20 L/min) | Increased airflow (+2.0 L/min) | Potentially beneficial |
| High (>2.20 L/min) | Decreased airflow (-1.86 L/min) | Harmful — do not tape |
If you want to try it: a practical approach
If you have no nasal obstruction, no known sleep apnea beyond mild, and you are interested in testing mouth taping, here is a sensible approach based on the clinical studies:
Talk to a doctor first. This is not just a formality. Snoring can be the first sign of sleep apnea, and you need to rule out anything that makes mouth taping risky before trying it. A sleep study or at-home sleep test can establish your baseline.
Start during waking hours. Put a strip of tape across your lips while watching television or reading. If you feel anxious or cannot breathe comfortably through your nose, mouth taping is not for you. This trial run lets you assess tolerance without the stakes of being asleep.
Use the right tape. The studies that showed positive results used 3M silicone hypoallergenic tape, cut to roughly 4 centimeters, placed vertically over the philtrum. It should be easy to remove with your tongue if needed. Do not use duct tape, athletic tape, or anything that could irritate skin or be difficult to remove.
Address nasal congestion first. Researchers in the Lee et al. study gave patients with any nasal obstruction medication and nasal spray to improve airflow before introducing mouth tape. Optimizing your baseline health matters.
Keep track of results. Monitor morning dry mouth, snoring (ask a partner or use a sleep-tracking app), and subjective sleep quality. If symptoms worsen or you find the tape dislodged every morning, the intervention is not working.

Alternatives that work without tape
If the goal is more nasal breathing at night, tape is one option among several, and not the one with the best evidence.
Nasal strips and dilators. External nasal strips (like Breathe Right) physically open the nasal valve, reducing airway resistance without sealing the mouth. Internal silicone dilators do the same thing from inside the nostril. Both are less invasive than taping and allow mouth breathing as a safety valve.
Positional therapy. The Lee et al. study found that most of their subjects had positional sleep apnea, worse in the supine position. Simple position changes, like sleeping on your side, can reduce both mouth breathing and apnea events without any device. A tennis ball sewn into the back of a sleep shirt is the classic low-tech solution.
Breathing exercises. Techniques like diaphragmatic breathing, alternate nostril breathing, and box breathing can help retrain your default breathing pattern. Practice during the day, and the habit carries into sleep.
Treat the underlying cause. Chronic nasal congestion from allergies, a deviated septum, or enlarged adenoids/tonsils should be addressed medically. Nasal corticosteroid sprays, antihistamines, or surgical correction (septoplasty, adenoidectomy) resolve mouth breathing at its source rather than working around it.
Myofunctional therapy. This is a program of exercises targeting the muscles of the face, tongue, and throat. Originally developed for swallowing disorders, it has shown promising results for improving tongue posture and promoting nasal breathing during sleep. A trained myofunctional therapist can design a personalized program.
CPAP or oral appliances. For diagnosed sleep apnea, CPAP remains the gold standard. The Meksukree 2025 study showed that mouth tape can complement CPAP by reducing mouth leak, but it is not a substitute for proper treatment.

Frequently Asked Questions
Is mouth taping safe for everyone?
No. People with nasal obstruction, chronic allergies, deviated septums, moderate to severe sleep apnea, or heart conditions should not attempt mouth taping. Even for otherwise healthy people, testing tolerance during waking hours before sleeping with tape is recommended. Four of ten clinical studies on mouth taping explicitly warned of asphyxiation risks.
Does mouth taping actually stop snoring?
In two small studies of patients with mild OSA and confirmed mouth breathing, mouth taping reduced snoring by about 50%. But a 2025 systematic review of all available evidence concluded there is not enough scientific evidence to recommend mouth taping as a snoring treatment for the general population. The improvement appears limited to a specific subgroup: mild snorers who breathe through their mouths despite having adequate nasal airways.
What type of tape should be used for mouth taping?
Clinical studies used 3M silicone hypoallergenic tape, cut to approximately 4 centimeters, placed vertically across the center of the lips. The tape should be easy to remove with your tongue. Dedicated mouth-tape products using porous materials are also available. Never use non-medical tape (duct tape, athletic tape) as it can cause skin damage and be difficult to remove in an emergency.
Can mouth taping replace a CPAP machine?
No. Mouth taping is not a substitute for CPAP in patients with diagnosed obstructive sleep apnea. A 2025 randomized trial showed that mouth tape can improve CPAP adherence by reducing mouth leak and dryness, but it complements rather than replaces the primary treatment. The authors of the 2022 preliminary study specifically stated that mouth taping is only appropriate before turning to CPAP or surgery, not instead of it.
Why does my mouth open during sleep?
Mouth opening during sleep can result from nasal obstruction (congestion, allergies, deviated septum, enlarged adenoids), habitual mouth breathing, or as a symptom of obstructive sleep apnea. Research shows OSA patients spend up to 97% of sleep time with their mouths open. If you consistently wake with a dry mouth or your partner reports mouth breathing, this is worth discussing with a healthcare provider to rule out underlying causes.
Related Articles
- How Sleep Timing (Not Just Duration) Affects Your Heart: What New Research Reveals — Explores the cardiovascular consequences of disrupted sleep patterns, including how sleep-disordered breathing affects heart health.
- Vagus Nerve and Heart Health: New Research on the Nerve That Keeps Your Heart Young — Covers breathing techniques and vagal tone, with practical exercises for better autonomic function during sleep.
- Inflammation and Chronic Disease: A Complete Guide to Anti-Inflammatory Living — Discusses how chronic mouth breathing and poor sleep contribute to systemic inflammation.
- Glycine: The Amino Acid That Improves Sleep, Collagen, and Longevity — Evidence-based approaches to improving sleep quality through supplementation.
- Myo-Inositol: The Supplement Going Viral for Anxiety, Sleep, and Hormonal Health — Covers supplements that may help with sleep anxiety, relevant for those who find mouth taping psychologically uncomfortable.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











