
What Hydrolyzed Collagen Peptides Do in Your Knees
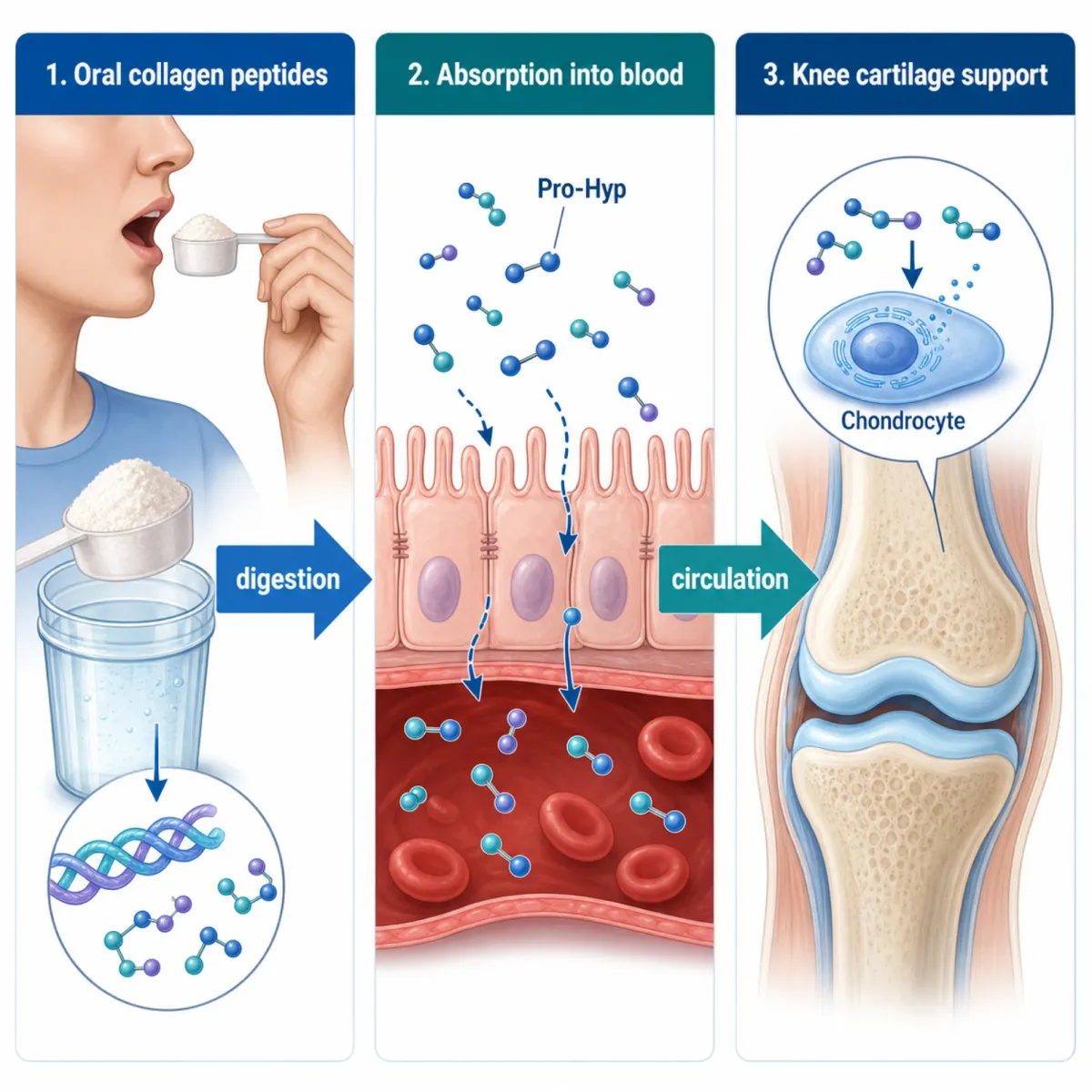
Your knee cartilage is roughly 60% collagen by dry weight, mostly type II. When that network degrades faster than your body rebuilds it, you get the grinding, stiffness, and pain of osteoarthritis. Hydrolyzed collagen peptides are animal collagen broken into small fragments under 6 kilodaltons through enzymatic hydrolysis. Think of it like shredding a rope into its individual fibers — same material, but the pieces are small enough to cross your intestinal wall into the bloodstream.
Researchers have tracked labeled collagen fragments and found that peptides like prolyl-hydroxyproline (Pro-Hyp) show up in blood plasma within an hour and accumulate preferentially in cartilage and bone tissue. Once there, Pro-Hyp stimulates chondrocytes — the cells maintaining cartilage — to produce more type II collagen and proteoglycans.
This is different from undenatured type II collagen (UC-II), which works through an immune mechanism called oral tolerance at just 40 mg daily. Hydrolyzed collagen peptides work through a direct structural pathway — absorbed peptides physically reach cartilage and signal cells to produce more matrix. If you're evaluating collagen for knee pain, you need to know which type was studied, at what dose, and for how long. The three studies below all used hydrolyzed collagen peptides at 10 grams daily.
Study 1: Clark 2008 — 147 Athletes, 24 Weeks, and the Knee Subgroup That Changed the Conversation
Kristine Clark and Wayne Sebastianelli at Penn State ran the first long-duration controlled trial of collagen hydrolysate in active people without diagnosed joint disease. Published in Current Medical Research and Opinion in 2008, the study enrolled 147 varsity and club sport athletes (72 male, 75 female) with activity-related joint pain but no degenerative joint disease. Seventy-three received 10 grams daily of CH-Alpha (by GELITA Health GmbH) as a 25 mL liquid; 74 received an identical xanthan placebo. Both groups continued normal training for 24 weeks.
What They Found
Of 147 enrolled, 97 completed the trial (34% dropout, attributed to student schedules). Among finishers, six pain parameters reached statistical significance: pain at rest physician-assessed (p=0.025), walking (p=0.007), standing (p=0.011), rest self-assessed (p=0.039), carrying objects (p=0.014), and lifting (p=0.018).
The most-discussed finding came from a post-hoc subgroup. Sixty-three subjects (65%) reported knee-specific pain, and when isolated, results sharpened: pain at rest jumped to p=0.001, walking to p=0.003. Two new parameters reached significance: running straight (p=0.027) and changing direction (p=0.026).
Effect size context: Clark reported an effect size of 0.36 for pain when walking across all joints (n=97), increasing to 0.45 in the knee subgroup (n=63). In clinical research terms, 0.2 is considered weak and 0.8 is strong — so these land in the small-to-moderate range. Meaningful? Probably. Dramatic? No.
A secondary finding: at the final visit, placebo athletes had used alternative therapies (acupuncture, hydrotherapy) 39 times versus just 12 times in the collagen group (p<0.001) — suggesting the placebo group felt more compelled to seek additional relief.
| Strength | Limitation |
|---|---|
| 24-week duration (longest at that time) | 34% dropout rate reduces statistical power |
| Proper randomization and blinding | Knee subgroup was post-hoc, not pre-planned |
| Active population (real-world relevance) | Mixed sports, no activity standardization |
| Multiple pain parameters measured | No imaging or biomarker outcomes |
| Physician and self-assessed pain | Funded and product supplied by GELITA |
That last row matters. GELITA Health GmbH sponsored the research and co-author Klaus Flechsenhar worked in GELITA's R&D department. Industry sponsorship doesn't invalidate findings, but the study needs independent corroboration.
Study 2: Benito-Ruiz 2009 — 250 Knee OA Patients in the Largest Trial to Date
Where Clark studied athletes with pain but no disease, P. Benito-Ruiz and colleagues went after the harder population: 250 adults with diagnosed primary knee osteoarthritis across multiple centers in Ecuador. Published in the International Journal of Food Science and Nutrition (2009), it remains the largest single randomized trial of hydrolyzed collagen for knee-specific outcomes. The protocol: 10 grams daily for 6 months versus placebo, measured by VAS, WOMAC pain subscale, and SF-36.

What They Found
The study reported significant improvements in knee joint pain and comfort across VAS and WOMAC assessments in the collagen group compared to placebo. A 2023 meta-analysis in the Journal of Orthopaedic Surgery and Research that included Benito-Ruiz among its four analyzed RCTs noted that the Ecuadorian trial showed "marked improvements in both VAS and WOMAC scores, particularly among severe OA cases."
Two subgroup findings stand out. Patients with more severe joint deterioration saw the greatest benefit — intuitive, since there's more room for improvement. And patients with minimal meat protein in their diets responded better. Collagen lacks tryptophan entirely (PDCAAS of 0), but it delivers glycine, proline, and hydroxyproline at concentrations well above a typical diet. If you already eat plenty of meat, the incremental benefit may be smaller.
| Strength | Limitation |
|---|---|
| Largest sample (N=250) | Granular effect sizes not in accessible abstracts |
| Actual knee OA patients (not just pain) | Industry funder not clearly disclosed |
| Multicenter design reduces site bias | Single geographic population (Ecuador) |
| 6-month duration | Full text less accessible than Clark or Kumar |
Benito-Ruiz provides the strongest evidence here based on sample size and clinical population. The protein-intake subgroup finding is especially relevant for older adults whose diets may already be lower in animal protein.
Study 3: Kumar 2015 — Small Trial, Big Claims, and the Industry Funding Question
Suresh Kumar and colleagues published a double-blind, placebo-controlled trial in the Journal of the Science of Food and Agriculture (2015) testing a question the others didn't: does the collagen source matter? Two parallel studies compared pork skin collagen peptide (PCP) and bovine bone collagen peptide (BCP) against maltodextrin placebo in knee OA patients (Kellgren-Lawrence grade 2-4). Each enrolled 30 subjects (2:1 randomization), with 5 grams twice daily (10g total) for 13 weeks after a 7-day NSAID run-in period.
What They Found
In the PCP study, WOMAC scores dropped from 47.2 to 31.1 — a 34% reduction over 13 weeks — while the placebo group barely moved (47.3 to 45.5, a 3.8% change). VAS pain told a similar story: 63.2 to 31.1 mm in the PCP group (50.8% pain reduction), versus 60.0 to 57.3 in placebo (4.5%). All differences reached P<0.01 by visit 5.
The BCP study mirrored these results: WOMAC dropped 48.7%, VAS fell 57.6%. Both collagen sources performed comparably despite different amino acid profiles. Among PCP-treated subjects, 63.2% met all pre-defined efficacy thresholds versus 0% in placebo.
Why These Numbers Deserve Skepticism
A 50% pain reduction versus near-zero in placebo is unusually large for a supplement trial. With only 19-20 subjects per treatment arm, random variation has outsized influence — a handful of extreme responders can swing group averages. Compare this to Benito-Ruiz's 250 patients.
Then there's funding. Lead author Suresh Kumar listed his affiliation as Nitta Gelatin India Ltd — the manufacturer. Co-authors Sugihara, Suzuki, and Inoue worked at Nitta Gelatin Inc. in Japan. This is a manufacturer testing its own product with its own employees as investigators.
| Strength | Limitation |
|---|---|
| Compared two collagen sources (PCP vs BCP) | Very small sample (N=30 per study, ~20 per arm) |
| Validated outcome measures (WOMAC, VAS) | Manufacturer-conducted study (Nitta Gelatin) |
| Clear dose and protocol description | 2:1 randomization weakens placebo arm |
| Both sources showed similar efficacy | 13 weeks shorter than Clark or Benito-Ruiz |
| Safety data collected | All participants pre-treated with NSAIDs in run-in |
A small manufacturer-funded study showing dramatic effects is a recurring pattern in supplement research and needs independent replication. The finding that both collagen sources performed similarly is genuinely useful — it suggests the source animal may matter less than the hydrolysis process.
What These Three Studies Collectively Show (and Where They Fall Short)
No single study here would survive rigorous scrutiny on its own. Together, though, the pattern is harder to wave away.
All three used 10 grams daily and reported statistically significant pain reduction across different populations — young athletes, middle-aged OA patients in Ecuador, diagnosed OA patients in India. A 2023 meta-analysis pooling 4 RCTs (507 patients) found a standardized mean difference of -0.58 (95% CI: -0.98 to -0.18, p=0.004) for pain reduction.
But that same meta-analysis flagged a problem: all four included studies rated high overall risk of bias under ROB 2.0. GRADE quality was "moderate" for pain. Heterogeneity hit I²=68%.
Where the Evidence Is Strong
The safety profile is consistently reassuring across all three studies and the broader meta-analysis. Adverse events did not differ significantly between collagen and placebo groups (OR 1.66, 95% CI 0.99-2.78, p=0.05). The FDA classifies collagen peptide as Generally Recognized as Safe (GRAS). Reported side effects across all three trials were minor gastrointestinal complaints at worst.
The dose convergence is notable. All three studies independently settled on 10 grams daily, and a 2024 five-arm dose-finding trial by Devasia et al. found a clear dose-response relationship: 10 grams of Type J collagen reduced WOMAC scores by 44.29 points versus 38.57 for 5 grams and 26.30 for 2.5 grams, compared to 5.67 for placebo. That same study measured CTX-II, a biomarker for cartilage degradation, and found it decreased by 34.35% with 10 grams versus 3.1% in placebo — the first strong biomarker evidence that collagen peptides affect cartilage metabolism, not just pain perception.
Where It's Weak
No study used MRI to verify structural cartilage changes. Pain is subjective and susceptible to placebo effects. The largest trial has limited granular data in English abstracts. Independent replications remain scarce. And a 2023 review noted "significant knowledge gaps regarding the digestion, bioavailability, and bioactivity of CH-derived bioactive peptides, and how different CH products compare."
Dosing, Timing, and Practical Considerations
Dose: All three studies used 10 grams daily. A 2021 systematic review of 15 RCTs supports 5-15 grams per day, with at least 3 months needed for observable benefit. Devasia's 2024 dose-finding study confirmed 10 grams outperformed 5 and 2.5 grams on all measures.
Timing: Shaw et al. showed amino acid levels peak about 1 hour after collagen ingestion. If you exercise regularly, taking it 60 minutes before activity aligns with the pharmacokinetics. For sedentary users, consistency matters more than timing.
Duration: Clark didn't see clear group separation until after 12 weeks. Kumar's smaller sample showed significance by week 6. Plan for at least 3 months before judging.
Source: Kumar found pork and bovine collagen equally effective. The Arthritis Foundation notes a meta-analysis of 41 studies found benefit "regardless of dose, type, or brand." However, processing affects which bioactive peptides survive, and the studies here used pharmaceutical-grade products.
What this is not: Hydrolyzed collagen is a nutritional supplement, not a drug. It is not a replacement for physical therapy, weight management, or medical treatment for advancing osteoarthritis. The studies above show modest pain reduction over months of daily use — not the kind of acute relief that NSAIDs provide within hours. Think of it as a potential addition to your toolkit, not the entire toolkit.

Frequently Asked Questions
How long does it take for hydrolyzed collagen to help knee pain?
Most participants showed measurable improvement between 6 and 12 weeks, with the strongest results at 13-24 weeks. Clark's study didn't show clear group separation until after 12 weeks. Plan for a minimum 3-month trial.
Is hydrolyzed collagen the same as type II collagen for joints?
No. Hydrolyzed collagen works by accumulating in cartilage to stimulate chondrocytes at doses around 10 grams daily. Undenatured type II collagen (UC-II) uses an immune mechanism at 40 mg daily. Different supplements, different evidence bases.
Are there risks or side effects from taking collagen peptides daily?
The 2023 meta-analysis of 507 patients found no significant increase in adverse events versus placebo. Minor gastrointestinal symptoms were the most common complaint. The FDA classifies collagen peptide as GRAS. People with source-animal allergies should choose products accordingly.
Does the collagen source — bovine vs. pork vs. marine — matter?
Kumar's study found pork and bovine collagen performed comparably. The processing method (hydrolysis conditions, molecular weight) likely matters more than animal origin. Marine collagen has less knee-specific clinical data.
Can collagen peptides rebuild knee cartilage or just reduce pain?
The three studies here measured pain, not structural changes. A 2024 trial by Devasia et al. found a 34.35% decrease in CTX-II (a cartilage degradation biomarker) with 10 grams versus 3.1% in placebo — suggesting collagen may slow breakdown. But no study has shown cartilage regrowth via imaging.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











