
For decades, the medical explanation for hot flashes went something like this: estrogen drops, your body overheats, and there's not much to do about it except replace the missing hormone. That explanation wasn't wrong, exactly, but it missed the wiring diagram underneath. Like blaming a car crash on a blown tire while ignoring the icy road and broken ABS.
A more complete picture came from a cluster of neurons most women have never heard of, buried in a region of the brain called the arcuate nucleus. These cells, known as KNDy neurons, produce three neuropeptides: kisspeptin, neurokinin B (NKB), and dynorphin. Research into how these neurons malfunction after menopause has rewritten our understanding of vasomotor symptoms and produced the first genuinely new class of hot flash medications in over two decades.
Most articles about "peptides for hot flashes" get the punchline wrong, though. Kisspeptin research revealed the mechanism. The treatment that emerged targets a different part of that mechanism entirely. Understanding why that distinction matters is the difference between following the science and chasing a misunderstanding.
The Brain's Broken Thermostat: How KNDy Neurons Drive Hot Flashes
Roughly 70% of women going through menopause experience vasomotor symptoms — hot flashes, night sweats, or both. For years, researchers assumed these were a straightforward consequence of falling estrogen levels. The hypothesis made intuitive sense but couldn't explain why some women with equally low estrogen never get a single hot flash, or why symptoms sometimes persist for a decade after menopause.
The missing piece turned out to be less about the hormone itself and more about a specific group of neurons that responds to it.
KNDy neurons sit in the hypothalamic arcuate nucleus (called the infundibular nucleus in humans), and they produce three neuropeptides simultaneously. Kisspeptin stimulates GnRH release, which drives reproductive hormone production. Neurokinin B acts as the accelerator, synchronizing the firing of neighboring KNDy neurons through NK3 receptors. Dynorphin acts as the brake, providing inhibitory control. Think of it as a three-pedal system: kisspeptin is the ignition, NKB is the gas, and dynorphin is the brake.
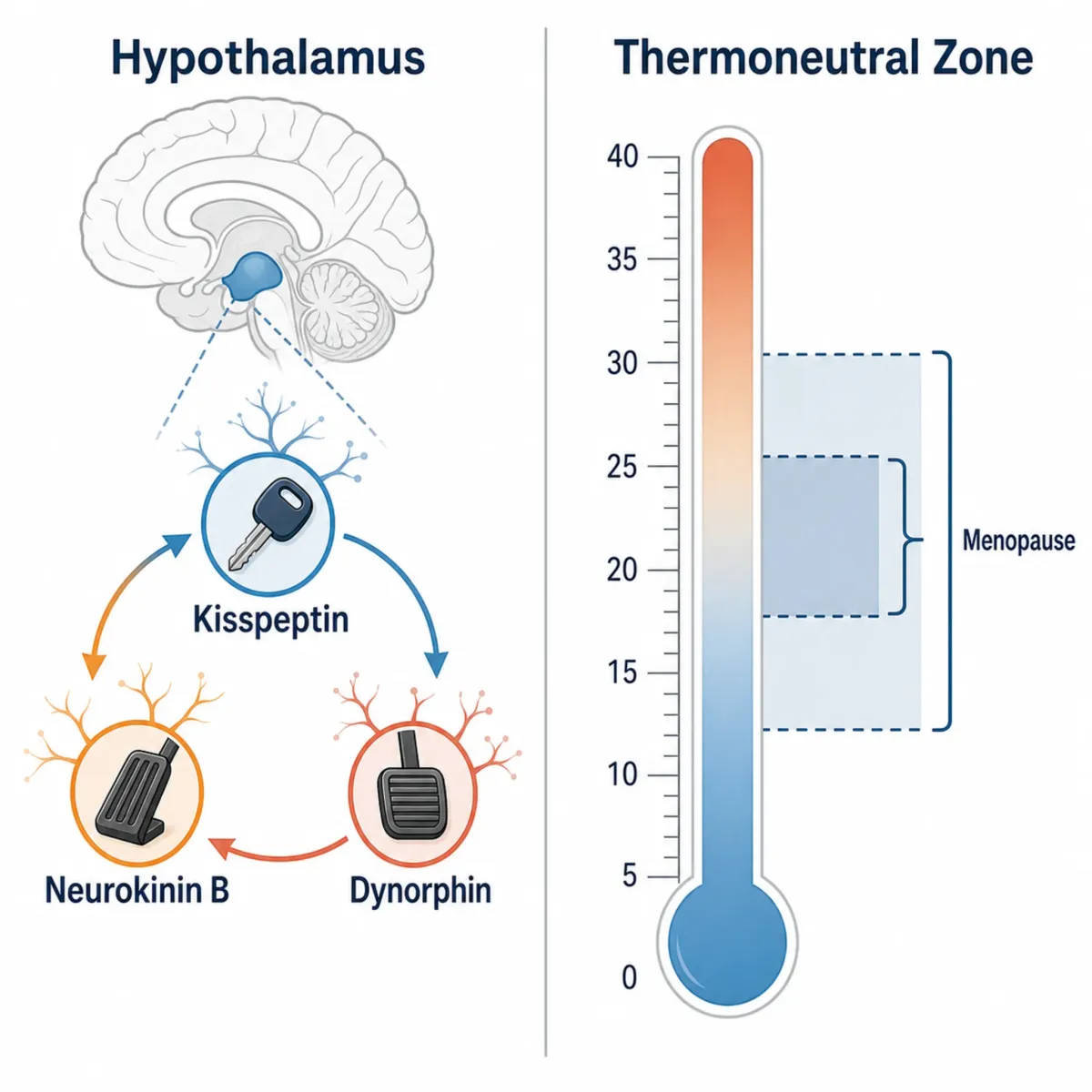
When estrogen is present at normal premenopausal levels, it keeps this system in check. The three neuropeptides maintain a balanced rhythm that coordinates both reproductive function and temperature regulation. These same neurons don't just control hormones — they project directly to the median preoptic nucleus (MnPO), the brain region that functions as the body's thermostat.
After menopause removes estrogen's restraining influence, these neurons physically change. Post-mortem studies of postmenopausal women have found that KNDy neurons become hypertrophied, with dramatically increased kisspeptin and neurokinin B gene expression. The gas pedal gets stuck down while the brake fades. Excess NKB floods into adjacent thermoregulatory areas, narrowing the thermoneutral zone — the temperature range your brain considers acceptable. A window that might normally span several degrees collapses to nearly nothing, meaning a tiny temperature fluctuation that wouldn't have registered before now triggers a full cooling emergency: blood vessels dilate, sweating kicks in, and you feel the unmistakable surge of a hot flash.
How Kisspeptin Research Cracked the Hot Flash Code
Kisspeptin's path to hot flash treatment took a circuitous route through melanoma research, of all places. It was first identified in 1996 as a metastasis suppressor gene product in melanoma research — nothing to do with reproduction, let alone menopause. Its role in the reproductive system only emerged in 2003, when two research groups independently discovered that inactivating mutations in KISS1R (the kisspeptin receptor, also called GPR54) cause hypogonadotropic hypogonadism and delayed puberty. That finding established kisspeptin as a master switch for puberty and reproductive function.
Subsequent work revealed that more than 90% of GnRH neurons express kisspeptin receptors. By 2005, kisspeptin was recognized as the most potent activator of GnRH neuron excitability ever identified.
The leap to hot flashes came from Dr. Naomi Rance at the University of Arizona, who showed that kisspeptin-producing neurons also produce neurokinin B and dynorphin. More critically, her lab demonstrated that these KNDy neurons project to thermoregulatory structures in the preoptic area — linking the reproductive control network directly to temperature management.
Clinicians had long noticed that hot flashes are closely timed with LH (luteinizing hormone) pulses, but LH doesn't cause vasodilation, and women without functional pituitary glands still get hot flashes. KNDy neurons explained the coincidence: the same cells driving LH pulses (via kisspeptin) simultaneously send NKB signals to the thermoregulatory center. The hot flash and the LH pulse share a neural origin without one causing the other.
Key distinction: Kisspeptin research revealed the pathway. But within that pathway, neurokinin B — not kisspeptin — is the neuropeptide that directly disrupts temperature regulation. This distinction is central to everything that followed in drug development.
From Lab Bench to Medicine Cabinet: NK3R Antagonists Take the Stage
Once NKB's role was clear, the therapeutic target followed: block NK3R to stop hot flashes without touching hormones. The first proof came in 2017 when MLE4901 showed a 73% reduction in hot flash frequency versus 28% for placebo in a trial led by Dr. Waljit Dhillo's group. Patients reported improvement within 48 hours. MLE4901 was shelved over liver toxicity concerns, but two drugs completed the pipeline.
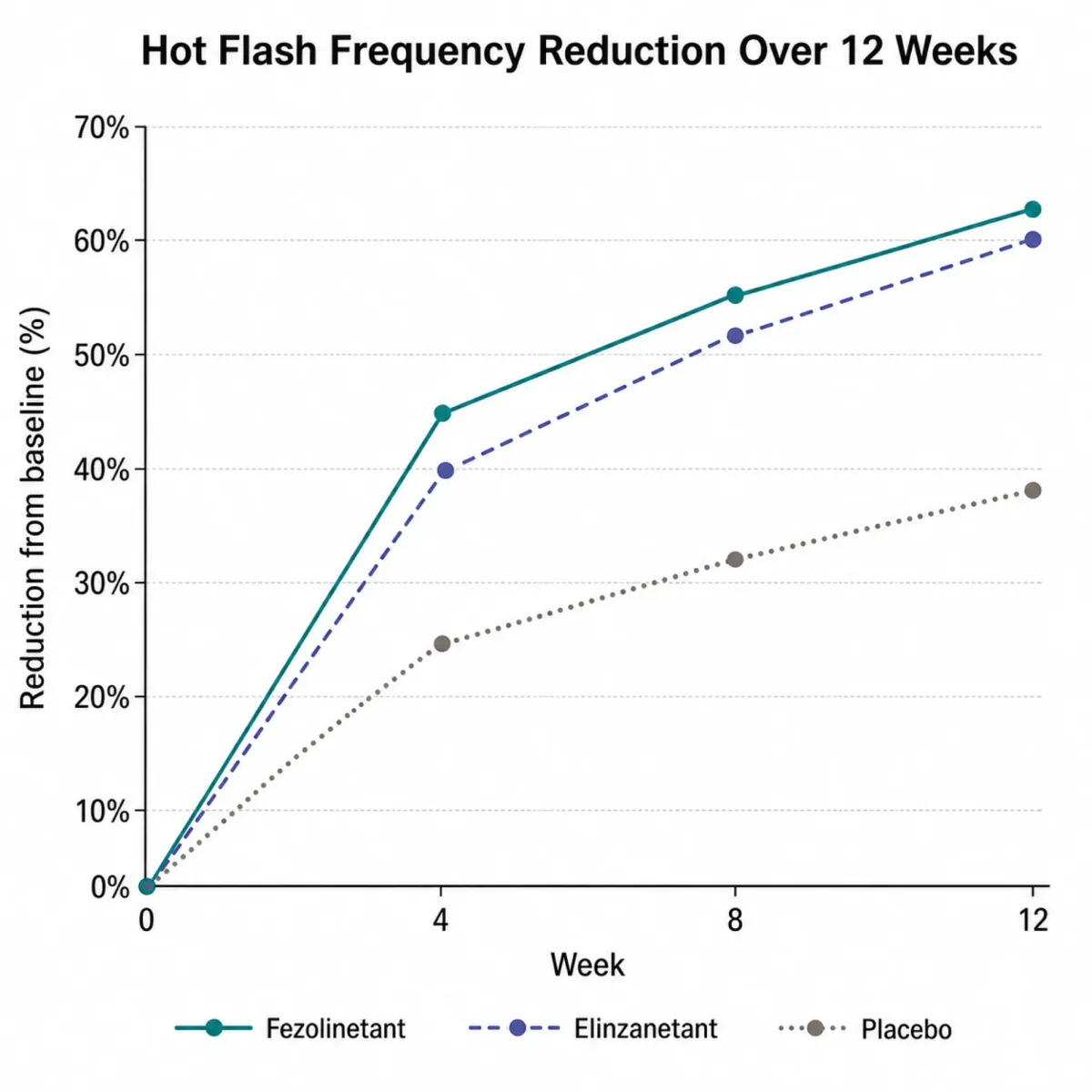
Fezolinetant (brand name Veozah) became the first FDA-approved NK3 receptor antagonist on May 13, 2023. Developed by Astellas Pharma, it's a selective NK3R blocker taken as a 45 mg tablet once daily. It crosses the blood-brain barrier to reach the hypothalamic thermoregulatory neurons directly. In the SKYLIGHT 2 trial, women taking 45 mg went from an average of nearly 12 moderate-to-severe hot flashes per day to about 4.5 at week 12 — a 64% reduction. The placebo group dropped from roughly 12 to about 7, a 45% reduction.
Elinzanetant (brand name Lynkuet), developed by Bayer, takes a different angle. It blocks both NK1 and NK3 receptors, which may explain its additional benefits for sleep. The FDA approved it in October 2024, making it the second drug in this class. At 120 mg daily, the OASIS-3 trial showed a 73.8% reduction in VMS frequency at week 12 versus 47.0% for placebo.

| Feature | Fezolinetant (Veozah) | Elinzanetant (Lynkuet) |
|---|---|---|
| FDA Approved | May 2023 | October 2024 |
| Mechanism | Selective NK3R antagonist | Dual NK1/NK3R antagonist |
| Daily Dose | 45 mg | 120 mg |
| VMS Reduction (Week 12) | ~64% (SKYLIGHT 2) | ~74% (OASIS-3) |
| Placebo Reduction | ~45% | ~47% |
| Sleep Benefits | Not primary endpoint | Significant (PROMIS −9.4 vs −5.7) |
| Liver Monitoring | Required at 3, 6, 9 months | Not required |
| Developer | Astellas Pharma | Bayer |
The Critical Distinction: Why Kisspeptin Itself Won't Cool You Down
Many peptide-focused articles get this part wrong. Because kisspeptin research led to the discovery of the KNDy pathway, and because NK3R antagonists emerged from that pathway, it's tempting to assume kisspeptin itself is a treatment for hot flashes. It is not — and giving someone exogenous kisspeptin could theoretically make things worse.
Kisspeptin is an activator. Administer it, and it stimulates GnRH neurons, triggering LH release. In clinical studies, exogenous kisspeptin increased LH secretion 2-3 fold in healthy volunteers. In women with hypothalamic amenorrhea, kisspeptin-54 at 6.4 nmol/kg produced a 10-fold LH increase. That's the opposite direction from hot flash relief. Since hot flashes are temporally linked to LH pulses through their shared KNDy origin, more kisspeptin could intensify the firing pattern that triggers temperature dysregulation.
The treatment works by blocking a different piece of the same machinery. Within the KNDy neuron, neurokinin B is the most direct driver of vasomotor symptoms. NKB signals through NK3 receptors on thermoregulatory neurons. Block that signal, and the overactive cooling response calms down while kisspeptin keeps doing its reproductive signaling job undisturbed.
Imagine a fire alarm system where one wire (kisspeptin) controls sprinkler pumps and another (NKB) controls the sirens. After menopause, both wires are over-activated. Injecting more current into the pump wire won't stop the sirens. You need to cut the siren wire (block NK3R). Kisspeptin research revealed the wiring diagram, which is why it gets the headlines, but the therapeutic action targets NKB.
Whether blocking kisspeptin's own receptor (KISS1R) would reduce hot flashes has never been tested in humans. A kisspeptin antagonist might dampen KNDy output broadly enough to affect temperature regulation, but it would also suppress reproductive hormone signaling with unpredictable consequences. NK3R antagonism avoids that problem by targeting only the thermoregulatory branch.
What the Clinical Trials Actually Show
Both approved NK3R antagonists have substantial phase 3 data. The headline reductions look impressive, but the gap between drug and placebo tells a more nuanced story.
In SKYLIGHT 2, women taking fezolinetant 45 mg started with an average of 11.79 moderate-to-severe hot flashes per day. At week 4, that number dropped to 5.67 — a 55% reduction. By week 12, it reached 4.49, a 64% reduction. These improvements held through week 52 of continued treatment. The placebo group also improved substantially, from 11.59 to 6.73 at week 12 (45% reduction), which speaks to both the strength of the placebo effect in hot flash research and the natural variability of symptoms.
Elinzanetant's OASIS program spanned three phase 3 trials across 184 sites in 15 countries. OASIS-1 (396 women) and OASIS-2 (400 women) showed VMS frequency dropping 55.9% and 57.9% at week 4 versus 31.4% and 35.7% for placebo, reaching 65.2% and 67.0% by week 12.
The OASIS-3 trial (JAMA Internal Medicine, September 2025), led by Dr. Nick Panay at Imperial College London, provided 52-week data: 73.8% reduction at week 12 versus 47.0% for placebo. The net drug effect beyond placebo was about 27 percentage points.
The Institute for Clinical and Economic Review (ICER) noted that fezolinetant's hot flash frequency reduction in the SKYLIGHT trials did not meet the minimum clinically important difference threshold of greater than 3.57 fewer hot flashes per day defined in earlier literature. The ICER panel voted 11-1 that the evidence was inadequate to demonstrate clear superiority over no pharmacologic treatment. That doesn't mean the drugs don't work — many patients report meaningful relief. But it does mean the gap between drug and placebo, while statistically significant, is more modest than the raw percentage numbers suggest.
What may tip the balance for elinzanetant is sleep. Its dual NK1/NK3 mechanism appears to address sleep disturbance directly, with PROMIS sleep scores improving by 9.4 points versus 5.7 for placebo in OASIS-3. Since night sweats and sleep disruption are often the most functionally debilitating aspects of menopausal vasomotor symptoms, that secondary benefit may matter as much as the hot flash count.
Where Peptide-Based Approaches Fit in the Post-HRT Landscape
Hormone replacement therapy remains the most effective treatment for hot flashes. No NK3R antagonist trial has shown better efficacy than estrogen. As Dr. Holly Thacker at the Cleveland Clinic has noted, "for the vast majority of women — especially if they start hormonal therapy under age 65 and within 10 years of menopause — there is significant benefit" from HRT.
NK3R antagonists fill a genuine gap for women who cannot or choose not to use hormones: breast cancer survivors on aromatase inhibitors, women with blood clot history, those who tried HRT and couldn't tolerate it. Before these drugs, the non-hormonal options were SSRIs, SNRIs, and gabapentin — all off-label, all inconsistent.
The comparative data between NK3R antagonists and the older non-hormonal options is telling. A systematic review found that NK3R antagonists reduced hot flash frequency by 62-93% from baseline, while SNRIs achieved 48-67%. The difference in severity was even starker: 41-94% severity reduction for NK3R antagonists versus 24-31% for SNRIs.
| Factor | NK3R Antagonists | SNRIs |
|---|---|---|
| VMS Frequency Reduction | 62-93% | 48-67% |
| VMS Severity Reduction | 41-94% | 24-31% |
| Onset of Effect | ~48 hours | Weeks (requires titration) |
| Discontinuation Due to AEs | 5-7% | 5-29% |
| Night Symptom Reduction | 63-81% | 53-77% |
| Most Common AE | Mild GI issues, fatigue | Nausea (often debilitating) |
Speed of onset also separates the two classes. The systematic review documented that NK3R antagonists produced symptom improvement after approximately 48 hours, with maximum effect by day 3. SNRIs require gradual dose titration over weeks, and nausea during that ramp-up period leads to discontinuation rates between 5-29%, especially during the first week.
Safety profiles differ. Fezolinetant requires liver function tests at 3, 6, and 9 months because 2.3% of patients developed elevated liver enzymes versus 0.9% on placebo, with one post-marketing case of cholestatic hepatitis with jaundice. Elinzanetant showed no hepatotoxic effects per an independent liver safety board.
By May 2024, roughly 28,700 patients had been prescribed fezolinetant in the U.S. Cost remains a barrier: ICER found a cost-effectiveness ratio of $390,000 per QALY at current pricing, far above standard thresholds.
What Researchers Are Working on Next
Researchers are investigating whether NK3R antagonists could treat polycystic ovary syndrome (PCOS), uterine fibroids, and endometriosis by modulating the same axis. If overactive NKB signaling disrupts temperature regulation in menopause, its role in other reproductive disorders with abnormal hormone pulsatility may be targetable too.
Kisspeptin itself is being explored for entirely different therapeutic applications. A trial of 32 women with low sexual desire found that kisspeptin modulated sexual brain processing, pointing toward potential use in hypoactive sexual desire disorder. That tracks biologically — kisspeptin sits at the top of the reproductive hormone cascade, and sexual desire has neuroendocrine components that kisspeptin may influence. Different application from hot flash treatment, though, and conflating the two misleads patients.
Could NK3R drugs work better combined with interventions targeting other parts of the KNDy circuit? Dynorphin, the inhibitory third of the triad, is reduced in postmenopausal women. Whether boosting dynorphin alongside NK3R blockade could produce additive benefits hasn't been tested. Three druggable targets, one addressed so far.
Fezolinetant is also in a phase 3 trial for hot flashes in women with breast cancer — a population locked out of HRT and with the greatest unmet need for non-hormonal options.
Frequently Asked Questions
Can I take kisspeptin peptide to treat hot flashes?
No. Kisspeptin activates GnRH neurons and stimulates reproductive hormone release — the opposite of what hot flash relief requires. The approved drugs (fezolinetant and elinzanetant) block neurokinin B signaling through NK3 receptors, a different branch of the same pathway. Kisspeptin research revealed the mechanism; the treatment targets NKB.
How quickly do NK3R antagonists work compared to other hot flash treatments?
Much faster. Clinical data shows improvement within about 48 hours, with maximum effect by day 3. SSRIs and SNRIs require weeks of dose titration. HRT typically takes 2-4 weeks.
What is the difference between fezolinetant and elinzanetant?
Fezolinetant (Veozah) blocks only the NK3 receptor and is taken at 45 mg daily. Elinzanetant (Lynkuet) blocks both NK1 and NK3 receptors at 120 mg daily. The dual mechanism may explain elinzanetant's additional benefits for sleep disturbance. Fezolinetant requires liver function monitoring at 3, 6, and 9 months; elinzanetant's trials showed no hepatotoxicity signals. Both are non-hormonal and taken orally once daily.
Are these drugs safe for breast cancer survivors?
Neither involves estrogen or any hormonal mechanism. A phase 3 trial is evaluating fezolinetant specifically in breast cancer patients with hot flashes. Both drugs showed no endometrial effects in long-term studies. Involve your oncologist in any treatment decision, particularly around drug interactions.
Do NK3R antagonists replace HRT?
Not for women who can safely take hormones. HRT remains more effective and provides additional bone, cardiovascular, and genitourinary benefits that NK3R antagonists don't address. These drugs fill a gap for women who cannot or choose not to use hormones, outperforming previous non-hormonal options (SNRIs, gabapentin) in both efficacy and tolerability.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











