
The FDA's New 3-Category Peptide Framework Explained
On a Tuesday in September 2023, the FDA quietly published an updated interim policy for its 503A Bulks List that reshuffled the legal rules for peptide therapies. Seventeen peptide bulk drug substances, including BPC-157, TB-500, epitalon, and MOTs-C, landed in a new classification bucket that effectively cut off their supply through standard compounding pharmacies.
The framework works like a traffic light, except the yellow light might be the most important one.
Category 1 means "go, with caution." The FDA has evaluated the substance and has not identified significant safety risks. Under the interim enforcement discretion policy, licensed 503A compounding pharmacies can use these bulk drug substances to prepare patient-specific formulations, provided they meet all other requirements of Section 503A of the FD&C Act: a valid prescription, an individually identified patient, and no "essentially copying" a commercially available drug.
Category 2 means "stop." The FDA has determined these substances "may present significant safety risks" in compounding. Standard 503A pharmacies cannot lawfully compound with them. Category 2 is what most people refer to when they say peptides were "banned," though that word oversimplifies what happened.
Category 3 means the FDA received a nomination but the supporting information was inadequate. The substance sits in a holding pattern, neither approved nor flagged for safety. Think of it as the DMV losing your paperwork: nothing has been decided because nothing has been reviewed.
Key distinction: Category 2 does not make a peptide illegal to possess. It restricts compounding pharmacies from using that bulk drug substance in patient medications. You would not face criminal charges for having BPC-157 in your medicine cabinet. But your doctor could not lawfully write you a prescription filled at a standard compounding pharmacy while the substance sat on the Category 2 list.
Category 1: FDA-Approved Peptides You Can Get With a Prescription
Category 1 is the shortest and most straightforward lane. These are bulk drug substances the FDA has evaluated and found no significant safety concerns for compounding purposes. A licensed prescriber can write a prescription, a 503A pharmacy can compound the formulation, and the patient picks it up. No special workarounds needed.
The catch: very few peptides currently sit in Category 1. The most notable example was GHK-Cu for non-injectable routes (topical creams, serums). But even that was removed from Category 1 in the April 2026 update because the nominator withdrew the nomination. It is now slated for PCAC review before the end of February 2027.
Meanwhile, several peptides that have full FDA drug approval are a different story entirely. Semaglutide (Ozempic/Wegovy), tirzepatide (Mounjaro/Zepbound), liraglutide (Saxenda/Victoza), and bremelanotide (Vyleesi) are approved drugs with their own NDAs. They exist outside the 503A compounding framework altogether.
The compounding question for these FDA-approved peptides comes down to drug shortages. When a drug is on FDA's Drug Shortages List, compounding pharmacies may prepare versions of it. When the shortage ends, compounding must stop within a defined enforcement discretion window. The FDA resolved the semaglutide shortage on February 21, 2025, and the tirzepatide shortage on December 19, 2024. Enforcement discretion for compounded semaglutide under 503A ended April 22, 2025; under 503B, May 22, 2025.
If you are currently using compounded semaglutide or tirzepatide from a 503A pharmacy, you should know that the legal basis for that compounding has expired. The FDA has explicitly stated that tirzepatide and semaglutide do not currently appear on the 503B bulks list or on FDA's drug shortage list.
Category 2: The Peptides FDA Pulled From Compounding (and Why)
As of the April 22, 2026 update, 14 substances remain on the active Category 2 list. Several of these are peptides that the biohacking community uses regularly, and understanding why the FDA flagged each one reveals how the agency weighs risk when clinical data is sparse.
| Substance | Date Added | FDA's Stated Safety Concern |
|---|---|---|
| GHRP-2 (injectable/nasal) | Sep 2023 | Immunogenicity risk, unnatural amino acid complexity, adverse events including death in critically ill subjects |
| GHRP-6 | Sep 2023 | Immunogenicity risk, potential cortisol effects, insulin sensitivity decrease |
| Ibutamoren mesylate (MK-677) | Dec 2022 / Sep 2023 | Congestive heart failure signal in a hip fracture RCT terminated early |
| Ipamorelin acetate | Sep 2023 | Immunogenicity risk, serious adverse events including death when administered IV for gastric motility |
| Kisspeptin-10 | Sep 2023 | Immunogenicity risk, no or only limited safety data for proposed routes |
The remaining active Category 2 entries are non-peptide compounds: cesium chloride (cardiac toxicity, flagged since 2018), chloral hydrate (oversedation and death risk, especially pediatric), domperidone (cardiac arrhythmias), and several others with long-established safety profiles that predated the peptide crackdown.
A pattern emerges when you read the FDA's reasoning across the peptide entries: the word "immunogenicity" appears in nearly every one. The agency's central argument is that compounded injectable peptides, produced without the quality controls of an approved manufacturing process, carry a heightened risk of aggregation and peptide-related impurities that could trigger immune reactions. This is less about the peptide molecule itself and more about the compounding process.

Category 3 and the Gray Area: Peptides That Just Left the "Banned" List
Here is where the April 2026 announcement matters most, and where the coverage has been most misleading.
On April 15, 2026, the FDA announced it would remove 12 peptide bulk drug substances from Category 2 within seven calendar days. The stated reason: their nominations had been withdrawn by the nominators. The peptides removed were:
BPC-157, cathelicidin LL-37, dihexa acetate, emideltide (DSIP), epitalon, GHK-Cu (injectable routes), KPV, mechano growth factor pegylated (PEG-MGF), melanotan II, MOTs-C, semax, and thymosin beta-4 fragment/TB-500.
Social media lit up. "11 peptides just got UNBANNED by the FDA" was a typical headline. But as healthcare attorneys at both Frier Levitt and Orrick quickly pointed out, this interpretation is wrong in a way that could cost people money and expose pharmacies to regulatory risk.
What actually changed: These peptides moved from the "no" list to the "maybe" list. Removal from Category 2 does not place a substance on the 503A bulks list. It does not grant Category 1 enforcement discretion. It does not authorize any pharmacy to compound with these substances. As Frier Levitt attorneys wrote: "Removal from Category 2 does not render these bulk drug substances eligible for compounding under section 503A."
The peptides now exist in a regulatory no-man's-land. They are no longer flagged as presenting significant safety risks, but they are not approved for compounding either. Think of it like being released from prison but not having your record expunged: the charges are dropped, but you still cannot vote.
This context matters because it followed weeks of public signaling from HHS Secretary Robert F. Kennedy Jr. On February 27, 2026, appearing on The Joe Rogan Experience, Secretary Kennedy stated he expected the FDA to announce action "within a couple of weeks." He described himself as a "big fan" of peptides, said he had used them personally "with really good effect on a couple of injuries," and asserted that the prior administration had "illegally" placed 19 peptides into Category 2 in 2023.
Kennedy also pointed to the gray market dangers: consumers "have no idea" whether unregulated products are legitimate. His framing positioned the regulatory shift as both a safety play and a market correction, channeling demand away from unregulated sellers and toward "ethical suppliers" operating through FDA-inspected channels.
Legal Buying Channels: Telehealth, Compounding Pharmacies, and the Research Chemical Crackdown
Three buying channels exist right now for peptides, and the FDA is actively working to collapse one of them.
Channel 1: Compounding Pharmacies (503A and 503B)
This is the regulated route. Under Section 503A of the FD&C Act, a state-licensed pharmacy can compound a drug for an individual patient based on a valid prescription. The pharmacy cannot regularly make "essentially copies" of commercially available drugs, and must source pharmaceutical-grade API from FDA-registered facilities operating under current Good Manufacturing Practice (cGMP) standards.
Section 503B outsourcing facilities operate under a different set of rules: they can compound without individual prescriptions but are restricted to bulk drug substances on the 503B bulks list or drugs currently on the FDA shortage list.
The practical problem with this channel, even for peptides that eventually clear the PCAC: pharmaceutical-grade API for many of these peptides does not yet exist at commercial scale. Most available supply is research-grade, which cannot lawfully be used in compounded drugs for patients. API manufacturers are positioning to meet demand, but supply chain readiness will likely be the bottleneck after regulatory approval.
Channel 2: Telehealth Clinics With Specialty Compounding Networks
A small network of specialty clinics and telehealth platforms have maintained access to certain peptides throughout the Category 2 era by working within specific compliance pathways. These operations pair licensed prescribers with 503A pharmacies that compound under narrow exemptions.
If the PCAC recommends inclusion on the 503A bulks list and the FDA follows through, this channel widens dramatically. As the Frier Levitt analysis notes, any licensed provider would then be able to prescribe these substances consistent with state law, and any compliant 503A pharmacy could compound them.
Channel 3: "Research Chemical" Sellers (Under Active FDA Attack)
This is the channel the FDA is dismantling. On April 7, 2026, the FDA published seven warning letters targeting research peptide sellers: Gram Peptides, Prime Sciences, Lovega, FormPour, Guangzhou Huli Technology, Mile High Compounds, and PekCura Labs. The products targeted included retatrutide, tirzepatide, semaglutide, and other GLP-1 agonists.
The legal argument in each letter was identical: a company sells unapproved peptides with a "research use only" or "not for human consumption" disclaimer, then pairs the product with bacteriostatic water for injection. The FDA reads the bacteriostatic water pairing as dispositive evidence of intended human use, declares the disclaimer a sham, and treats both items as unapproved drugs under Section 505(a) of the FD&C Act.
This is not theoretical enforcement. The bacteriostatic-water trigger gives the FDA a clean, repeatable enforcement template. If you are buying peptides from a website that sells them alongside reconstitution supplies, the legal risk to that supplier has increased substantially in 2026.
| Buying Channel | Legal Status (May 2026) | Quality Assurance | Typical Cost |
|---|---|---|---|
| 503A Compounding Pharmacy | Legal for Cat 1 substances with prescription | FDA-registered API, cGMP, state board oversight | $150-400/month |
| Telehealth + Specialty Compounding | Legal (same 503A framework) | Same as above + prescriber oversight | $200-600/month (includes consult) |
| Research Chemical Websites | Legal gray area, active FDA enforcement | None guaranteed; research-grade, no COA standard | $30-150/month |
The 2026 Enforcement Timeline: Key Dates Every Buyer Should Know
The regulatory picture for peptides will shift more in the next 12 months than it has in the previous decade. Here is the timeline, stripped of speculation.
| Date | Event | What It Means |
|---|---|---|
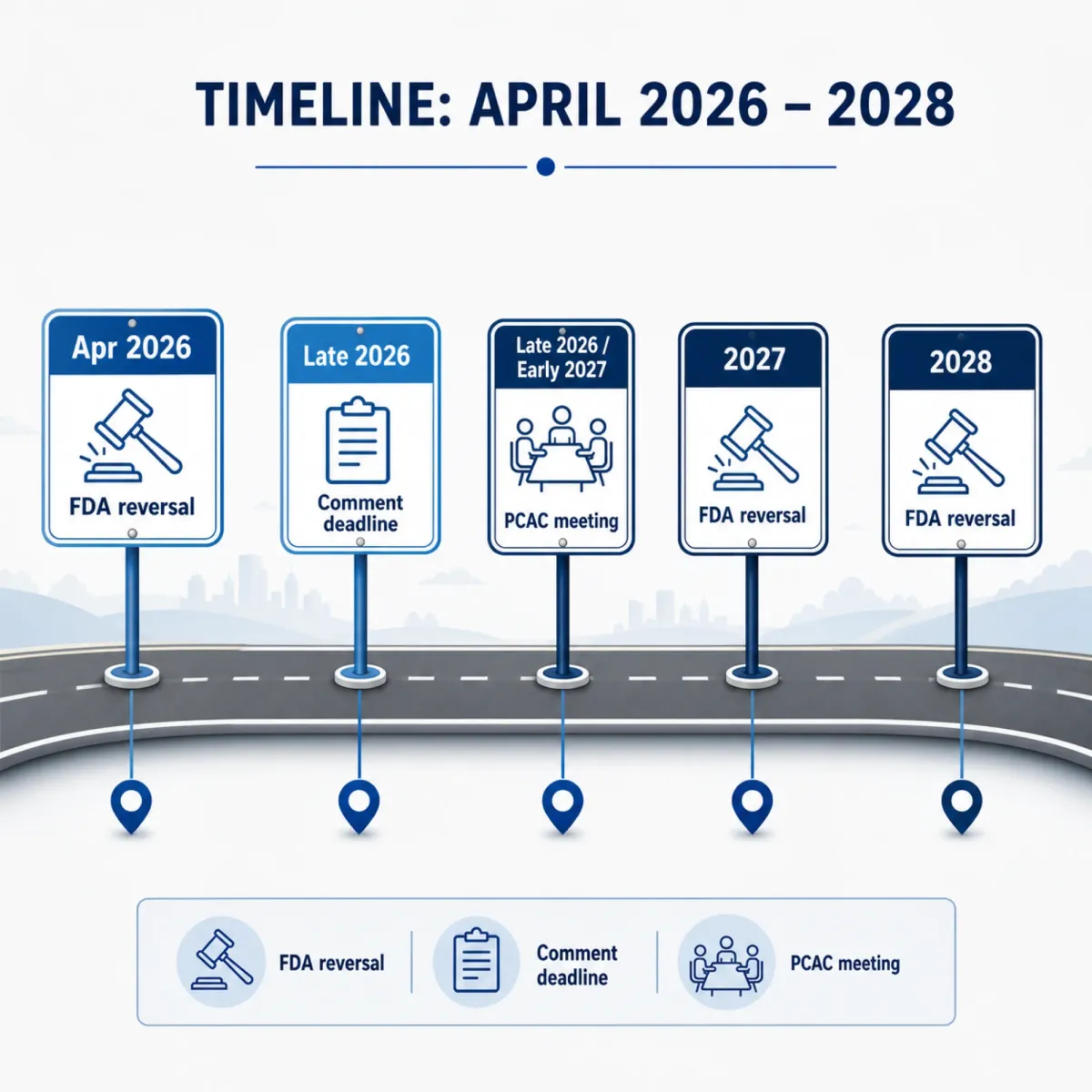
| April 15, 2026 | FDA publishes Federal Register notice (Doc 2026-07361) and updated interim 503A Bulks List | 12 peptides announced for removal from Category 2; PCAC meetings scheduled |
| ~April 22, 2026 | 12 peptides formally removed from Category 2 | No longer designated as "significant safety risk," but NOT approved for compounding |
| June 30, 2026 | Deadline for oral presentation requests to PCAC | Researchers, clinicians, or patients who want to speak at the hearing must file by this date |
| July 9, 2026 | Priority deadline for written public comments (Docket FDA-2025-N-6895) | Comments submitted by this date are provided directly to the PCAC committee for review |
| July 23-24, 2026 | PCAC reviews 7 peptides: BPC-157, KPV, TB-500, MOTs-C (July 23); DSIP, Semax, Epitalon (July 24) | Advisory committee votes on whether to recommend inclusion on 503A bulks list |
| Before Feb 2027 | PCAC reviews remaining 5: LL-37, dihexa, GHK-Cu (injectable), PEG-MGF, melanotan II | Second batch of Category 2 removals evaluated |
| 2027-2028 (est.) | Proposed rule → final rule for any PCAC-recommended peptides | Formal rulemaking typically takes 2-3 years after PCAC recommendation |
The PCAC currently has only four members. Several were removed and have not been replaced, raising quorum concerns. This is a procedural detail that could delay the July meeting, though given the administration's public commitment, most regulatory attorneys expect the vacancies to be filled before summer.
There is also a precedent problem. Under the previous administration, the PCAC voted against inclusion of all peptides that were brought before it, finding unacceptable safety risks in each case. However, as Orrick attorneys note, "the current environment is materially different: many prior FDA staff have departed, the PCAC has significant vacancies that Secretary Kennedy could fill before the July meeting, and the administration has publicly signaled support for broader peptide access."
The practical question for buyers comes down to what happens between the PCAC vote and the final rule. If the PCAC recommends inclusion and the FDA extends enforcement discretion (moving these peptides into Category 1 during the rulemaking process), compounding pharmacies could resume dispensing relatively quickly. If the FDA declines to extend enforcement discretion, the formal rulemaking process could stretch into 2028 or beyond.
Frequently Asked Questions
Can I legally buy BPC-157 right now in the United States?
BPC-157 was removed from the FDA's Category 2 list on approximately April 22, 2026, meaning it is no longer classified as presenting "significant safety risks." However, it has not been added to the 503A bulks list and is not under Category 1 enforcement discretion. A specialty clinic operating through narrow compliance pathways may still offer it, but standard compounding pharmacies cannot yet compound it as a matter of routine. The PCAC will review BPC-157 at its July 23, 2026 meeting.
Are peptides illegal to possess?
Peptides are not controlled substances under federal law (with rare exceptions like growth hormone, which is regulated under the Anabolic Steroids Control Act). The FDA's category system governs what compounding pharmacies can make, not what individuals can possess. However, selling unapproved peptides for human use is unlawful under the FD&C Act, which is why the FDA has issued warning letters to research chemical sellers.
What is the difference between 503A and 503B pharmacies?
A 503A pharmacy compounds individual prescriptions for specific patients based on a doctor's order. A 503B outsourcing facility can compound drugs without patient-specific prescriptions, often in larger batches, but is restricted to substances on the 503B bulks list or the FDA drug shortage list. 503B facilities are FDA-inspected; 503A pharmacies are state-regulated. Both must use pharmaceutical-grade API from FDA-registered manufacturers.
How can I submit a public comment on the peptide PCAC review?
Written comments can be submitted to Docket FDA-2025-N-6895 at regulations.gov. Comments submitted by July 9, 2026 are prioritized for inclusion in the PCAC's meeting materials. Requests to make oral presentations at the July 23-24 meeting must be filed by June 30, 2026.
Will compounded semaglutide come back?
The FDA resolved the semaglutide shortage on February 21, 2025, and enforcement discretion for compounders has expired. Unless semaglutide goes back on the drug shortage list, compounding pharmacies cannot lawfully produce it. Semaglutide and tirzepatide do not appear on the 503B bulks list. A separate FDA proposal to explicitly exclude them from the 503B list was published in May 2026.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











