
Why Postpartum Recovery Takes Longer Than Anyone Tells You
Your six-week postpartum checkup feels like a finish line. Clear it, get told everything looks fine, go back to life. But the tissues that built and delivered a baby work on a different clock, and there's a wide gap between "no acute complications" and "actually healed."
During vaginal delivery, pelvic floor muscles stretch to 250% of their resting length. Pull a rubber band to two and a half times its natural size, then expect it to snap back in six weeks. Pelvic floor recovery isn't maximized until four to six months postpartum, yet most women get activity clearance well before that.
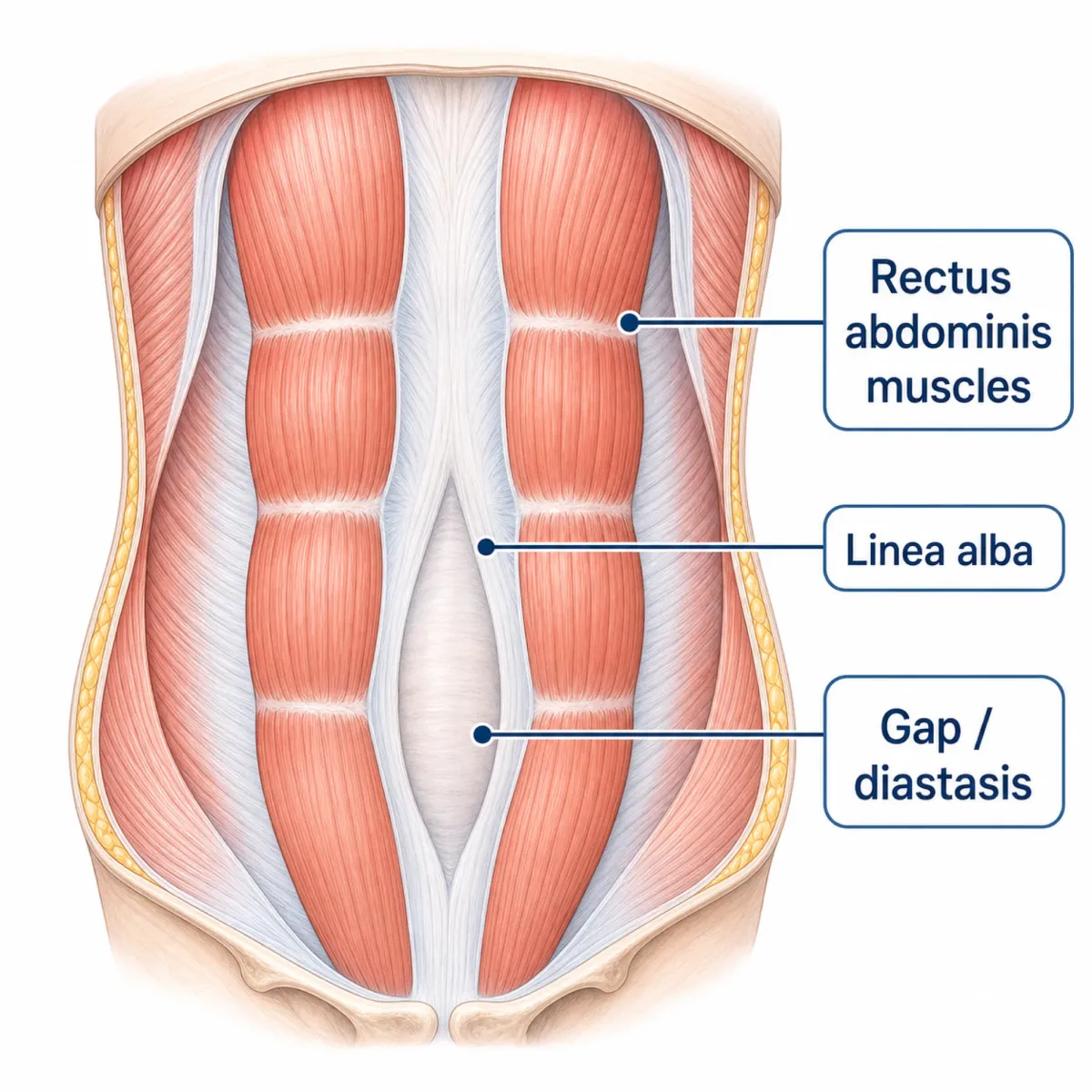
The abdominal wall follows a similar arc. By 38 weeks, abdominal musculature has stretched to 115% of its resting length. The connective tissue down the center of your abdomen (the linea alba) separates to make room, creating diastasis recti abdominis. A scoping review found that DRA affects 66-100% of women in the final trimester and persists in up to 53% within 24 hours of delivery. At twelve months, 36% still have measurable separation.
For the roughly 32% of women who deliver by cesarean section, surgical healing stacks on top of pregnancy recovery. Uterine scar tissue continues remodeling at six weeks postpartum, and sensory nerve recovery at the incision site takes approximately one year, with superficial nerves regenerating at roughly 1mm per day.
Across all delivery types, more than one in four women experience at least one pelvic floor dysfunction condition. Those still symptomatic at three months show significantly higher odds of problems persisting at five years. These aren't complications from unusual births. They're normal recovery from normal ones.
Six-week clearance means your OB doesn't see acute complications. It does not mean connective tissue, pelvic floor, or surgical sites have finished healing. The actual recovery window runs four to six months minimum, with some tissues remodeling for a full year.
Collagen Peptides for Connective Tissue Repair
Collagen peptides have the fewest question marks of any peptide category for postpartum women. Food-derived, broken down during digestion into amino acids your body already uses, and carrying the closest thing to a safety consensus you'll find for breastfeeding mothers.
The InfantRisk Center, a clinical resource for medication safety in lactation, notes that collagen is generally considered safe during breastfeeding because it breaks down into amino acids and small peptides during digestion, with minimal impact on breast milk. Their cited research indicates that moderate changes in protein intake do not significantly affect milk protein content. Your body doesn't pass intact collagen molecules into breast milk. It dismantles them and uses the parts.
That matters because collagen is the structural protein holding your abdominal wall together. As one DRA nutrition resource explains, collagen is what binds together at the front of your abdomen, and without adequate regeneration the gap can't close. Think of collagen as bricks and exercise as the mason. You need both, but adding extra bricks during a rebuild makes sense.
Protein targets for postpartum recovery land around 70-100 grams daily, with collagen counting toward that total. Bone broth is the best food source for rebuilding collagen, containing gelatin, glucosamine sulfate, chondroitin, and hyaluronic acid. Collagen peptide powders offer a concentrated alternative for postpartum women who can barely finish a meal, let alone simmer stock for hours.
| Collagen Source | Key Benefits | Breastfeeding Safety |
|---|---|---|
| Bone broth | Contains gelatin, glucosamine, chondroitin, hyaluronic acid | Safe — whole food |
| Bovine collagen peptides (Type I & III) | Supports skin, connective tissue, linea alba repair | Generally safe — breaks down to amino acids |
| Marine collagen peptides | Higher glycine content (~33%), gut barrier support | Generally safe — check for shellfish allergies |
| Plant-based approach (vitamin C + protein) | Supports endogenous collagen synthesis | Safe — food-derived nutrients |
One caveat: supplements lack FDA regulation for purity. The InfantRisk Center recommends choosing brands with third-party testing and checking ingredients for allergens, especially fish or bovine sources.
BPC-157 and Tissue Healing: The Promise and the Safety Gap
BPC-157 appears in nearly every "postpartum peptide protocol" circulating online. The animal research explains the enthusiasm. This synthetic peptide, derived from a compound in gastric juice, has produced striking wound healing results in rodent studies. The problem is translating those results to a breastfeeding mother.
A review in Frontiers in Pharmacology documented that BPC-157 cream at 1 μg/g accelerated healing of deep partial-thickness burns covering 20% of body surface area, with increased breaking strength and reduced edema. The same review found BPC-157 stimulated earlier collagen maturation and produced more organized collagen than PDGF-BB (a clinical standard growth factor) by day 12.
The muscle data gets peptide clinics excited about postpartum use. In rats with transected quadriceps muscles, BPC-157 produced functional connection and near-normal appearance by day 72. It upregulates tissue repair genes, including VEGF and Akt1, within two to five minutes of application. The lethal dose threshold (LD1) was never reached in available studies.
The gap between rat tissue repair and postpartum human use, though, is wide open. No bridge exists yet.
| What We Know (Animal Data) | What We Don't Know (Human Data Gap) |
|---|---|
| Accelerates burn, muscle, and tendon healing in rodents | No human wound healing clinical trials completed |
| LD1 not achieved in toxicity studies | No safety data in pregnant or breastfeeding women |
| Upregulates collagen maturation and angiogenesis | Unknown transfer into breast milk |
| Previously used in UC/MS trials without adverse effects | A 2015 Phase I human trial was registered but results never published |
| Consistent dosing across multiple injury models in rats | No validated human dosing protocol exists |
Multiple clinical sources are unambiguous on this point. Inovi Fertility explicitly states to avoid BPC-157 during pregnancy or breastfeeding unless controlled human data show safety. American Wellness Pharmacy echoes that pregnant or breastfeeding individuals should not use BPC-157 or related peptide preparations. Human clinical data are, in the words of one fertility clinic's assessment, "virtually nonexistent."
A Phase I human trial was registered in 2015 to study BPC-157 safety and pharmacokinetics, but published results are "conspicuously missing." That gap — between registering a trial and publishing nothing — should give anyone pause, especially new mothers weighing risk against recovery speed.

Glycine for Postpartum Sleep and Mood
Sleep deprivation is the universal postpartum experience. It drags down mood, healing speed, hormonal recovery, milk production. Glycine won't give you eight uninterrupted hours, but the data suggests it can make whatever sleep windows you get more restorative.
Glycine is the simplest amino acid, already present in your body and your diet. Its sleep mechanism is surprisingly specific: it acts through NMDA receptors in the suprachiasmatic nucleus, your brain's master clock, and ablating this structure completely abolishes glycine's sleep effects. What that looks like in practice: glycine drops your core body temperature by shunting blood toward your extremities. Thermal imaging shows increased hand and foot skin temperature within 30 minutes of a dose. Your body cools itself to initiate sleep naturally; glycine speeds that up.
The standard dose in human trials is 3 grams, one hour before bed. A crossover trial with sleep-restricted adults found glycine reduced NREM sleep latency from 54.67 to 36.79 minutes, roughly 18 minutes faster to restorative sleep. A second study showed 3g significantly decreased next-day reaction time (p=0.003) and reduced fatigue (p=0.022), with fatigue improvement peaking in early afternoon. A systematic review confirmed that 3 grams per day improved sleep quality, alertness, and cognition while decreasing fatigue across multiple small trials.
| Glycine Sleep Data | Finding | Source |
|---|---|---|
| Dose | 3 grams, 1 hour before bedtime | Multiple trials |
| Sleep latency reduction | ~18 minutes faster to reach NREM sleep | PMC4397399 |
| Next-day reaction time | Significantly improved (p=0.003) | PMC3328957 |
| Next-day fatigue | Significantly reduced (p=0.022) | PMC3328957 |
| Mechanism | Core temperature reduction via peripheral vasodilation | PMC4397399 |
| Safety | <5% mild digestive upset; no serious adverse events | Multiple reviews |
Safety is where glycine separates from injectable peptide options. Fewer than 5% of study participants had any side effects, limited to minor digestive upset. No dependency, tolerance, or rebound insomnia documented. It preserves normal sleep architecture instead of forcing sedation.
A caveat worth noting: a systematic review found that glycine sleep studies had small sample sizes with high risk of bias, and only 2 of 21 parallel-group RCTs were at low risk of bias. The results are consistent and the mechanism is well-characterized, but the evidence base is thinner than the headlines suggest. Still, glycine's status as a naturally occurring amino acid in common foods places it in a different risk category entirely from injectable research peptides.
The Practical Recovery Timeline (Weeks 0-6, 6-12, 12-24)
Your body's healing phases dictate what it can use and when. Flooding a system with growth-signaling compounds during the inflammatory phase doesn't accelerate recovery. It's fertilizer on unprepared soil.
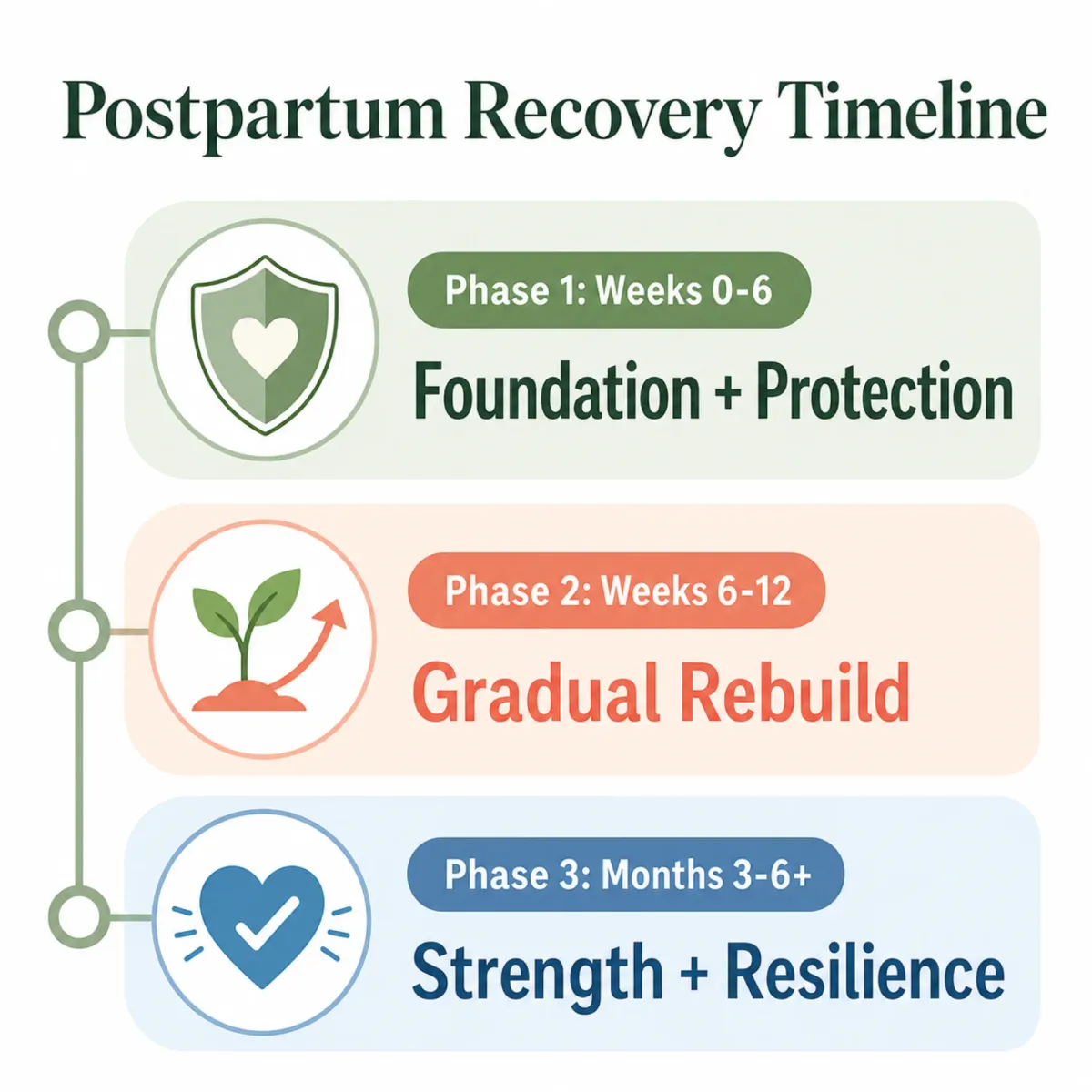
Weeks 0-6: Protect and Nourish
This is the acute healing window. Research-based rehabilitation guidelines recommend minimizing musculoskeletal stress during weeks 0-2 with only household ambulation, then progressing to walking under 15 minutes during weeks 3-4. For C-section recovery, weeks 0-6 should focus on gentle breathing, light mobility, and short walks — skipping diastasis-specific drills entirely.
Peptide focus here should be food-based: adequate protein (70-100 grams daily), collagen through bone broth or peptide powder if tolerated, glycine if sleep fragmentation is severe. Your body is running its own inflammatory-to-repair cascade. Supply building materials; don't interfere.
Weeks 6-12: Rebuild
The six-week mark is where most DRA rehabilitation programs begin structured intervention. Transversus abdominis exercises produce significant inter-recti distance reduction after 12 weeks compared to controls. Walking increases to 30 minutes by weeks 5-6, with short jogging bouts under 60 seconds beginning at week 8 — but only after completing 30-minute asymptomatic walking.
Collagen supplementation during this phase supports connective tissue under active remodeling. Fascia needs approximately 12 weeks for baseline tensile strength, so this window is when your body is most actively laying down new collagen. For C-section recovery, add consistent scar massage 2-4 times weekly for at least 2 minutes to loosen adhesions.
Weeks 12-24: Strengthen and Assess
DRA natural resolution plateaus after the initial 8-week postpartum period, so active rehabilitation becomes more important, not less. This is the phase for targeted eccentric abdominal work, hypopressive training with breath holds, and gradual return to higher-impact activity. Clinical guidelines recommend a minimum of 6 months of conservative treatment before considering surgery for persistent DRA.
Collagen can continue if desired. Glycine remains safe for ongoing sleep support. Whether to explore anything beyond food-derived peptides becomes a conversation with your OB, armed with the reality that injectables still lack postpartum safety data.
What Postpartum Peptide Clinics Won't Tell You
Peptide clinics marketing "postpartum recovery protocols" have multiplied recently, offering BPC-157, thymosin beta-4, and growth hormone secretagogues with claims about accelerated healing and body composition. Some of the ingredient data, from animal research, looks promising. But the framing hides things that matter when the patient is a new mother.
No validated human dosing protocol exists for BPC-157. Rodent doses don't scale to humans because metabolic rates and clearance mechanisms differ across species. Clinics dose based on extrapolation and anecdote, not pharmacokinetic data.
Quality control from unregulated peptide sources is a real concern. BPC-157 has no FDA approval for any indication. Compounding pharmacies operate under different standards than pharmaceutical manufacturers, and direct-to-consumer peptide vendors operate under almost none. What's in the vial may not match the label.
And none of these protocols have been tested in postpartum women. The animal models used healthy male rats. The human trials studied adults with ulcers or MS. No human clinical trial data exists for BPC-157 wound healing, let alone for lactating postpartum women.
Collagen peptides and glycine come from food, have established safety profiles, and offer real (if modest) support for tissue healing and sleep. Injectable peptides like BPC-157 carry genuine promise in animal data but zero safety evidence for postpartum women. Any provider who glosses over that gap deserves skepticism.
If postpartum hair loss is a concern alongside tissue recovery, we've covered the peptide angle on that separately. The same safety framing applies.
Frequently Asked Questions
Are collagen peptides safe while breastfeeding?
Yes. The InfantRisk Center considers collagen generally safe during breastfeeding because it breaks down into amino acids during digestion, with minimal impact on breast milk. Choose third-party tested products and start with a lower dose. You're supplementing the same amino acids found in bone broth and meat.
Can I take BPC-157 for C-section recovery?
The animal data is impressive, but pregnant or breastfeeding individuals are explicitly advised against BPC-157 by multiple clinical sources. No human wound healing trials are complete, no validated dosing exists, and breast milk transfer is unknown. After weaning, discuss the evidence gaps with your OB rather than relying on clinic marketing.
How much collagen should I take postpartum?
No postpartum-specific dosing study exists. General protein targets are 70-100 grams daily from all sources. Most collagen supplements deliver 10-20 grams per serving. Pair with whole food protein and adequate vitamin C, which your body needs to synthesize new collagen from the amino acids.
Does glycine actually help with postpartum sleep?
Small but consistent trials show 3 grams of glycine before bedtime reduces time to restorative sleep by roughly 18 minutes and improves next-day alertness. The evidence base is limited to small studies, but the safety profile is strong and the mechanism well-understood. It won't replace lost sleep hours, but it can improve the quality of the ones you get.
When should I start a peptide protocol after giving birth?
Food-derived peptides (collagen, glycine) are fine as soon as you're eating normally postpartum. For injectable peptides or synthetic compounds, no evidence-based protocol exists for postpartum women. Clinical guidelines recommend a minimum of 6 months of conservative treatment (exercise, nutrition, pelvic floor therapy) before considering interventional approaches for persistent DRA.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











