
Which Peptides Insurance Actually Covers (and Which It Never Will)
Insurance coverage for peptide therapy falls into three tiers, and understanding which tier your peptide sits in saves you from spending hours on hold with your insurer only to hear "not covered."
Tier 1: FDA-approved peptide drugs. Semaglutide (Ozempic, Wegovy, Rybelsus), tirzepatide (Mounjaro, Zepbound), liraglutide (Saxenda, Victoza), and bremelanotide (Vyleesi) are approved drugs with NDAs. Insurance can cover them because they have gone through the FDA approval process. Whether your specific plan does cover them depends on the indication (diabetes vs. weight loss), your formulary, and whether you meet prior authorization criteria.
Tier 2: Compounded versions of FDA-approved peptides. Compounded semaglutide from a 503A pharmacy was widely covered by cash-pay telehealth clinics during the shortage era but was almost never covered by traditional insurance. The shortage has ended, and the legal basis for compounding has largely expired.
Tier 3: Non-FDA-approved peptides. BPC-157, TB-500, epitalon, selank, CJC-1295/ipamorelin, and every other peptide that has not gone through FDA drug approval. Insurance does not cover these because they are classified as experimental or wellness treatments rather than medically necessary interventions. No amount of appealing will change this. There is no billing code, no formulary listing, and no medical necessity pathway for unapproved substances.
The distinction is binary: if the FDA has approved a peptide drug for a specific indication, insurance coverage is possible. If it has not, insurance coverage is not.
FDA-Approved GLP-1s: The Coverage You Can Fight For
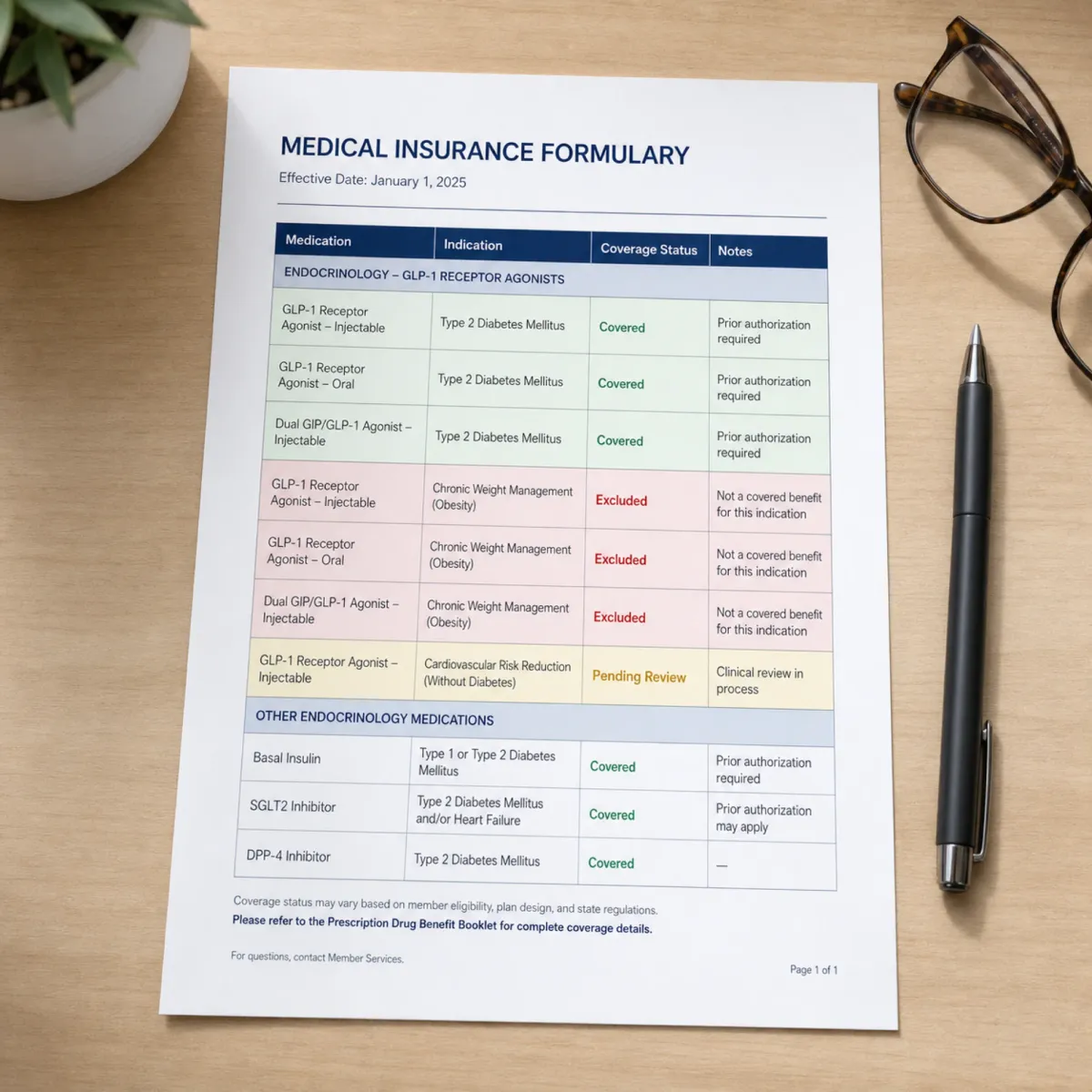
Even within the FDA-approved tier, coverage is not guaranteed. It depends on what you are being treated for.
GLP-1 drugs approved for type 2 diabetes (Ozempic, Mounjaro, Victoza) have broader coverage because diabetes is a well-established medical condition with clear diagnostic criteria. Most commercial insurance plans, Medicare Part D, and Medicaid programs include at least one GLP-1 on their formulary for diabetes management.
GLP-1 drugs prescribed for weight loss face a different reality. Most employer and Marketplace plans exclude GLP-1s for weight loss. The decision depends on your employer's benefit design, the drug's formulary placement, and insurer utilization management policies. Even if you are medically eligible, policy barriers often block access.
| Drug | Indication | Typical Commercial Coverage | Medicare Part D |
|---|---|---|---|
| Ozempic (semaglutide) | Type 2 diabetes | Usually covered (preferred formulary tier varies) | Covered |
| Wegovy (semaglutide) | Obesity/weight management | Often excluded; employer-dependent | Not covered (Bridge program starting July 2026) |
| Mounjaro (tirzepatide) | Type 2 diabetes | Usually covered | Covered |
| Zepbound (tirzepatide) | Obesity/weight management | Often excluded; employer-dependent | Not covered (Bridge program starting July 2026) |
| Saxenda (liraglutide) | Obesity/weight management | Rarely covered | Not covered |
| Vyleesi (bremelanotide) | HSDD (female sexual dysfunction) | Rarely covered; specialty tier | Covered if medically necessary |
The coverage gap between diabetes and obesity indications creates a perverse incentive. Some patients with both conditions receive their GLP-1 covered under the diabetes indication while benefiting from the weight loss effect. If the same patient only had obesity without diabetes, the identical drug at the identical dose would be denied.
Compounded Peptides: Why Most Plans Say No
Traditional health insurance rarely covers compounded medications of any kind, and compounded peptides are no exception. The reasons are structural, not arbitrary.
Insurance plans cover FDA-approved drugs because the approval process generates the safety and efficacy data that insurers use to justify coverage decisions. Compounded drugs bypass this process. They are not reviewed by the FDA for safety or efficacy. They do not have NDAs. They are not listed in drug compendia that insurers use for formulary decisions.
From the insurer's perspective, covering a compounded peptide would mean paying for a product with no FDA efficacy data, no standardized dosing, variable quality depending on the compounding pharmacy, and no post-market surveillance. The liability exposure alone makes coverage impractical.
Some specialty clinics accept HSA or FSA cards for peptide therapy, and financing options exist at some practices. But these are patient-funded channels, not insurance coverage.
Prior Authorization: The Gatekeeper Between You and Coverage
Even when your plan covers a GLP-1 drug, prior authorization stands between your prescription and your pharmacy counter. Expect prior authorization, ongoing documentation requirements, and potentially high out-of-pocket costs even with coverage.
Prior authorization for GLP-1 weight loss drugs typically requires:
- Documented BMI above a threshold (usually 30, or 27 with comorbidities)
- Evidence of failed lifestyle interventions (diet, exercise, behavioral counseling)
- Sometimes evidence of failed prior pharmacotherapy
- A letter of medical necessity from your prescriber
- Regular follow-up documentation showing continued medical need
The process is designed to be difficult. Insurers use prior authorization as a utilization management tool because the eligible population is enormous and the per-patient cost is high. The AMA has called for insurance coverage parity for emerging obesity treatments, but policy change moves slowly when billions of dollars are at stake.
Step therapy adds another layer. Some plans require you to try and fail on a cheaper medication (liraglutide) before approving a more expensive one (semaglutide or tirzepatide). Each step takes weeks to months, during which you either go without treatment or pay out of pocket.
Medicare, Medicaid, and the GLP-1 Coverage Gap
Medicare has the most significant coverage gap for GLP-1 weight loss drugs, and the most active effort to close it.
Medicare is statutorily prohibited from covering drugs used for weight loss. This exclusion dates back to the original Medicare statute and means that Part D plans cannot include Wegovy or Zepbound on their formularies when prescribed for obesity. The same drugs are covered when prescribed for diabetes or cardiovascular risk reduction.
The federal government is attempting to work around this prohibition through two programs:
Medicare GLP-1 Bridge (July 1 - December 31, 2026): This short-term program covers Wegovy and Zepbound for eligible Medicare Part D enrollees at a $50 copayment. Eligibility requires BMI of 35 or more alone, or 27 or more with additional clinical criteria. The program operates outside the Part D benefit structure, meaning the $50 copay does not count toward the Part D deductible or the $2,100 out-of-pocket spending cap.
BALANCE Model (starting 2027): A multi-year CMS demonstration program that will test sustained Medicare coverage of GLP-1s for obesity. Part D plan participation is voluntary, which means beneficiaries may need to switch plans during the 2027 open enrollment period to maintain coverage.
A previous KFF analysis estimated that close to 14 million Medicare beneficiaries had a diagnosis of overweight or obesity in 2020, though the specific Bridge program eligibility criteria would reduce that number substantially.
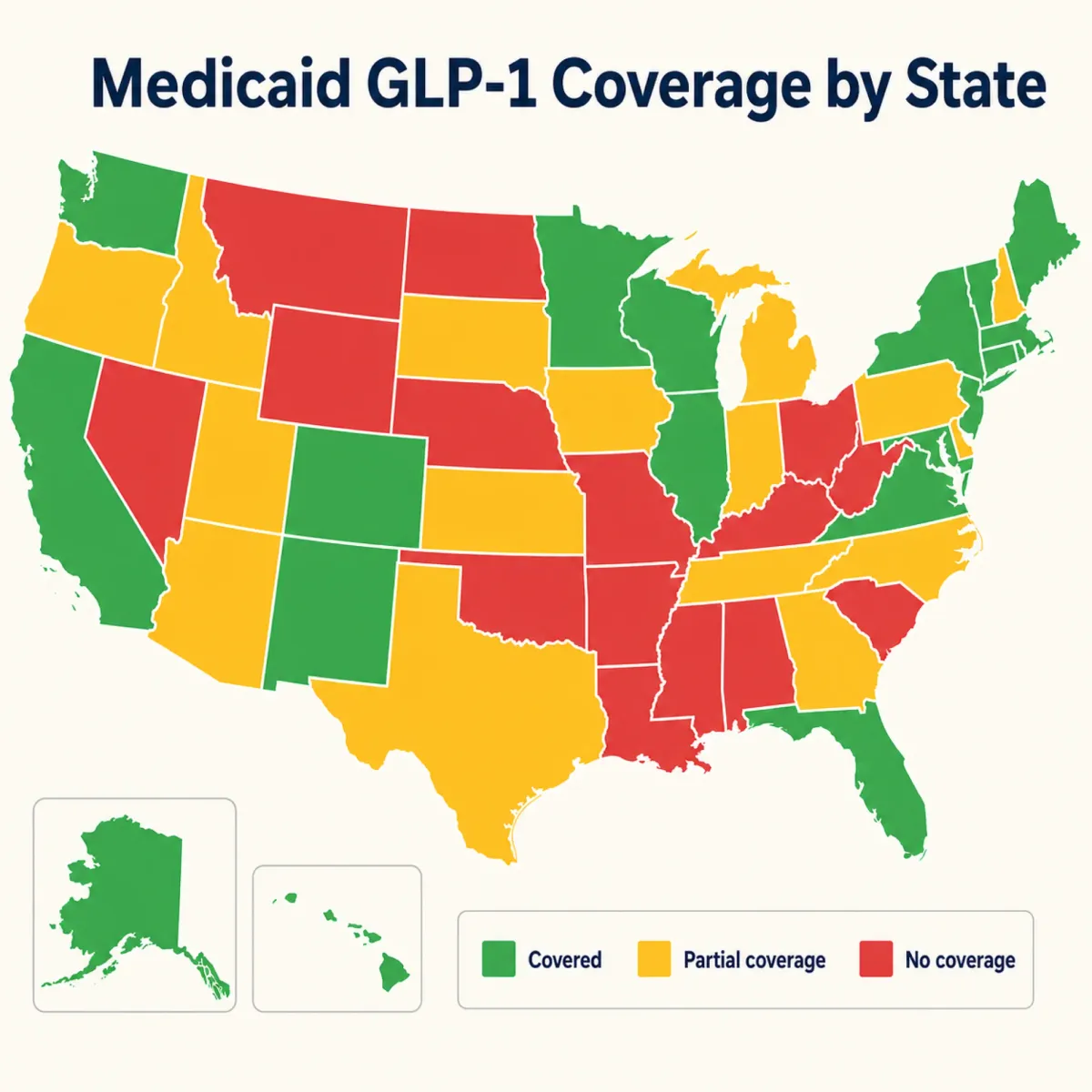
Medicaid coverage varies by state. Medicaid has low out-of-pocket costs and covers virtually all drugs, but only a few states cover anti-obesity medications. Even in states that do, access restrictions like prior authorization and prescriber limitations create barriers.
HSA and FSA: The Tax-Advantaged Workaround
When insurance says no, tax-advantaged health accounts offer a partial workaround for peptide therapy costs.
HSA (Health Savings Account) and FSA (Flexible Spending Account) funds can be used for qualifying medical expenses. The key question is whether your specific peptide therapy qualifies.
FDA-approved peptide drugs prescribed by a licensed provider for a diagnosed medical condition are generally HSA/FSA eligible. If your doctor prescribes semaglutide for type 2 diabetes and your insurance does not cover it, you can pay with HSA/FSA funds. The prescription itself establishes medical necessity.
Compounded peptides from a 503A pharmacy, prescribed by a licensed provider for a specific medical condition, may also qualify as HSA/FSA eligible medical expenses. The IRS defines eligible expenses broadly as amounts paid for the "diagnosis, cure, mitigation, treatment, or prevention of disease." A compounded peptide prescribed by a physician for a diagnosed condition meets this definition, even though the product is not FDA-approved.
Research peptides purchased without a prescription from a gray-market website do not qualify. They are not prescribed by a provider, they are not dispensed by a licensed pharmacy, and they carry no medical necessity documentation.
Practical tip: If you are paying out of pocket for peptide therapy through a telehealth clinic, ask the clinic for a superbill (itemized receipt with CPT and diagnosis codes). This documentation supports HSA/FSA reimbursement even when insurance does not cover the treatment. Keep all COAs and prescriptions as backup documentation in case of an IRS audit.
How to Appeal a Denied Peptide Therapy Claim
If your insurance denied coverage for an FDA-approved GLP-1 drug, you have the right to appeal. The process is regulated by federal law (ERISA for employer plans, ACA for marketplace plans) and follows a defined sequence.
Step 1: Get the denial in writing. Request the specific reason for denial. Common reasons include: not medically necessary, not on formulary, prior authorization not completed, step therapy not followed, or diagnosis not covered.
Step 2: Internal appeal. File a written appeal with your insurer within the deadline specified in the denial letter (usually 180 days). Include: your prescriber's letter of medical necessity, relevant clinical documentation (BMI, comorbidities, failed prior interventions), and any clinical guidelines supporting the treatment.
Step 3: External review. If the internal appeal is denied, you have the right to an independent external review. An outside physician reviews your case without insurer involvement. For ERISA plans, request an external review through your insurer. For marketplace plans, your state insurance department manages the process.
Step 4: Peer-to-peer review. Some insurers offer a peer-to-peer call where your prescriber speaks directly with the insurer's medical director. This is often the most effective step because it puts two physicians in direct conversation about your clinical situation.
Appeals succeed more often than most patients expect. The denial is often a first-pass utilization management decision, not a final clinical judgment. Having your prescriber actively involved in the appeal process significantly improves the outcome.
Frequently Asked Questions
Will insurance ever cover BPC-157 or TB-500?
Not under current regulations. Insurance covers FDA-approved drugs. BPC-157 and TB-500 are not FDA-approved and have no NDA. Even if they are added to the 503A bulks list (pending PCAC review in July 2026), that allows compounding pharmacies to make them, not insurance companies to cover them. Coverage would require an FDA drug approval process that no manufacturer has initiated for these peptides.
Can I use my HSA to pay for peptide therapy?
If the peptide is prescribed by a licensed provider for a diagnosed medical condition and dispensed by a licensed pharmacy, HSA funds are generally eligible. This includes both FDA-approved drugs and compounded peptides from 503A pharmacies. Research chemicals purchased without a prescription do not qualify.
What is the Medicare GLP-1 Bridge program?
A short-term CMS program running July 1 through December 31, 2026 that covers Wegovy and Zepbound for Medicare Part D enrollees with BMI 35+ (or 27+ with clinical criteria) at a $50 copayment. It operates outside the Part D benefit, so the copay does not count toward deductibles or out-of-pocket caps. It transitions to the voluntary BALANCE Model in 2027.
My GLP-1 was denied for weight loss but I also have diabetes. Can I get it covered?
Yes, potentially. If you have a type 2 diabetes diagnosis, GLP-1 drugs prescribed for diabetes management are covered under most plans and Medicare Part D. The same drug at the same dose may be approved when the billing code reflects a diabetes indication rather than an obesity indication. Discuss with your prescriber whether a diabetes-based prescription is clinically appropriate for your situation.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











