
What the DUTCH test measures (and why blood work misses it)
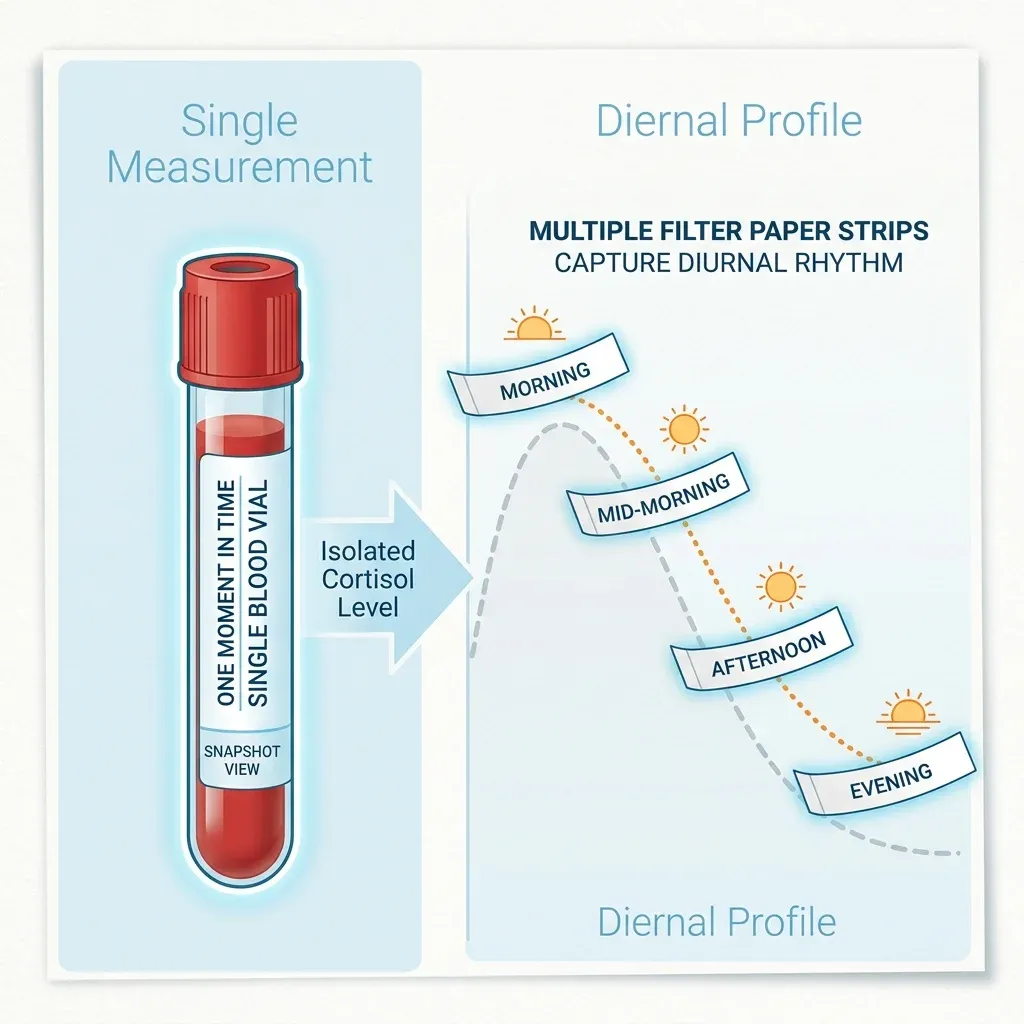
A hormone blood panel gives you one number from one blood draw at one time of day. If your doctor orders a morning cortisol, they see what your adrenal glands were doing at 8:17am on a Tuesday. That number can look perfectly normal while your cortisol pattern falls apart by afternoon.
The DUTCH test -- Dried Urine Test for Comprehensive Hormones -- works differently. Developed by Precision Analytical and founder Mark Newman, M.S., the test collects four dried urine samples across the day: at waking, two hours after waking, late afternoon, and bedtime. Those samples are analyzed using liquid chromatography tandem mass spectrometry (LC-MS/MS), producing a profile of 35 hormones and metabolites covering estrogen, progesterone, testosterone, DHEA-S, cortisol, and their downstream breakdown products.
The metabolites are where DUTCH pulls ahead of standard labs. When your body finishes using a hormone, the liver and kidneys convert it into water-soluble byproducts that exit through urine. These metabolites show how your body processes hormones -- not just how much is circulating. Blood tells you the level. Dried urine tells you the level, the pattern across the day, and which metabolic pathways are handling the cleanup.
The analytical method matters too. Most clinical labs use immunoassays -- antibody-based tests that are fast and cheap but can cross-react with similar molecules, inflating or distorting results. The DUTCH test uses LC-MS/MS, the same method preferred by the Mayo Clinic and Quest Diagnostics for salivary cortisol. LC-MS/MS identifies molecules by exact mass and fragmentation pattern instead of relying on antibody binding, which cuts false positives.
Does filter paper actually work for this? The published evidence says yes. A 2020 study in the Journal of Clinical and Translational Endocrinology by Newman, Curran, and Mayfield found near-ideal agreement between dried and liquid urine, with intraclass correlation coefficients (ICCs) of 0.99 for free cortisol, 0.97 for cortisone, and 0.96 for cortisol metabolites. A follow-up in BMC Chemistry confirmed ICCs above 0.90 for all reproductive hormones measured in dried versus liquid urine, with 14 of 17 metabolites showing excellent agreement between the 4-spot method and a full 24-hour collection.
A fair criticism: those validation studies were conducted by the test's creator. Independent replication at other institutions is limited. The analytical accuracy looks solid based on published data, but large clinical outcome studies comparing DUTCH-guided treatment decisions to standard care don't exist yet.
Cortisol metabolites: the 24-hour picture a morning blood draw can't show
Most endocrinology visits skip a detail that changes the interpretation: free cortisol accounts for less than 5% of total cortisol secretion. The other 95% gets converted into metabolites -- primarily alpha-tetrahydrocortisol (aTHF), beta-tetrahydrocortisol (bTHF), and tetrahydrocortisone (THE). A blood draw or saliva test measuring free cortisol catches a sliver of what's happening. Judging total cortisol output by free cortisol alone is like estimating a river's flow from the surface current.
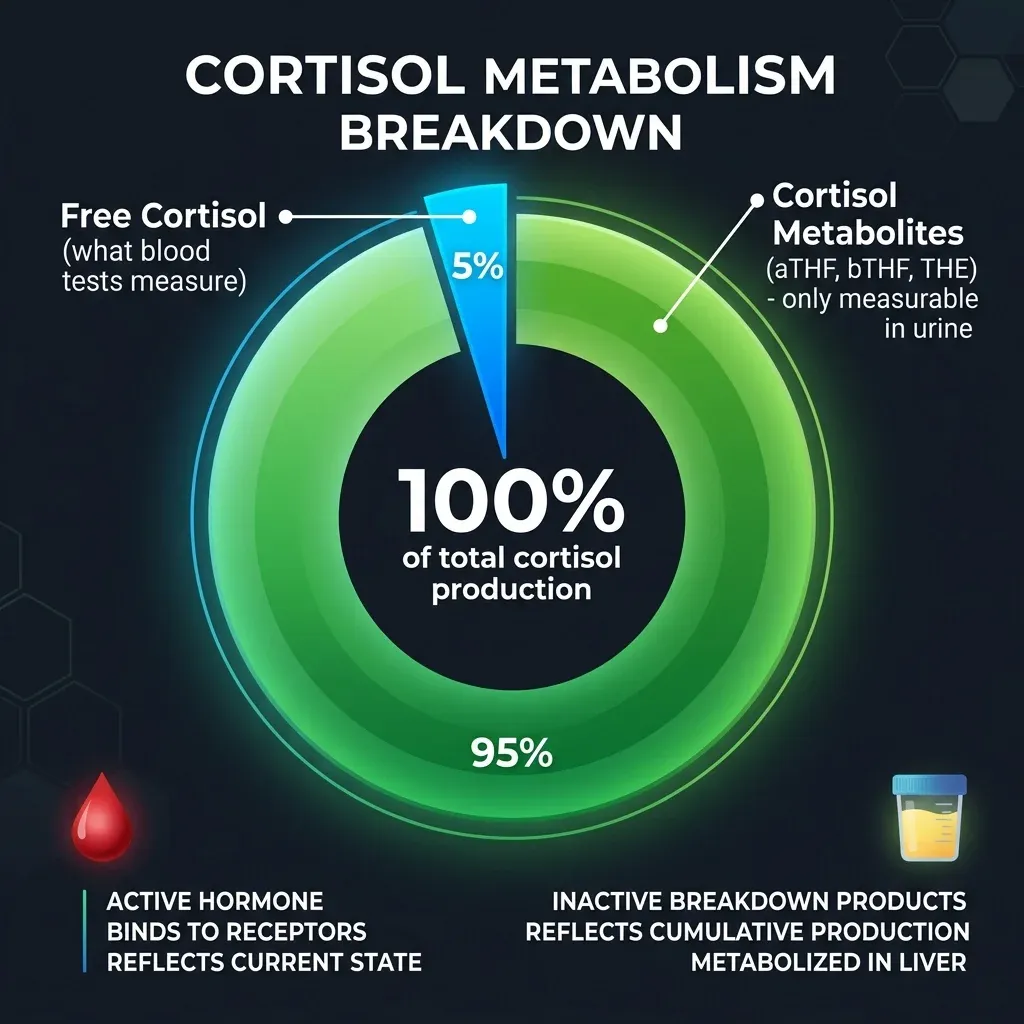
Why does the other 95% matter? Because cortisol clearance rate can shift independently of cortisol production. Research in the clinical validation documentation shows that metabolized cortisol tracks with BMI in over 5,000 women, while free cortisol stays flat regardless of body weight. Tomlinson's research found a 36% decrease in metabolized cortisol following weight loss, with statistical correlation between cortisol metabolites and both waist circumference and intra-abdominal fat.
Two patients can have identical free cortisol levels but very different metabolized cortisol, pointing to different clinical pictures. Someone on thyroid medication pushing T3/T4 too high might show low free cortisol -- not because the adrenals are failing, but because excess thyroid hormone accelerates cortisol clearance. Pull back on the thyroid dose, and free cortisol normalizes without touching the adrenals.
The diurnal cortisol pattern adds another dimension. Healthy cortisol peaks 30-45 minutes after waking, declines through the day, and bottoms out around midnight. A meta-analysis of 208 studies by Miller and colleagues found that chronic stress flattens this curve -- the morning peak blunts, the evening dip disappears, and cortisol sits at an unhealthy midrange throughout the day. Mathews (2006) found that patients with flattened curves were more than three times more likely to have coronary artery calcification, and the Whitehall II study of over 4,000 people linked flat cortisol curves directly to increased cardiovascular mortality.
A single morning blood draw cannot detect a flattened curve. It might show the peak looks fine while the rest of the day is a metabolic disaster. The 4-spot dried urine collection captures the slope -- and the diurnal pattern matches salivary cortisol testing with no statistically significant difference (P=0.83, n=68).
Estrogen pathways and methylation: detoxification meets cancer risk
Blood estrogen tests tell you how much estradiol or estrone is circulating. That is useful information. But your body doesn't just produce estrogen and reabsorb it. Estrogen gets processed through specific detoxification pathways in the liver, and which pathway dominates has clinical consequences -- particularly for breast cancer risk.
The DUTCH test measures five Phase 1 estrogen metabolites and one Phase 2 metabolite, then calculates two ratios worth paying attention to: the 2-OH/4-OH ratio and the 2-OH/16-OH ratio.
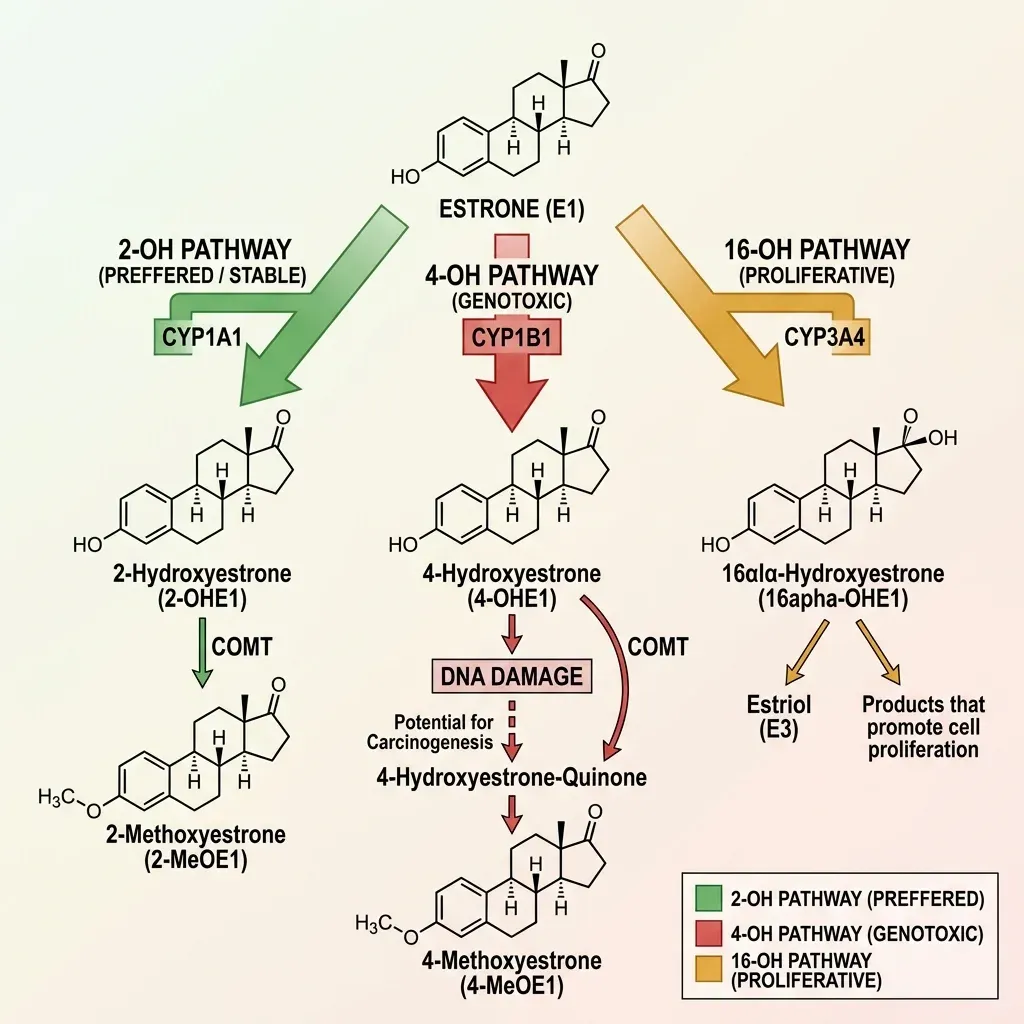
Phase 1 metabolism works through three pathways. The 2-OH pathway (CYP1A1 enzyme) is the preferred route, producing the most stable metabolites. The 4-OH pathway (CYP1B1 enzyme) is the concerning one. These metabolites can become reactive quinones that bind directly to DNA, forming depurinating adducts. In a 2019 study, Miao et al. reported that 4-hydroxy estrogen was the most significant breast cancer risk factor found in urine samples when comparing patients with breast cancer to healthy controls. Cavalieri and Rogan (2010) confirmed the connection -- depurinating estrogen-DNA adducts were significantly elevated in urine from women with breast cancer versus healthy women.
The 16-OH pathway (CYP3A4 enzyme) produces metabolites that are less directly DNA-damaging but promote tissue growth. Elevated 16-OH-E1 levels tend to appear alongside heavy menstrual bleeding, breast tenderness, endometriosis, and fibroids. For women with a history of estrogen-sensitive breast cancer, 16-OH dominance may increase recurrence risk.
Phase 2 metabolism -- methylation specifically -- is where dangerous Phase 1 metabolites get neutralized. The COMT enzyme (catechol-O-methyltransferase) methylates the 2-OH and 4-OH catechol estrogens, converting them into inactive forms the body can excrete. The DUTCH test measures 2-methoxyestrone as a direct marker of this methylation activity. When methylation slows -- from COMT or MTHFR genetic variants, nutrient deficiencies (B vitamins, magnesium), or environmental factors -- those reactive Phase 1 metabolites stick around longer, widening the window for DNA damage.
None of this shows up on a standard blood estradiol test. A woman could have normal estradiol levels but a dangerously low 2-OH/4-OH ratio, meaning her estrogen is channeling through the most DNA-damaging pathway available. That gap is what the DUTCH test is built to fill.
DUTCH Complete vs DUTCH Plus vs standard labs
The question most people land on: which test do I actually need? Cost and insurance coverage are real constraints here.
The DUTCH test costs $300 to $700 depending on the version, and health insurance does not typically cover it. Precision Analytical considers itself out-of-network for all plans. You can submit receipts for possible reimbursement if a provider ordered the test, but plan on paying out of pocket.
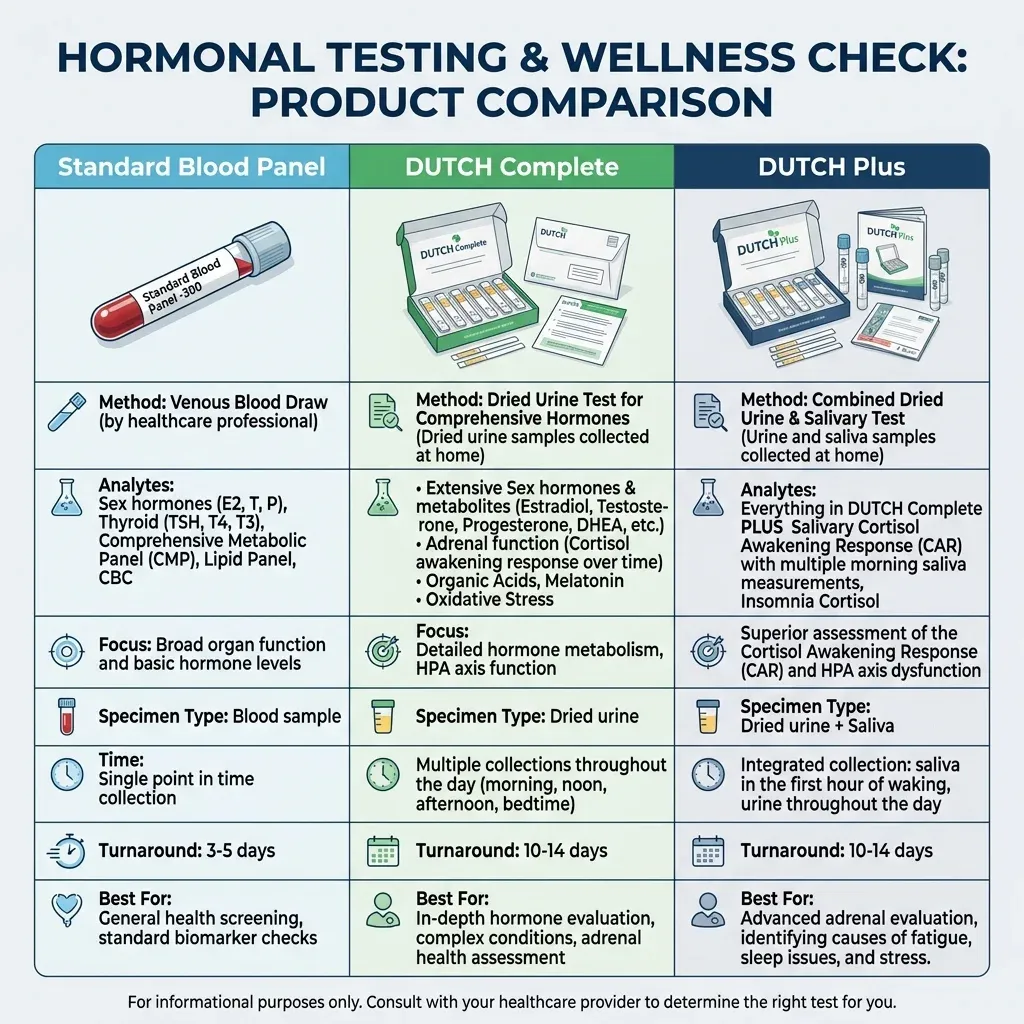
A standard hormone blood panel through your primary care provider -- estradiol, testosterone, DHEA-S, morning cortisol, thyroid panel -- generally runs $50-300 with insurance and remains the standard of care for diagnosing hypothyroidism, Cushing syndrome, or hypogonadism. Blood tests measure circulating hormone levels reliably and are backed by decades of clinical guidelines.
Cost snapshot: Blood hormone panel with insurance: $50-300. DUTCH Complete: ~$399. DUTCH Plus: ~$499-599. Standard saliva cortisol panels (ZRT Laboratory, Genova Diagnostics): $100-300.
The DUTCH Complete collects four dried urine samples and measures 35 analytes: sex hormones, their metabolites, diurnal free cortisol and cortisone, metabolized cortisol, organic acids (markers for B12, B6, glutathione, dopamine, norepinephrine), melatonin, and an oxidative stress marker (8-OHdG). It does not include the Cortisol Awakening Response.
The DUTCH Plus includes everything in the DUTCH Complete and adds five saliva collections (at waking, +30 min, +60 min, afternoon, and bedtime) to capture the Cortisol Awakening Response. The CAR -- the spike in cortisol that normally happens within 30-45 minutes of waking -- can only be accurately assessed through saliva because a waking urine sample represents cortisol accumulated across the entire night, not the precise waking moment. Researchers at Northwestern University found that the CAR -- not absolute morning cortisol -- correlated significantly with risk for Major Depressive Disorder.
When does a standard blood panel make more sense? If you suspect thyroid dysfunction, need a Cushing's or Addison's workup, want fertility hormone levels (FSH, LH, AMH), or need insurance to cover the bill. Blood tests are validated, established, and covered. If your symptoms are well-explained by standard labs, there's no reason to spend $400+ on a DUTCH test.
When to order a DUTCH test (and when not to)
The DUTCH test fills a specific clinical niche. It doesn't replace standard bloodwork and it's not a screening tool. It adds value when standard labs come back "normal" but symptoms persist, or when understanding the metabolic pathway matters as much as knowing the hormone level.
| Consider DUTCH testing when | Stick with standard labs when |
|---|---|
| You suspect cortisol pattern dysfunction (fatigue, insomnia, stress-related symptoms) but morning cortisol is normal | You need to rule out Cushing syndrome or adrenal insufficiency (requires serum ACTH stim test) |
| You want to understand estrogen metabolism pathways, particularly with personal or family history of hormone-sensitive cancers | You need basic fertility hormone levels (FSH, LH, AMH) |
| You are monitoring bioidentical hormone replacement therapy and want to see how supplemented hormones are metabolized | You suspect thyroid dysfunction (TSH, free T3, free T4) |
| A functional medicine provider is guiding treatment based on metabolic patterns | Insurance coverage matters and you need a cost-effective starting point |
| You have unexplained symptoms (fatigue, weight gain, mood instability) that standard labs haven't explained | You have kidney disease or abnormal GFR (urine testing may give misleading results) |
The DUTCH test should not be used to diagnose adrenal insufficiency or Cushing syndrome. Those conditions still require serum-based dynamic testing -- an ACTH stimulation test or dexamethasone suppression test. The DUTCH test is a functional assessment tool, not a replacement for standard endocrine workups.
Kidney function is another exclusion. Patients with abnormal glomerular filtration rates should not rely on urine-based cortisol testing (DUTCH or 24-hour collection) because low GFR can artificially reduce urinary cortisol levels.
Over 4,000 MDs currently use the DUTCH test in their practice, making physicians the most common practitioner type ordering it. It isn't exclusively used by naturopaths. But interpretation requires training that falls outside standard medical education, so finding a provider who knows what to do with the results matters as much as the test itself.

How to read your DUTCH test results
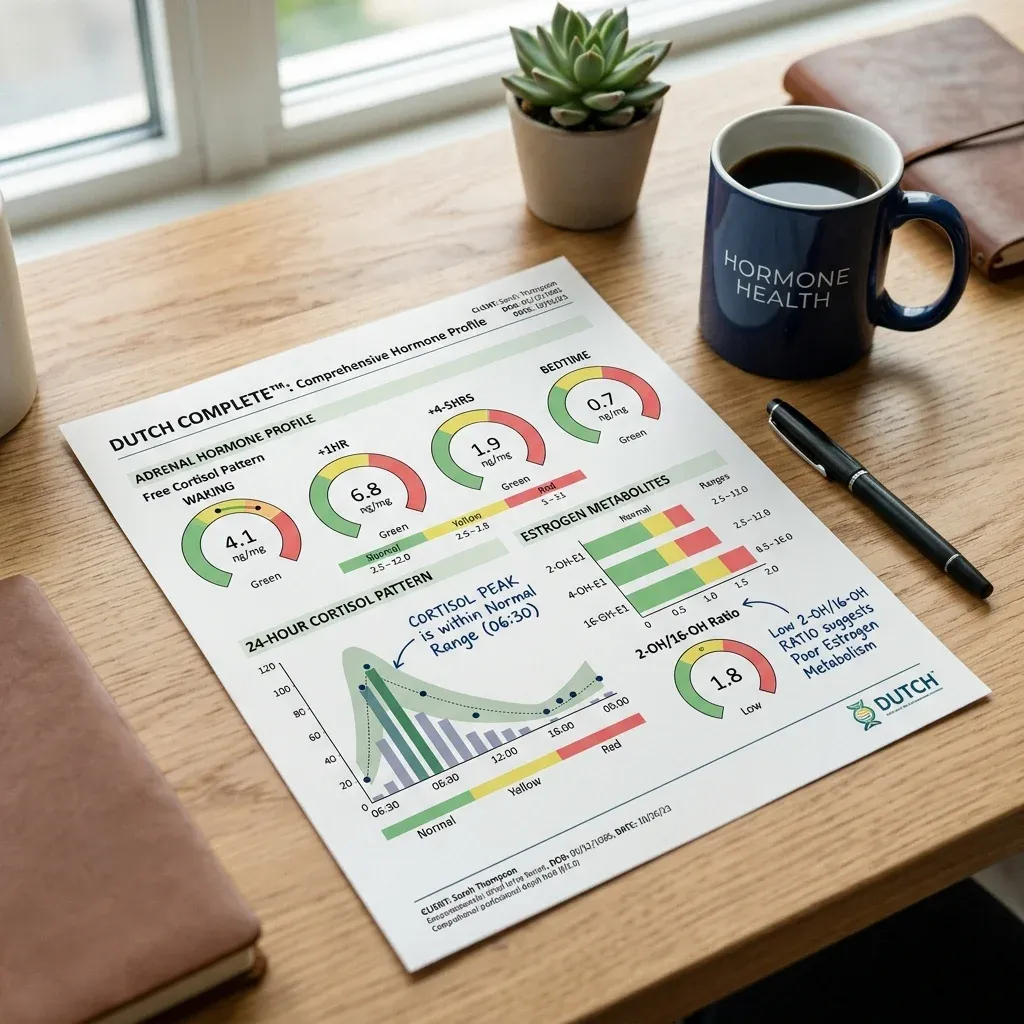
A DUTCH report is dense -- color-coded dials, bar charts, metabolic pathway diagrams. Breaking it into three zones makes it more manageable.
Zone 1: The diurnal cortisol curve. This is the most readable section. You're looking at free cortisol and free cortisone levels plotted across four time points. A healthy pattern shows the highest values at waking, declining progressively to the lowest point at bedtime. If the curve is flat -- morning and evening values sit close together -- that pattern is associated with chronic stress and, based on the Whitehall II study data, increased cardiovascular mortality. Elevated evening values may correlate with insomnia or difficulty winding down.
Zone 2: Free cortisol vs metabolized cortisol. This is where DUTCH catches things standard labs miss. When free cortisol is low but metabolized cortisol (THF + THE) is high, it suggests rapid cortisol clearance -- the body makes plenty of cortisol but burns through it too fast. This pattern appears in obesity, hyperthyroidism, systemic inflammation, and insulin resistance. The reverse -- high free cortisol, low metabolized cortisol -- points to impaired clearance, which can happen with hypothyroidism or liver dysfunction. A provider who only sees "low cortisol" on a blood test might assume the adrenals are failing, when the actual problem is clearance rate.
Zone 3: Estrogen metabolism ratios. Pay attention to the 2-OH/4-OH ratio and the 2-OH/16-OH ratio. A low 2-OH/4-OH ratio means more estrogen goes through the genotoxic 4-OH pathway, associated with increased breast and prostate cancer risk. A low 2-OH/16-OH ratio indicates preference for the proliferative 16-OH pathway, which can worsen estrogen-dominant symptoms like heavy bleeding and fibrocystic breast changes. The 2-methoxyestrone level shows whether Phase 2 methylation keeps pace with Phase 1 output -- a low reading means potentially harmful intermediates are accumulating faster than the body can neutralize them.
The creatinine correction in the DUTCH results is worth understanding. Urine concentration varies with hydration, so raw hormone levels would mislead without adjustment. Precision Analytical normalizes results to creatinine (excreted at a predictable rate) and applies a proprietary correction for age, sex, height, and weight. Their data shows this correction improves correlation with 24-hour urine values -- R-squared improves from 0.86 to 0.92 for estradiol.
The organic acids panel at the bottom of the report -- markers for B12 (methylmalonate), B6 (xanthurenate), glutathione (pyroglutamate), dopamine (homovanillate), norepinephrine/epinephrine (vanilmandelate), and melatonin (6-OHMS) -- provides context for the hormone results. Low B6, for instance, could explain sluggish estrogen metabolism, since B vitamins are cofactors in methylation. The 8-OHdG marker reflects oxidative DNA damage -- relevant to the estrogen pathway section above.
A DUTCH report requires a trained provider to interpret. The report includes embedded video tutorials and visual representations, but treatment decisions should come from someone with specific training in functional hormone interpretation -- whether an MD, DO, ND, or nurse practitioner with the relevant background.
Frequently asked questions
How accurate is the DUTCH test compared to blood testing?
For the analytes it measures, the DUTCH test shows strong analytical accuracy. Peer-reviewed studies in the Journal of Clinical and Translational Endocrinology and BMC Chemistry demonstrate intraclass correlation coefficients above 0.90 between dried urine and liquid urine for cortisol, cortisone, and reproductive hormones. Blood testing remains the gold standard for circulating hormone levels, particularly for diagnosing thyroid disorders, Cushing syndrome, and hypogonadism. The two methods measure different things -- blood captures what's circulating now, while DUTCH captures metabolic processing patterns across a full day.
Is the DUTCH test FDA-approved?
No. The DUTCH test uses LC-MS/MS, which falls under laboratory-developed tests (LDTs). LDTs are governed by CLIA (Clinical Laboratory Improvement Amendments), not the FDA. This is the same regulatory framework used by the Mayo Clinic and Quest Diagnostics for their LC-MS/MS assays. The filter paper used for sample collection has FDA approval for collecting whole blood, though no formal FDA clearance exists for its use with urine. Precision Analytical's lab undergoes regular CLIA inspections covering validation data, analytical performance, and QA/QC programs.
Can I order a DUTCH test without a provider?
Some direct-to-consumer options exist, but you'll need a healthcare provider to interpret the results meaningfully. The report contains complex metabolic pathway data that requires clinical context -- your symptoms, medications, medical history, and goals -- to translate into anything useful. Ordering without someone who can read the data is spending $400+ on information you can't act on.
How long do DUTCH test results take?
Results typically arrive within two to three weeks of the lab receiving your samples. Dried urine samples are stable at room temperature during shipping, so transit time doesn't affect sample quality.
DUTCH Complete or DUTCH Plus?
If your primary concern is sex hormone metabolism, estrogen pathways, or general cortisol patterns, the DUTCH Complete covers that. If stress response, HPA axis dysfunction, depression, anxiety, or morning fatigue are the reason you're testing, the DUTCH Plus adds the Cortisol Awakening Response via saliva, which can't be measured through urine alone and provides clinically distinct information about your brain's stress reactivity. The price difference is roughly $100-200.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











