
Your melatonin gummies worked fine at 38. What changed?
Between ages 40 and 55, 37% of women report sleep difficulties, according to the Study of Women's Health Across the Nation. By postmenopause, the numbers get worse: 35-60% of women experience clinical sleep disturbances. Most reach for melatonin. And for a while, it helps. Then it stops.
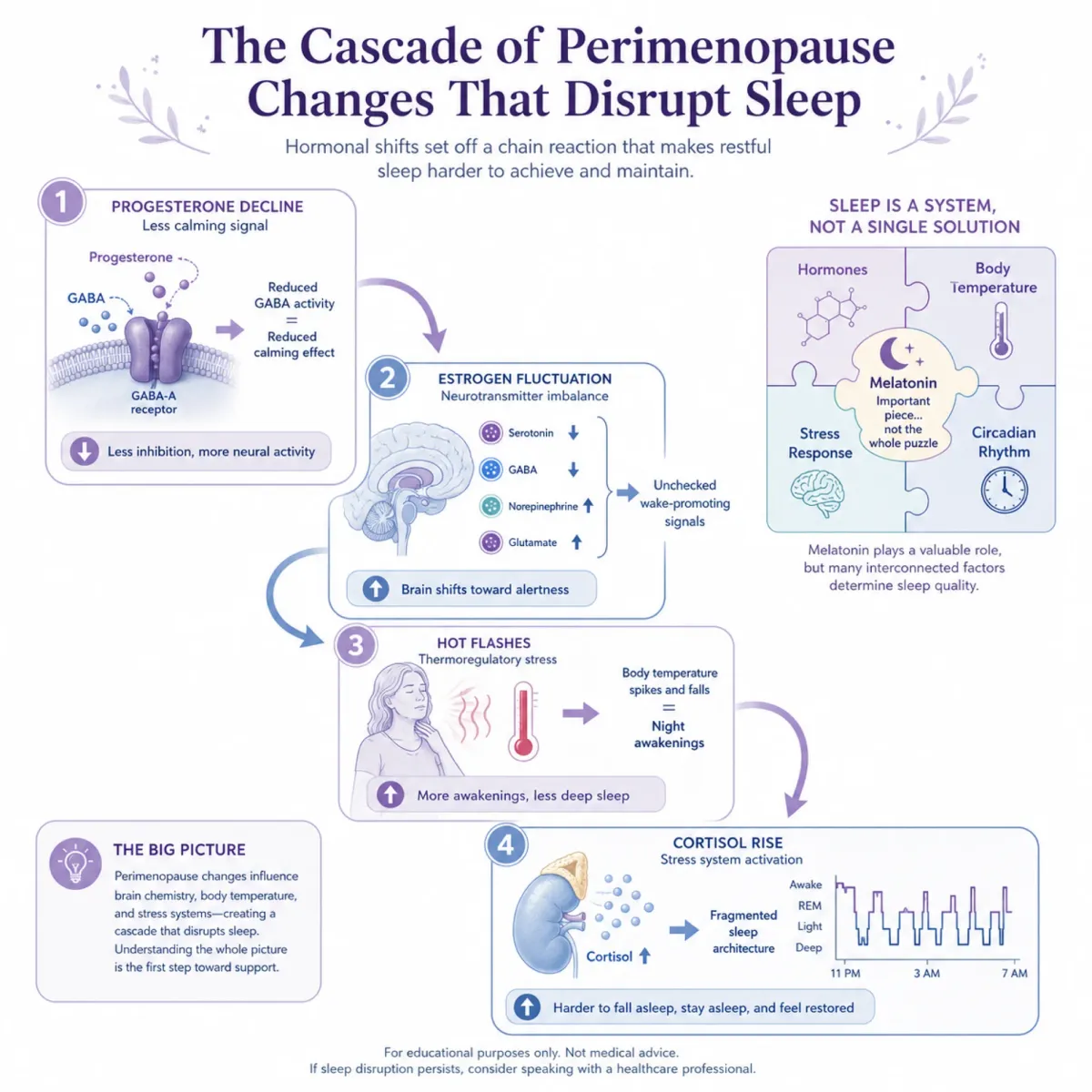
The problem is that perimenopausal insomnia usually isn't a melatonin deficiency problem. It's a cascade problem. Progesterone, which produces sedative and anxiolytic effects through metabolites acting on GABA receptors, drops first. Think of progesterone as your brain's built-in Xanax. When levels start swinging, the calming influence on your nervous system weakens, and the 3 a.m. wakeups begin.
Estrogen compounds it. Estrogen normally inhibits wakefulness neurotransmitters including acetylcholine, histamine, noradrenaline, and orexin. As levels fluctuate, those wake-promoting chemicals run unchecked. Research suggests the degree and dynamics of estrogen fluctuation matter more than the absolute level, which explains why some women with "normal" lab values still can't sleep.
Then there are hot flashes, which have a bidirectional relationship with sleep disruption and persist for 4-10 years on average. And cortisol, which tends to rise during menopause, further fracturing sleep architecture.
Melatonin does decline with age. Poor-sleeping menopausal women show smaller evening melatonin increases and a dim light melatonin onset delayed by about 50 minutes compared to good sleepers. But supplementing melatonin addresses one variable in a multi-variable problem. It reliably reduces sleep onset latency but its effects on sleep maintenance are "quantitatively rather moderate". Women who can fall asleep but can't stay asleep, or who wake drenched in sweat at 2 a.m., often find melatonin beside the point.
That gap between what melatonin addresses and what perimenopausal women actually experience is where peptide-based approaches have gained traction. Each targets a different part of the broken sleep machinery. Some have real trial data. Others are running on mechanism and clinical anecdote. Knowing the difference matters.
DSIP has a perfect name and imperfect evidence
Delta sleep-inducing peptide was isolated in 1977 from rabbit cerebral venous blood. Its proposed mechanism involves stimulating growth hormone-releasing hormone secretion, which promotes deeper sleep stages. Early small trials looked promising: a 1984 study of 10 insomnia patients showed improvements in sleep arousals, efficiency, and slow-wave sleep.
But the best-controlled trial deflated the excitement. A double-blind study of 16 chronic insomnia patients using intravenous DSIP over 5 nights found effects that were "weak and in part could be due to an incidental change in the placebo group." The researchers concluded that "short-term treatment of chronic insomnia with DSIP is not likely to be of major therapeutic benefit."
All human studies used intravenous dosing at 25 nmol/kg. No standardized subcutaneous protocol exists. DSIP is FDA Category 2 restricted due to immunogenicity concerns, and most positive data comes from 1980s studies with 5-10 subjects. No modern large-scale trials have followed up. Clinicians who use it typically embed it in broader peptide stacks, making its individual contribution hard to isolate.
The connection between growth hormone and sleep runs deeper than most people realize
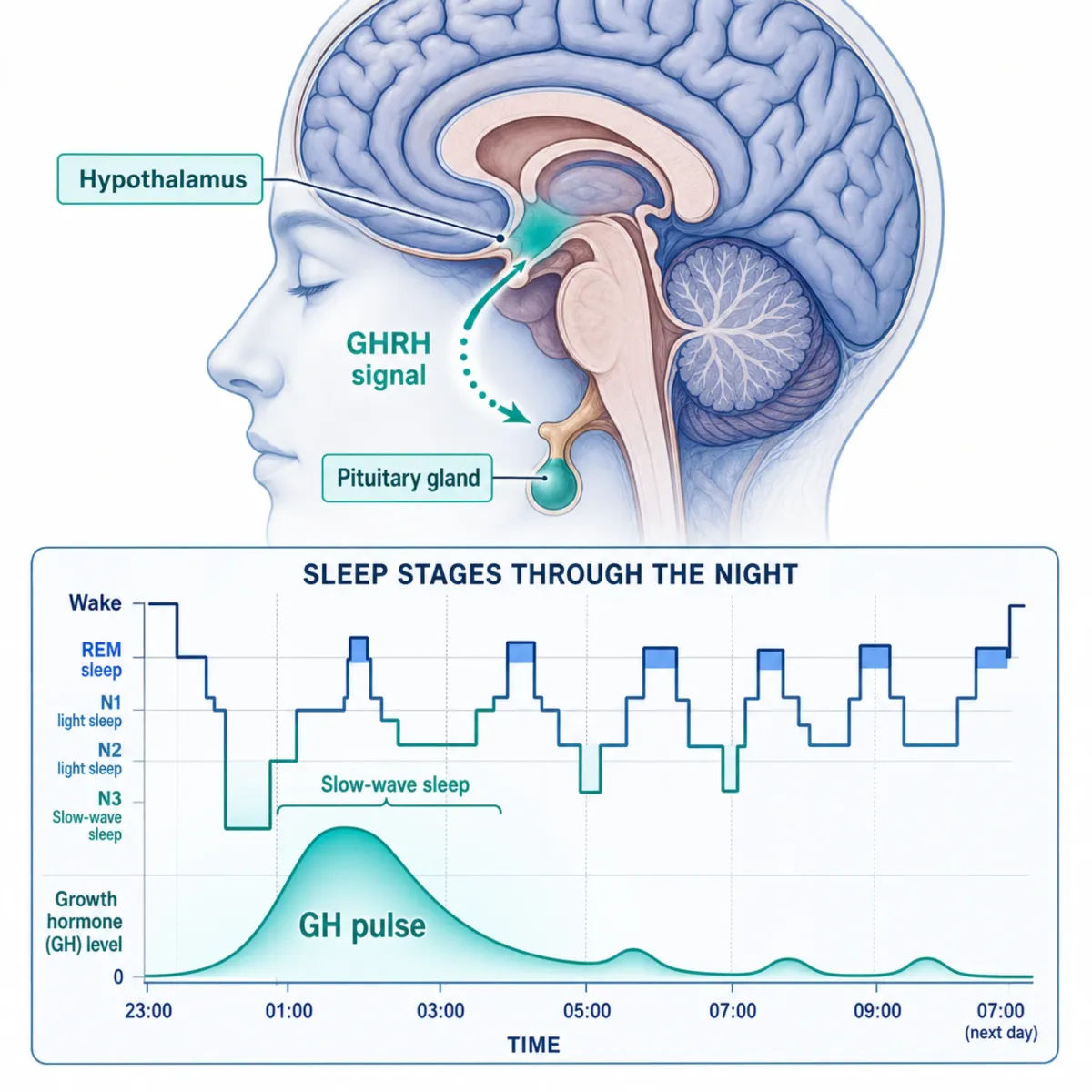
Your body's largest natural growth hormone pulse happens during the first cycle of deep sleep. This isn't coincidental. Growth hormone-releasing hormone (GHRH) doesn't just trigger GH release; it prompts an increase in slow wave sleep in healthy volunteers and simultaneously blunts cortisol. The two systems are intertwined like gears in a clock. When one slows, the other follows.
GH secretion declines with age, and slow-wave sleep shrinks with it. CJC-1295 mimics GHRH at the pituitary, while ipamorelin binds ghrelin receptors for GH release. Together, CJC-1295 provides sustained stimulation while ipamorelin delivers more immediate growth hormone release.
Research by J.C. Weikel at the Max Planck Institute showed that ghrelin increased slow-wave sleep during the total night and enhanced delta-wave activity in 7 subjects receiving intravenous ghrelin. Studies since the 1990s have confirmed that higher GHRH activity decreases wakefulness and increases slow-wave sleep.
An important distinction: taking exogenous GH injections is different from using secretagogues. A 2025 Frontiers in Endocrinology study found that exogenous GH injections suppress endogenous GHRH secretion and remain in serum for 10-16 hours, potentially blanketing the sleep window. Secretagogues instead stimulate your own pituitary to release GH in natural pulses, preserving the GHRH-sleep connection.
For perimenopausal women, ipamorelin's selectivity matters: it doesn't affect cortisol, unlike ghrelin itself, which increased cortisol during the initial night period in the Weikel study. Women already dealing with elevated cortisol benefit from a secretagogue that avoids piling on more.
Clinical outcomes come from integrative medicine practices, not large RCTs. Practitioners report improved sleep within 2-4 weeks of starting CJC-1295/ipamorelin. No randomized trial has tested this combination for sleep in perimenopausal women specifically.
When the problem isn't sleeplessness but the racing mind that causes it
Between 22% and 29% of women going through the menopausal transition experience depression or anxiety. For many of them, insomnia is downstream of the anxiety rather than the other way around. They're not lying awake because their sleep system is broken. They're lying awake because their brain won't stop rehearsing tomorrow's problems.
Selank, a synthetic analog of the naturally occurring immunomodulatory peptide tuftsin, was developed at the Institute of Molecular Genetics in Russia and has completed Phase 3 clinical testing as a selective anxiolytic. Its mechanism is unusual. Rather than binding directly to GABA receptors the way benzodiazepines do, Selank works through allosteric modulation of GABAA receptors. The distinction matters.
Volkova and colleagues examined 84 neurotransmission-related genes after Selank administration. At one hour, 45 genes showed mRNA changes. GABA receptor epsilon and theta subunits were suppressed 20-fold at 1 hour, then rebounded to 16-fold and 13-fold upregulation by 3 hours. This biphasic pattern suggests Selank resets the GABA system rather than sedating it.
Selank demonstrates anxiolytic activity comparable to benzodiazepines without amnesia, withdrawal, or dependence. The orexin data hints at why: the Hcrt gene (orexin precursor) increased 128-fold by 3 hours. Orexin maintains wakefulness. That upregulation likely explains why Selank reduces anxiety without causing drowsiness.
Semax works through BDNF upregulation and monoamine signaling rather than GABA. Some practitioners combine both: Selank for calming, Semax for daytime cognitive support. Both are intranasal with effects in 30-60 minutes. Neither has FDA approval, and the sleep evidence for Selank is inferred from its GABA and orexin effects rather than direct sleep trials.
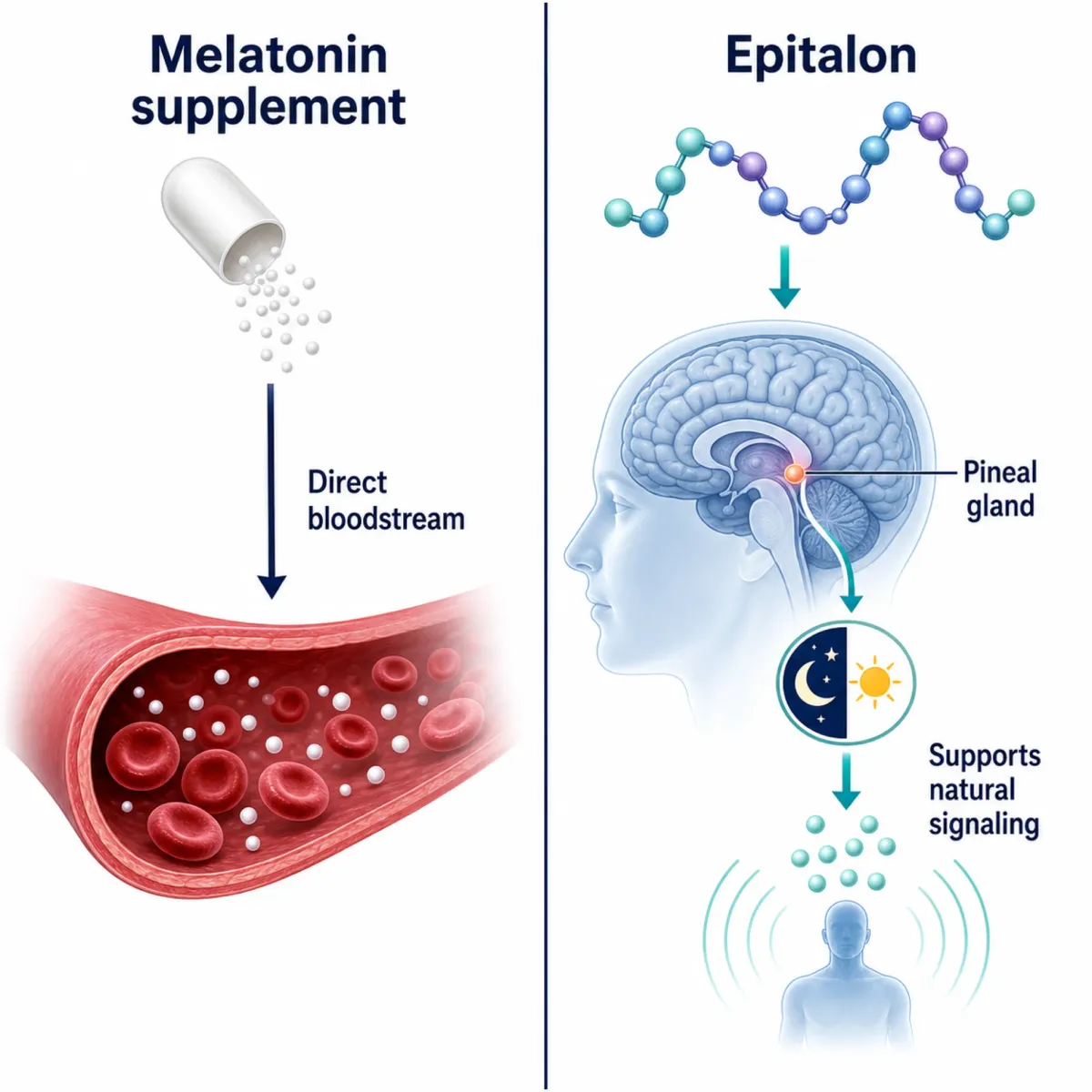
Epitalon doesn't replace your melatonin. It tries to make your pineal gland produce its own again.
Instead of supplementing melatonin from outside, what if you could restart the factory? Epitalon (Ala-Glu-Asp-Gly) is a synthetic tetrapeptide targeting the pineal gland. Developed by Russian gerontologist V.K. Khavinson from pineal tissue research begun in 1973, it upregulates AANAT and pCREB in pinealocytes. AANAT is the rate-limiting enzyme in melatonin synthesis, the bottleneck determining your pineal gland's melatonin output. In aged human pinealocytes, Epitalon selectively safeguarded cells from degenerative changes.
The best human evidence comes from a randomized clinical trial of 75 women who received 0.5 mg/day sublingual Epitalon for 20 days. Urinary melatonin metabolite increased 1.6-fold compared to placebo. Circadian gene expression shifted significantly: Clock gene expression decreased 1.8-fold, Cry2 doubled, and Csnk1e decreased 2.1-fold. In elderly humans and aged rhesus monkeys, the peptide preparations recovered night release of endogenous melatonin and normalized the hormone circadian rhythm, with no reported side effects.
| Epitalon evidence | Model | Finding | Strength |
|---|---|---|---|
| 75-woman RCT | Human | Melatonin metabolite up 1.6x; circadian gene shifts | Moderate (short duration, single trial) |
| Elderly + monkey study | Human/Primate | Night melatonin restored, rhythm normalized | Moderate (no sham control details in abstract) |
| Pinealocyte cultures | In vitro | AANAT/pCREB upregulated, cells protected | Mechanistic only |
| CBA mouse lifespan | Animal | 4x more mice reached 23 months | Preclinical |
Healthspan's evidence review is blunt: "Epitalon lives up to its hype mechanistically, but falls short in translational readiness." No large-scale RCTs exist. Only the all-L form has been studied. Oral bioavailability is poor, so the typical protocol uses subcutaneous injection in loading cycles of 10-20 days, once or twice yearly. The 75-woman trial proves Epitalon can shift circadian gene expression. Whether that translates to lasting sleep improvement remains unproven.
Glycine costs pennies and has better clinical evidence than peptides costing hundreds
Every other peptide here requires a prescription or gray-market supplier. Glycine is an amino acid available at any supplement store for under $15, found abundantly in collagen and bone broth. It also has something most sleep peptides lack: multiple randomized controlled trials.
A 2012 crossover trial by Bannai and colleagues tested 3 grams of glycine 30 minutes before bedtime in sleep-restricted volunteers. Results: significant fatigue reduction (p=0.022) and improved reaction time on day 1 (p=0.003) and day 3 (p=0.05). Earlier trials by Yamadera (2007) and Inagawa (2006) showed polysomnographic sleep quality improvements at the same dose.
The mechanism is well-mapped. Research by Nobuhiro Kawai at Ajinomoto and Seiji Nishino at Stanford showed glycine works through NMDA receptors in the suprachiasmatic nucleus (your brain's master clock), not glycine receptors. NMDA antagonists blocked the effect; strychnine (a glycine receptor blocker) didn't. Target confirmed: glycine induces peripheral vasodilation via NMDA receptors.
Think of it like opening a window on a warm night. Glycine activates the SCN, triggering dose-dependent core body temperature drops by pushing blood flow to the skin. This thermal shift happens 30-45 minutes after dosing, mimicking the natural signal your body uses to initiate sleep. When researchers destroyed the SCN in animal models, glycine failed to affect sleep at all.
For perimenopausal women: glycine does not alter melatonin levels or clock genes like Bmal1 and Per2. It works through an independent pathway, which means it could help even when melatonin has stopped working. Different problem, different solution.
| Peptide/compound | Human sleep RCT data | Mechanism certainty | Accessibility |
|---|---|---|---|
| Glycine | Multiple RCTs (Bannai 2012, Yamadera 2007, Inagawa 2006) | High (SCN/NMDA pathway confirmed) | OTC supplement, ~$15 |
| DSIP | One weak double-blind trial (16 patients) | Low (mechanism unclear) | FDA restricted, prescription only |
| CJC-1295/Ipamorelin | None for sleep specifically | Moderate (GHRH-SWS link established) | Prescription, compounding pharmacy |
| Selank | None for sleep (Phase 3 for anxiety only) | Moderate (GABA modulation confirmed) | Not FDA-approved, intranasal |
| Epitalon | One 20-day circadian gene trial (75 women) | Moderate (AANAT pathway confirmed) | Not FDA-approved, injection cycles |
The dose across studies is consistent: 3 grams before bed. Side effects are minimal. The main limitation of the glycine data is sample size. The Bannai trial had 7 participants. That's enough to demonstrate a mechanistic effect but not enough to make population-level claims. Still, for a woman weighing whether to start with a $15 supplement or a $400 peptide prescription, the risk-to-evidence ratio favors trying glycine first.
What practitioners are actually prescribing (and in what order)
No clinical guideline exists for peptide-based sleep protocols in perimenopausal women. What follows reflects integrative medicine practice patterns, not randomized trial data.
Cognitive behavioral therapy for insomnia (CBT-I) outperformed pharmacological interventions in pooled RCT analyses. Peptides should complement behavioral strategies, not replace them.
Most practitioners first classify the insomnia type. For deep sleep deficits, the typical protocol is 0.2 mg CJC-1295/Ipamorelin subcutaneously at bedtime, five times weekly, at least two hours fasted. Cycles run three months on, one month off. Clinics report fewer nighttime awakenings within weeks 1-2, with deeper sleep by weeks 3-6.
Epitalon uses loading cycles of 10-20 days, once or twice yearly via subcutaneous injection. Some clinicians layer it on top of ongoing CJC-1295/Ipamorelin to reset circadian machinery while maintaining deep sleep architecture. Selank goes intranasally before bed for anxiety-predominant insomnia, with effects in 30-60 minutes.
Glycine is the common baseline. The 3g-before-bed protocol is cheap, safe, and targets the SCN thermal pathway independently from every hormonal intervention on this list.
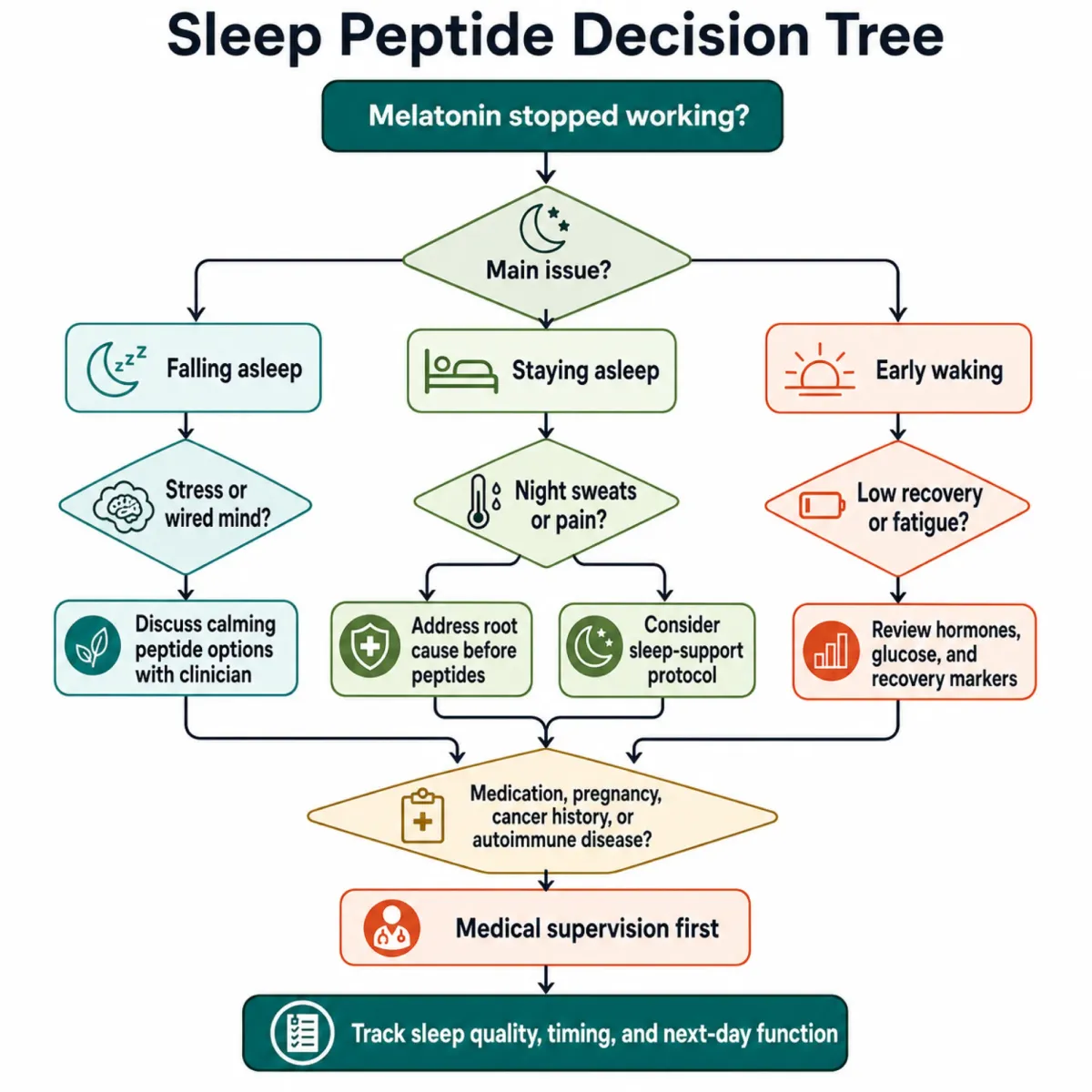
| Insomnia type | Primary approach | Supporting approach |
|---|---|---|
| Can't fall asleep (onset) | Glycine 3g + CBT-I | Selank if anxiety-driven |
| Can't stay asleep (maintenance) | CJC-1295/Ipamorelin at bedtime | Glycine 3g baseline |
| Hot flash wakeups | Address hormones first (HRT discussion) | Glycine for thermal regulation |
| Shifted circadian rhythm | Epitalon loading cycle | Low-dose melatonin (0.3-1 mg) timing |
| Anxiety-driven | Selank intranasal | Glycine 3g, Semax daytime |
Two universal cautions: source peptides from licensed compounding pharmacies, not gray-market suppliers. And CJC-1295/Ipamorelin is contraindicated for cancer survivors due to increased cellular replication.
The bottom line: glycine has the best evidence-to-cost ratio. GH secretagogues have strong mechanistic support but no sleep-specific RCTs. Selank addresses anxiety-driven insomnia without sedation, though sleep evidence is indirect. Epitalon has one real human circadian trial. DSIP has the weakest controlled data despite the promising name.
Frequently Asked Questions
Can I take sleep peptides alongside hormone replacement therapy?
No published data exists on peptide-HRT sleep interactions. Glycine poses minimal risk as a dietary amino acid. For CJC-1295/Ipamorelin or Selank, coordinate with a practitioner managing both protocols, since GH secretagogues affect hormonal axes that overlap with HRT.
How long do sleep peptides take to work?
Glycine can improve next-day alertness from the first dose. Clinical sources report CJC-1295/Ipamorelin effects within 1-2 weeks, with deeper sleep by weeks 3-6. Selank works within 30-60 minutes intranasally. Epitalon targets longer-term circadian reset over 10-20 day loading cycles.
Is it safe to combine multiple sleep peptides?
Some practitioners layer glycine, CJC-1295/Ipamorelin, and Selank since they target different mechanisms. No controlled trials have studied multi-peptide stacks. Start with one, assess over 4-6 weeks, and add sequentially. Glycine is the lowest-risk starting point.
Why not just increase my melatonin dose?
Studies found low doses of 0.3-1.0 mg are the most effective for sleep promotion. Higher doses cause grogginess and may desensitize receptors. If your insomnia stems from progesterone decline, cortisol, or hot flashes, melatonin at any dose addresses the wrong mechanism.
Are any of these peptides FDA-approved for sleep?
No. Glycine is a dietary supplement. DSIP is FDA Category 2 restricted. CJC-1295/Ipamorelin have uncertain regulatory status. Selank completed Phase 3 testing in Russia but lacks FDA approval. Epitalon has no U.S. regulatory pathway. All prescription peptides here are accessed through compounding pharmacies, not standard channels.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











