What your brain does all day
The brain does far more than generate thoughts. It runs breathing patterns while you sleep, helps you keep balance when you walk across a wet floor, tracks social cues in conversation, and updates your memory in the background while you focus on something else. If that sounds like a lot, it is. Your brain is a high-demand organ with limited downtime. Even at rest, it remains metabolically active and constantly coordinates body systems.
A good way to think about it: your brain is less like a single "thinking center" and more like a network manager. Different regions specialize, but they also work together in fast loops. The frontal regions help with planning and inhibition. Temporal regions help with language and memory. Subcortical circuits help automate movement and reward learning. Brainstem networks keep essential life functions online. When one area is strained, your performance in everyday tasks can drop even if the rest of your body feels fine.
This is one reason brain health should be treated as a daily maintenance issue, not something to worry about only in older age. Global public health data from the World Health Organization dementia fact sheet shows dementia affects tens of millions of people and remains a leading cause of disability and dependency in later life. The same report also notes that risk does not come from one single cause. Multiple medical, social, and lifestyle factors accumulate over time.
Recent evidence has sharpened that message. The updated Lancet dementia prevention commission emphasizes that a meaningful share of dementia risk may be linked to modifiable factors such as hearing loss, blood pressure, diabetes, smoking, inactivity, depression, and social isolation. In plain language: while no one can promise prevention, there is strong reason to act early on risks you can influence.
Quick takeaway: brain health is built in routines. Blood pressure checks, sleep consistency, movement, hearing care, and social connection matter more than most people think.
If you are looking for practical ways to start, this site already has focused guides on physical exercise for brain health and evidence-based memory improvement. In this guide, we zoom out and connect the full picture: anatomy, function, risk, early warning signs, and a step-by-step action plan.
Brain anatomy without jargon
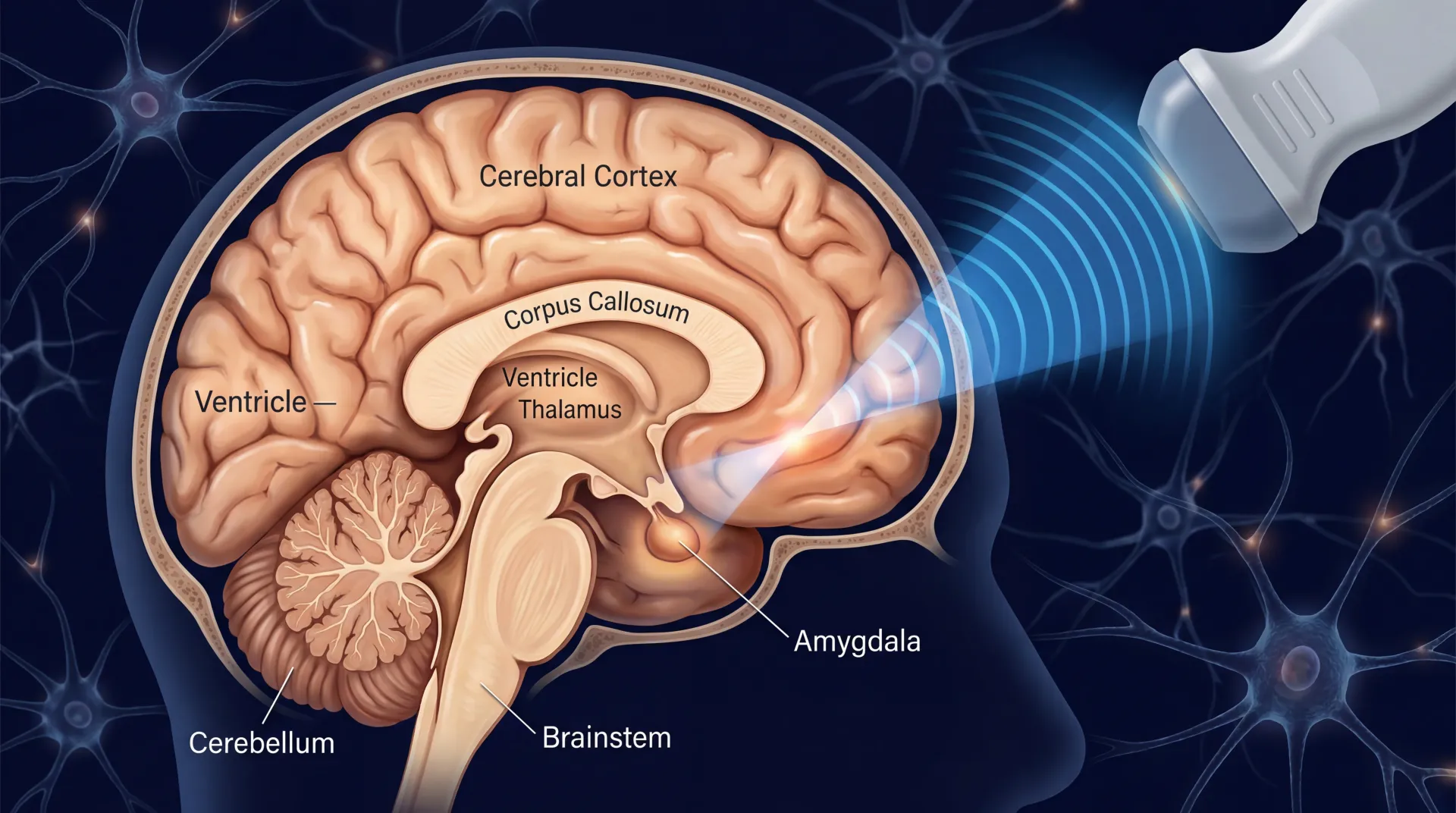
Most anatomy charts are dense and hard to use in real life. A simpler frame helps: the brain has cortical regions that handle higher-order processing, deep structures that regulate emotion and memory, and support systems that keep signals clean and reliable. None of these parts works in isolation. The value of anatomy is not memorizing labels. It is understanding which symptoms could map to which systems.
The NINDS brain basics resource is useful here because it explains regional function without overselling certainty. Different networks overlap, and many tasks use more than one pathway.
| Brain region | Core role | What changes may look like | Everyday support habit |
|---|---|---|---|
| Prefrontal cortex | Planning, impulse control, working memory | Disorganization, poor follow-through, increased impulsivity | Use written plans, reduce multitasking, protect sleep timing |
| Hippocampus | Forming and indexing new memories | Repeating questions, forgetting recent details | Daily recall practice, spaced learning, aerobic exercise |
| Basal ganglia | Habit loops, motor coordination, reward learning | Slowed movement, rigid routines, reduced initiation | Structured movement sessions and cue-based routines |
| Cerebellum | Balance, precision, motor timing | Clumsiness, poor coordination, gait instability | Balance drills, strength training, vision checks |
| Brainstem | Breathing, heart rate, arousal, autonomic control | Dizziness, severe swallowing or breathing changes | Urgent medical evaluation when sudden symptoms appear |
What this means in practice: if someone says "my memory is getting worse," the issue may involve sleep debt, medication effects, mood strain, vascular risk, hearing loss, or workload overload, not just one isolated memory center. The anatomy framework helps you ask better questions instead of jumping to worst-case conclusions.
The second useful concept is neuroplasticity. The brain does adapt, but adaptation is specific. Training one skill does not magically improve all cognitive domains. Improvement usually follows the demands you repeat most: aerobic challenge, focused attention, language use, social interaction, sleep repair, and stress regulation.
How the brain changes across life
Normal brain aging is real, but it is not the same as rapid decline. Processing speed may slow with age. Word retrieval may feel less instant under stress. Recovery from sleep loss may take longer. None of those alone confirms disease. The pattern that matters is trajectory: stable vs progressively worse, especially when changes interfere with daily function.
Large-scale evidence keeps pointing to cumulative risk. A network meta-analysis in Alzheimer's & Dementia (2024) found associations between modifiable domains and cognitive trajectories, with combinations of healthy behaviors showing stronger protective signals than single isolated changes. That aligns with what clinicians already see: stacking small wins tends to outperform searching for one miracle intervention.
Sleep is another major lever. A 2025 meta-analysis on sleep trajectories and cognitive outcomes reported that persistent poor sleep patterns were linked with higher risk of later cognitive decline, while maintaining healthier sleep trajectories was associated with lower risk over time (Sleep Medicine Reviews, 2025). This does not mean one bad week of sleep causes permanent harm. It means chronic, untreated sleep disruption is not benign.
Vascular risk control also matters. In SPRINT MIND follow-up reporting, NIH-funded investigators observed fewer cases of mild cognitive impairment in participants randomized to intensive blood pressure control compared with standard targets. The lesson is straightforward: what protects blood vessels often protects cognitive function too.
Hearing and cognition have moved from theory to stronger trial evidence. The ACHIEVE trial, published in The Lancet (2023), showed that hearing intervention in older adults at elevated risk was associated with slower cognitive decline in a high-risk subgroup. Hearing is not a small quality-of-life detail. It can influence cognitive load, social engagement, and long-term brain outcomes.
| Life stage | Common pressure points | High-yield action | Why it helps |
|---|---|---|---|
| 20s-30s | Sleep debt, stress load, high alcohol intake, inconsistent routines | Lock a sleep window and train 150+ minutes weekly | Builds cognitive reserve and metabolic resilience early |
| 40s-50s | Blood pressure drift, insulin resistance, chronic overload | Track BP, waist, and fasting labs with regular follow-up | Reduces long-run vascular strain linked to cognitive decline |
| 60s+ | Hearing loss, social isolation, polypharmacy, inactivity | Address hearing early and preserve social + physical routines | Lowers cognitive load and supports engagement networks |
If you have been postponing sleep work, start with the fundamentals in this sleep improvement guide. If you have suspected chronic stress is affecting concentration, you can pair it with practical breathing routines from these stress-relief breathing techniques.
Daily habits that protect cognition
When people ask "What is the best brain supplement?" they usually want one quick answer. The more useful answer is a system: movement, sleep, blood pressure control, diet quality, hearing care, social engagement, and mental challenge. Supplements can play a minor role in specific deficiencies, but they do not replace fundamentals. If you are exploring that area, read the context first in our guide to natural brain-supportive nutrition strategies.
Exercise has some of the strongest evidence for broad cognitive support. A 2024 systematic review and meta-analysis found that physical activity interventions were associated with reduced cognitive decline risk in older adults, especially when programs were sustained over time (PubMed 38300618). The key is consistency, not intensity spikes.
Diet quality also appears to influence cognitive trajectories. In the previously noted 2024 evidence synthesis (PubMed 41584749), patterns rich in whole foods and lower in ultra-processed load were associated with better long-term cognitive outcomes compared with low-quality baseline eating patterns.

Stress management belongs in this conversation too. Chronic, unmanaged stress can worsen sleep, raise blood pressure, shift eating behavior, and narrow attention. That combination can compound cognitive strain. Evidence for mind-body tools is mixed by method and population, but structured mindfulness and meditation programs have shown benefits for stress symptoms and mood in many groups, summarized by the NCCIH meditation overview.
Sleep is where most plans collapse. People optimize food and workouts but still run a rotating bedtime. If you do one thing this month, set a stable wake time every day. A regular wake anchor often improves sleep drive more effectively than chasing perfect bedtime conditions. The NHLBI sleep deprivation resource is a solid reminder that chronic short sleep affects mood, performance, metabolism, and cardiovascular risk, all of which feed back into cognitive function.
| Habit domain | Practical weekly target | Evidence signal | How to monitor |
|---|---|---|---|
| Aerobic movement | 150-300 minutes moderate activity + 2 strength sessions | Strong and repeated across meta-analyses | Calendar completion rate, resting heart rate trend |
| Sleep consistency | 7-9 hours with fixed wake time | Moderate to strong for long-run cognitive risk | Weekly sleep midpoint variability |
| Blood pressure care | Home BP checks and clinician-guided targets | Strong vascular-cognitive linkage | Average home BP log over 2-4 weeks |
| Nutrition quality | Mostly minimally processed foods, adequate protein and fiber | Moderate, stronger when combined with activity and sleep | Meal pattern adherence, waist and lab trend |
| Social engagement | At least 2 meaningful social contacts weekly | Moderate, linked with lower isolation risk | Scheduled contacts completed each week |
| Hearing and sensory care | Prompt hearing checks when communication strain appears | Moderate to strong in high-risk older adults | Hearing follow-up completion |
Notice the pattern: these are ordinary habits, but they are not optional. They shape vascular function, inflammation burden, metabolic control, and cognitive load. Your brain responds to all of that.
Warning signs and medical conditions
Not every headache is an emergency. Not every memory slip is a neurodegenerative disease. But some symptoms need rapid evaluation. The key is to differentiate nuisance symptoms from red-flag patterns. When in doubt, urgency is safer than waiting.
Stroke-like symptoms are always urgent. Sudden one-sided weakness, facial droop, slurred speech, severe confusion, or abrupt vision loss should trigger emergency care. Time-sensitive treatment can reduce long-term disability. Repeated head injuries are another high-risk category. The CDC traumatic brain injury prevention page outlines avoidable risk factors and prevention basics for work, sport, home, and driving contexts.
Beyond emergencies, watch for slower patterns: progressive decline in complex tasks, repeated missed payments, getting lost in familiar places, new personality changes, or social withdrawal tied to cognitive strain. These changes deserve structured assessment rather than self-diagnosis.
| Symptom pattern | Possible concern | Recommended action window | Why timing matters |
|---|---|---|---|
| Sudden weakness, speech change, facial droop | Stroke or TIA | Immediate emergency response | Early intervention can preserve function |
| Sudden severe "worst headache" with neuro signs | Possible hemorrhage or vascular event | Immediate emergency response | Delay can raise mortality and disability risk |
| Persistent post-concussion symptoms | TBI recovery complication | Prompt clinical follow-up within days | Guided rehab improves return-to-function planning |
| Gradual memory + executive decline over months | MCI, mood disorder, medication effect, sleep disorder, or neurodegenerative disease | Comprehensive outpatient evaluation within weeks | Early clarification improves treatment options and planning |
| Hearing withdrawal plus cognitive complaints | Increased cognitive load and social isolation risk | Hearing assessment and cognitive screening | Treatable hearing issues can reduce daily strain |
Common medical conditions tied to brain outcomes include hypertension, diabetes, sleep apnea, depression, high alcohol burden, and repetitive head trauma. None of these guarantees severe decline. But unmanaged combinations raise risk substantially. The goal is to treat what is treatable now, before functional losses become harder to reverse.
Myth vs fact: brain health
Confusion around brain health usually comes from half-true claims. This section is designed to make decisions easier.
| Myth | What evidence suggests | Better decision |
|---|---|---|
| "A single supplement can protect my brain." | Single-product evidence is usually limited or context-specific. | Build fundamentals first: sleep, activity, BP control, hearing, diet. |
| "Brain decline is just aging, nothing to do." | Multiple modifiable factors are associated with risk trajectories. | Treat risk factors early and consistently. |
| "If I forget names sometimes, I must have dementia." | Occasional lapses can be normal; progressive functional loss is different. | Track pattern, duration, and functional impact before panicking. |
| "I can catch up on sleep on weekends forever." | Irregular long-term sleep patterns are linked with poorer outcomes. | Prioritize consistent sleep timing throughout the week. |
| "Mental games alone are enough." | Cognitive challenge helps, but vascular and lifestyle factors remain central. | Use mental training as one part of a broader plan. |

The reason myths persist is simple: quick fixes are easier to market than behavior systems. But systems are what hold up under stress, travel, busy weeks, and life transitions.
A practical 30-day brain health plan
You do not need a perfect month. You need a repeatable month. Start where friction is lowest, then stack additional habits.

| Week | Primary focus | Daily minimum | Completion marker |
|---|---|---|---|
| Week 1 | Sleep anchor + morning light | Fixed wake time, 10-20 minutes outdoor light, caffeine cutoff | 5 of 7 days completed |
| Week 2 | Movement baseline | 30 minutes brisk walking or equivalent, plus 2 strength sessions this week | 150+ weekly movement minutes |
| Week 3 | Vascular and nutrition reset | Home BP log, protein-forward meals, fiber at each main meal | BP log complete + meal adherence at 70%+ |
| Week 4 | Cognitive load and social protection | One focused learning block, one social call/meetup, one stress-downshift practice | At least 4 focused blocks and 2 social contacts |
If you miss two days, do not reset the whole plan. Continue from the next block. Brain-health routines fail when people treat small misses as total failure. Consistency beats intensity.
Consider discussing this checklist with your clinician if you have diabetes, hypertension, sleep apnea, depression, repeated concussion history, or current cognitive symptoms. Personal medical context changes priorities.
Frequently Asked Questions
Can you really reduce dementia risk, or is it mostly genetics?
Both matter. Genetics can raise baseline vulnerability, but large population evidence suggests that modifiable factors still influence risk trajectories. You cannot control your genes, but you can control sleep, blood pressure care, physical activity, diabetes management, hearing follow-up, smoking exposure, and social engagement.
How much exercise is enough for brain health?
A practical evidence-aligned baseline is 150 to 300 minutes of moderate aerobic activity each week plus resistance training at least twice weekly. If you are currently inactive, start smaller and progress. Consistency over months matters more than short bursts of extreme intensity.
Do brain-training apps prevent cognitive decline?
They may improve performance on trained tasks, but they should not be treated as a standalone prevention strategy. The strongest support still points to combined lifestyle and vascular risk management. Use cognitive apps as a supplement, not the foundation.
When should memory problems be evaluated by a professional?
Seek evaluation when changes are progressive, interfere with daily tasks, or are noticed by family and coworkers. Also seek prompt care after head injury with persistent symptoms, sudden confusion, or any stroke-like signs. Early assessment improves options and planning.
Related Articles
- Physical Exercise for Brain Health: Ultimate Guide - A deeper protocol for aerobic, strength, and coordination training that supports cognition.
- Best Ways to Seriously Improve Your Memory - Practical memory systems you can apply at work and at home.
- Best Ways to Improve Your Sleep - Sleep architecture, routine design, and troubleshooting for better recovery.
- Nootropics for the Mental Edge - Evidence-based review of common nootropics, expected effects, and safety limits.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.