
For about 60 years, nobody cared much about Zika virus. It was a footnote in tropical medicine textbooks, a mild illness that caused a rash and some joint pain and then went away. Then, in the span of about 18 months, it went from medical curiosity to global emergency, leaving thousands of families with children who would need lifelong care. The WHO declared it a Public Health Emergency of International Concern in February 2016. And despite what the quiet headlines since then might suggest, Zika hasn't gone away.
How a Forest Virus Became a Global Emergency
Scientists first isolated Zika from a rhesus monkey in Uganda's Zika Forest in 1947. For decades after that, it barely registered. Sporadic human infections turned up in Africa and Southeast Asia through the 1960s and '70s, but the illness looked mild, self-limiting, and frankly boring from a research funding perspective.
The first real outbreak hit Yap Island in Micronesia in 2007, infecting an estimated 73% of the population over age three. Even then, the worst anyone experienced was a rash, some joint pain, and low fever. In 2013, French Polynesia saw a much bigger wave, roughly 30,000 cases. Doctors there noticed an unsettling pattern: a sudden spike in Guillain-Barré syndrome, a rare condition where the immune system attacks the peripheral nerves.
Then Zika reached Brazil in late 2014, and everything changed. Cases exploded across the Americas. Doctors in northeastern Brazil started seeing something they'd never encountered at this scale: baby after baby born with abnormally small heads. Between late 2014 and early 2016, affected Brazilian regions reported roughly 20 times more microcephaly cases than the previous five years combined.
On February 1, 2016, the WHO declared Zika-linked microcephaly and neurological disorders a Public Health Emergency of International Concern. The virus had already reached more than 60 countries.
Every Way Zika Spreads
Zika doesn't just travel by mosquito. That was one of the surprises during the 2015-2016 outbreak. The virus has at least five documented routes, and a couple of them caught researchers off guard.
| Transmission Route | How It Works | Key Detail |
|---|---|---|
| Mosquito bite | Aedes aegypti (primary) and Aedes albopictus carry the virus | Mosquitoes bite during the day but can also bite at night |
| Sexual contact | Vaginal, anal, and oral sex, even from people with no symptoms | Viral RNA detected in semen up to 188 days after symptom onset |
| Mother to fetus | Virus crosses the placental barrier during pregnancy | Highest birth defect risk during first trimester (~8%) |
| Blood transfusion | Confirmed via platelet transfusions in Brazil | No confirmed cases in the U.S.; screening protocols now in place |
| Laboratory exposure | Needle-stick injuries | Rare; standard biosafety protocols apply |
Aedes aegypti mosquitoes do the heavy lifting. They thrive in cities, breed in tiny pools of standing water (a bottle cap is enough for hundreds of eggs), and bite aggressively during early morning and late afternoon. That urban lifestyle is exactly why Zika spread so fast through densely populated areas in the Americas.
Sexual transmission was the real curveball. The CDC reports Zika RNA persists in semen far longer than in blood, which means someone can test negative on a blood draw and still carry infectious virus in their reproductive system. Both symptomatic and asymptomatic people can pass it to partners.
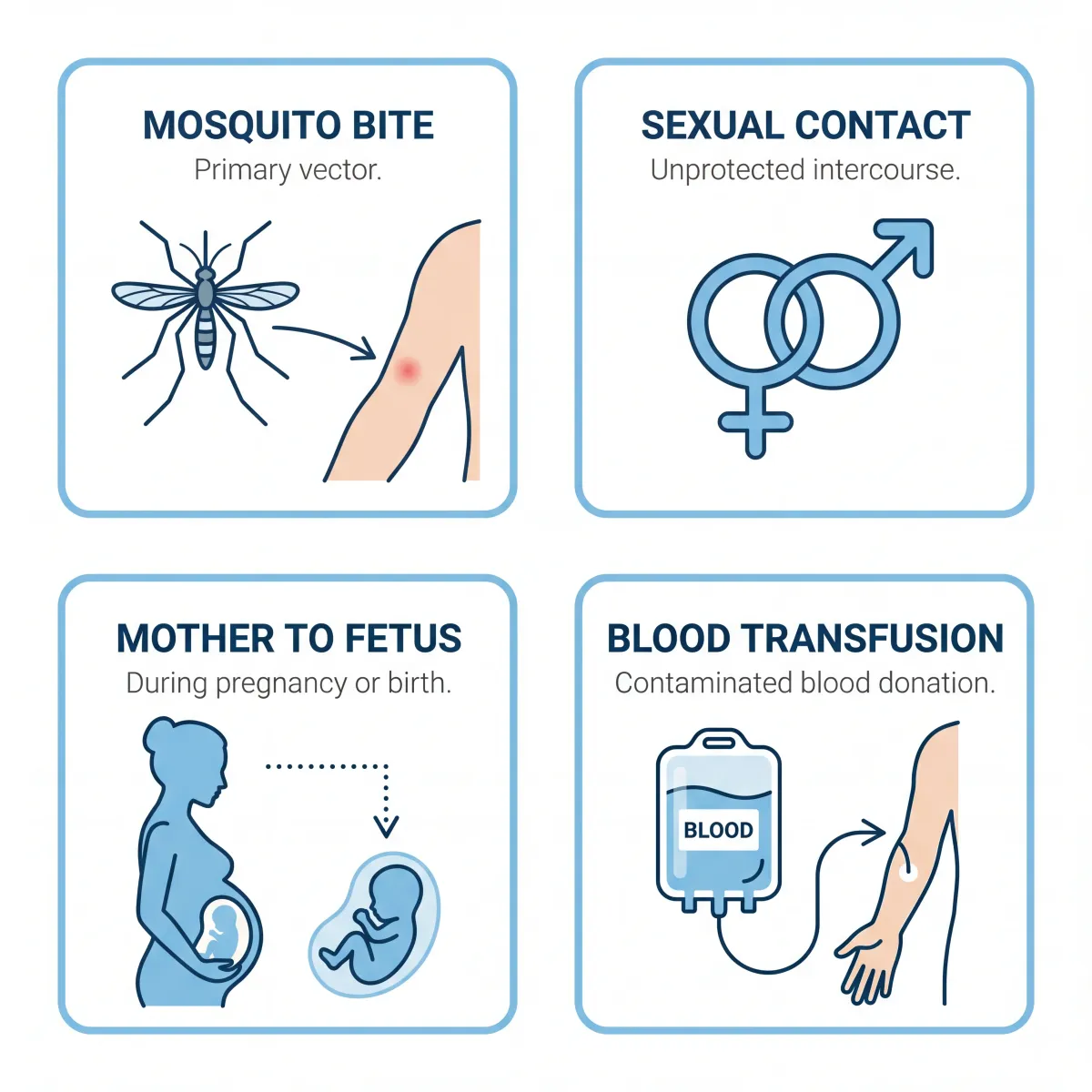
The route that does the most damage, though, is vertical transmission from mother to fetus. The virus crosses the placenta during any trimester, but first-trimester infections carry the highest risk of severe brain damage. Transmission around the time of delivery is also documented.
One thing Zika does not do: spread through kissing, breastfeeding, coughing, sneezing, or casual contact. The WHO actually encourages mothers in affected areas to keep breastfeeding. For a broader look at the virus itself, see our guide to everything you need to know about Zika virus.
When Zika Reaches the Womb: Birth Defects and Beyond
Congenital Zika Syndrome is what doctors call the cluster of birth defects caused by Zika infection during pregnancy. The CDC defines it by five features: severe microcephaly with a partially collapsed skull, decreased brain tissue with specific damage patterns, damage to the back of the eye, restricted joint movement, and excessive muscle tone that limits movement after birth. Seizures, hearing loss, and feeding problems are common too.
| Trimester of Infection | Birth Defect Rate | Primary Risks |
|---|---|---|
| First trimester | ~8% | Severe microcephaly, brain calcifications |
| Second trimester | ~6% | Brain abnormalities, eye damage |
| Third trimester | ~3.8% | Milder brain changes, growth restrictions |
| Overall (any trimester) | ~5% | Full range of congenital Zika syndrome |
Those percentages come from the CDC's U.S. Zika Pregnancy and Infant Registry. Worth noting: mothers who never showed symptoms still had a 4.2% birth defect rate, almost as high as the 5.3% rate among symptomatic mothers. You didn't have to know you were infected for the virus to cause damage.
The mortality numbers are hard to read. A nationwide Brazilian cohort study in the New England Journal of Medicine found children with CZS died at a rate of 52.6 per 1,000 person-years, versus 5.6 per 1,000 in unaffected kids. A January 2025 study in JAMA Network Open put it another way: children under five with CZS had a 13.1-fold higher risk of death. Respiratory diseases, infections, and nervous system conditions were the top killers.
Zika also targets the nervous system in adults. During outbreaks, Guillain-Barré syndrome incidence rose 2 to 9.8 times above baseline. A case-control study from French Polynesia, published in The Lancet, estimated GBS at 0.24 per 1,000 Zika infections. That study was the first to definitively link the virus to GBS.
If you're unsure what to watch for, we cover early Zika symptoms and how to get tested in a separate guide.
92 Countries and Counting: Where Zika Stands Now
The 2016 emergency faded from the news cycle, but the virus didn't go with it. As of mid-2024, the WHO documents mosquito-borne Zika transmission in 92 countries and territories.

| Region / Country | Recent Cases | Notes |
|---|---|---|
| Americas (total) | 16,000+ confirmed (2024) | Brazil accounts for the vast majority |
| Brazil | 13,785 cases, 4 deaths (2024) | 3,678 cases in first 4 weeks of 2025 |
| United States | 19 cases (2024) | All travel-related; no local transmission since 2018 |
| Thailand | 446 cases (2024) | 127 cases in early 2025 |
| India | 151 cases across 3 states (2024) | WHO outbreak notification issued in 2025 |
| U.S. peak (comparison) | 5,000+ cases (2016) | Included local mosquito-borne transmission |
The Pan American Health Organization tracks active transmission across the Americas, and Brazil keeps reporting the highest numbers. Early 2025 data showed 3,678 cases in just the first four epidemiological weeks, which doesn't suggest the virus is winding down.
Asia has its own situation. Thailand confirmed 446 cases in 2024 with another 127 in early 2025. India reported 151 cases across three states, enough to trigger a WHO outbreak notification. In the U.S., all 19 cases in 2024 came from travelers returning from affected areas. No mosquito-borne transmission has happened on the U.S. mainland since 2018.
Fewer cases doesn't mean less risk. The Aedes mosquitoes that carry Zika keep expanding their range, and there's still no licensed vaccine to fall back on.
Myth vs. Fact: What the Science Actually Shows
Misinformation about Zika spread almost as fast as the virus during the 2016 outbreak. Conspiracy theories blamed everything from genetically modified mosquitoes to pesticides to childhood vaccines for the surge in microcephaly. None of it held up.
| Myth | Fact |
|---|---|
| GMO mosquitoes caused the Zika outbreak | No evidence supports this. Genetically modified mosquitoes are designed to reduce Aedes populations, not spread disease. |
| The pesticide pyriproxyfen causes microcephaly, not Zika | Pyriproxyfen disrupts insect hormone pathways through a mechanism that doesn't exist in human fetal development. It also has poor absorption in humans. |
| Only pregnant women need to worry about Zika | Adults of any age can develop Guillain-Barré syndrome and other neurological complications from Zika infection. |
| Zika spreads through kissing and casual contact | Zika RNA has been found in saliva, but the WHO says there is no evidence of transmission through kissing, breastfeeding, or casual contact. |
| Zika is no longer a threat because cases dropped | The virus is still circulating in 92 countries. The Americas reported 16,000+ cases in 2024. No vaccine exists. |
| Breastfeeding transmits Zika to babies | Zika RNA has been found in breast milk, but no confirmed cases of breastfeeding transmission exist. Both WHO and CDC recommend continuing breastfeeding. |
The most dangerous misconception might be the last one on that list: that Zika went away. It didn't. The drop in cases actually created a new problem, which leads to the vaccine situation.
The Race for a Zika Vaccine
After more than a decade of research, no licensed Zika vaccine exists. Not in the U.S., not in Brazil, not anywhere. As of early 2026, 16 vaccine candidates sit in Phase 1 or Phase 2 trials, plus three monoclonal antibody candidates in Phase 1.
The most advanced work spans three platforms. The National Institute of Allergy and Infectious Diseases developed DNA vaccines (VRC5283 and VRC5288) that encode Zika structural proteins and entered a Phase 2/2b trial with over 2,490 planned participants. Moderna's mRNA candidate, mRNA-1893, looked good in animal studies and Phase 1, then moved to Phase 2 with about 800 adults. Valneva's inactivated vaccine (VLA1601) started an additional Phase 1 trial in March 2024, with initial results posted last November.
All three programs ran into the same wall: not enough Zika cases to prove the vaccines work. You can't demonstrate that a vaccine prevents infection when barely anyone in the trial group encounters the virus. None of the Phase 2 trials were completed as planned.
It's a genuinely frustrating catch-22. The decline in cases that ended the immediate emergency also killed the clinical trials designed to prevent the next one. Researchers writing in The Lancet Infectious Diseases have pushed for creative workarounds like human challenge studies and adaptive trial designs, but nothing has broken through yet.
This kind of development stall isn't unique to Zika. Lyme disease faces similar diagnostic and treatment challenges as another vector-borne illness.
Your Complete Prevention Toolkit
No vaccine means prevention is everything. The CDC and WHO both recommend a layered approach that addresses mosquitoes, sex, and travel separately.
For mosquito bites: use EPA-registered repellents with DEET, picaridin, oil of lemon eucalyptus, IR3535, or icaridin. Wear long sleeves and long pants outdoors. Treat clothing with permethrin. Stay in screened or air-conditioned rooms when you can, and use insecticide-treated bed nets at night.

Around your home, get rid of standing water. Flower pots, pet dishes, old tires, clogged gutters: empty and scrub anything that holds water at least once a week. Aedes mosquitoes don't need much to breed.
If you're coming back from a Zika-risk area, keep up mosquito prevention for three weeks after you return, even if you feel perfectly fine. This isn't about protecting yourself at that point; it's about making sure a local mosquito doesn't bite you and start a new transmission chain.
For sexual transmission: the CDC says men should use condoms or abstain for at least three months after potential Zika exposure, women for at least two months. The difference reflects how much longer the virus hangs around in semen.
If you're pregnant or planning to become pregnant, the guidance is straightforward: consider postponing travel to areas with active Zika transmission. If travel is unavoidable, follow strict mosquito prevention and talk to your doctor about testing before and after the trip.
General immune health matters as a baseline, too. We have a separate guide on natural ways to strengthen your immune system.
Recognizing Symptoms and Getting Tested
Here's what makes Zika so tricky to track: roughly 80% of infected people never develop symptoms. When symptoms do show up, they're mild. Low-grade fever, rash, joint pain (hands and feet especially), red eyes, muscle aches, headache. They appear 3 to 14 days after a bite and clear up within a week.
Testing combines two approaches. Nucleic acid amplification testing (NAAT/RT-PCR) detects viral RNA directly, and it works best on serum drawn within seven days of symptoms or urine within 14 days. IgM antibody testing picks up the immune response starting in the first week, but it cross-reacts with other flaviviruses like dengue and West Nile, which muddies the picture. A plaque reduction neutralization test (PRNT) can sort out ambiguous results, but it's not simple or fast.
Treatment? There isn't one. Rest, fluids, and acetaminophen for pain and fever. The CDC specifically warns against aspirin and other NSAIDs until dengue is ruled out, because of bleeding risk. If you develop progressive weakness or tingling in your arms and legs, that could signal Guillain-Barré syndrome and needs immediate medical attention.
What Lasts After the Virus Clears
The acute infection clears in about a week. The consequences, for some people, don't.
Children born with congenital Zika syndrome face a lifetime of challenges: difficulty swallowing, seizures, repeated hospitalizations for pneumonia and UTIs. The JAMA Network Open study from January 2025 broke down cause-specific mortality: 30 times higher for respiratory diseases, 28 times higher for infections, 57 times higher for nervous system conditions, all compared to unaffected children.
But here's something that doesn't get enough attention: even children born looking completely normal after in utero Zika exposure may have problems that emerge later. A February 2025 study in Pediatrics found a nearly threefold increase in adverse developmental outcomes, with higher rates of motor and cognitive delays, especially when the infection happened in the first trimester. A Colombian study tracking kids to age five and six found emerging differences in executive function, behavior, and mobility.
Then there's the immune system angle. Research in The Lancet eBioMedicine (2024) found that Zika-exposed infants, even clinically normal ones, showed elevated inflammation markers, skewed immune responses, and weaker reactions to routine childhood vaccines like DTaP. These kids might be more vulnerable to infections throughout childhood, though the research is still catching up to that question.
For adults, Guillain-Barré syndrome is the main long-term worry. Some patients recover fully within months. Others deal with lingering weakness and fatigue for years. Dietary support for immune health can be part of the recovery picture. Our guide to probiotic-rich foods and immune function covers the basics.
Frequently Asked Questions
Can you catch Zika from a mosquito in the United States?
No locally acquired mosquito-borne Zika cases have occurred in the continental U.S. since 2018. Every recent U.S. case has been travel-related. That said, Aedes mosquitoes capable of carrying Zika are present in southern states, so the theoretical risk of local transmission hasn't disappeared entirely.
Is it safe to travel to countries where Zika is circulating?
For most travelers, the risk of serious complications is low. The big exception: anyone who is pregnant or actively trying to conceive should consult their healthcare provider and seriously consider postponing travel to affected areas. All travelers should use insect repellent and mosquito prevention measures consistently.
How long after Zika infection should couples wait before trying to conceive?
The CDC recommends men wait at least three months and women wait at least two months after symptom onset or last possible exposure. The gap accounts for how long the virus persists in semen versus blood.
Does having Zika once make you immune to future infections?
Current evidence suggests a single infection probably produces lasting immunity, similar to other flaviviruses. One complication: prior Zika infection may affect how your body responds to a later dengue infection through cross-reactive antibodies. Researchers are still working out exactly what that means clinically.
Can Zika be passed through breast milk?
Zika RNA has been detected in breast milk, but no confirmed cases of transmission through breastfeeding have been documented. Both the WHO and CDC recommend mothers continue breastfeeding even in areas with active transmission. The benefits of breastfeeding outweigh the theoretical risk.
Related Articles
- All You Need to Know About Zika Virus — A broader primer on the virus, its biology, and why it matters for public health.
- Zika Virus Symptoms and Early Diagnosis — What to look for and how to get tested if you think you've been exposed.
- Lyme Disease Facts and Symptoms: How to Spot the Signs — Another vector-borne disease with its own set of diagnostic challenges.
- Natural Ways to Strengthen Your Immune System — Practical strategies for supporting immune function year-round.
- Immune-Boosting Probiotic Foods — How fermented foods and probiotics support your body's defenses.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











