
A Hungarian scientist tried to give mice cancer and accidentally grew their fur back
Red light therapy has one of the stranger origin stories in medicine. In the 1960s, Hungarian scientist Endre Mester set out to test whether low-level red light exposure would cause skin cancer in mice. It didn't. The mice grew thicker fur than their unexposed counterparts. That accidental finding launched six decades of research into what we now call photobiomodulation -- the use of specific light wavelengths to trigger biological changes in tissue.
The mechanism: your cells contain mitochondria, the organelles that produce adenosine triphosphate (ATP), the energy currency powering nearly every cellular process. One enzyme in the mitochondrial respiratory chain -- cytochrome c oxidase -- absorbs red and near-infrared light in the 600-1100 nanometer range. Think of cytochrome c oxidase as a revolving door that gets stuck when nitric oxide molecules wedge themselves into it. Red light photons knock those nitric oxide molecules loose, letting oxygen flow through instead. The result is a measurable increase in ATP production, which gives cells more energy to repair, regenerate, and do their normal jobs faster.
That ATP boost triggers downstream effects. Cells ramp up collagen and elastin production. Fibroblast activity increases. Blood vessels dilate, improving circulation to treated areas. Dr. Zakia Rahman, clinical professor of dermatology at Stanford, suspects this vasodilation is the mechanism behind several of red light's documented effects -- the widening of blood vessels enables more blood and nutrients to reach tissue, whether that's hair follicles on the scalp or collagen-producing cells in the dermis.
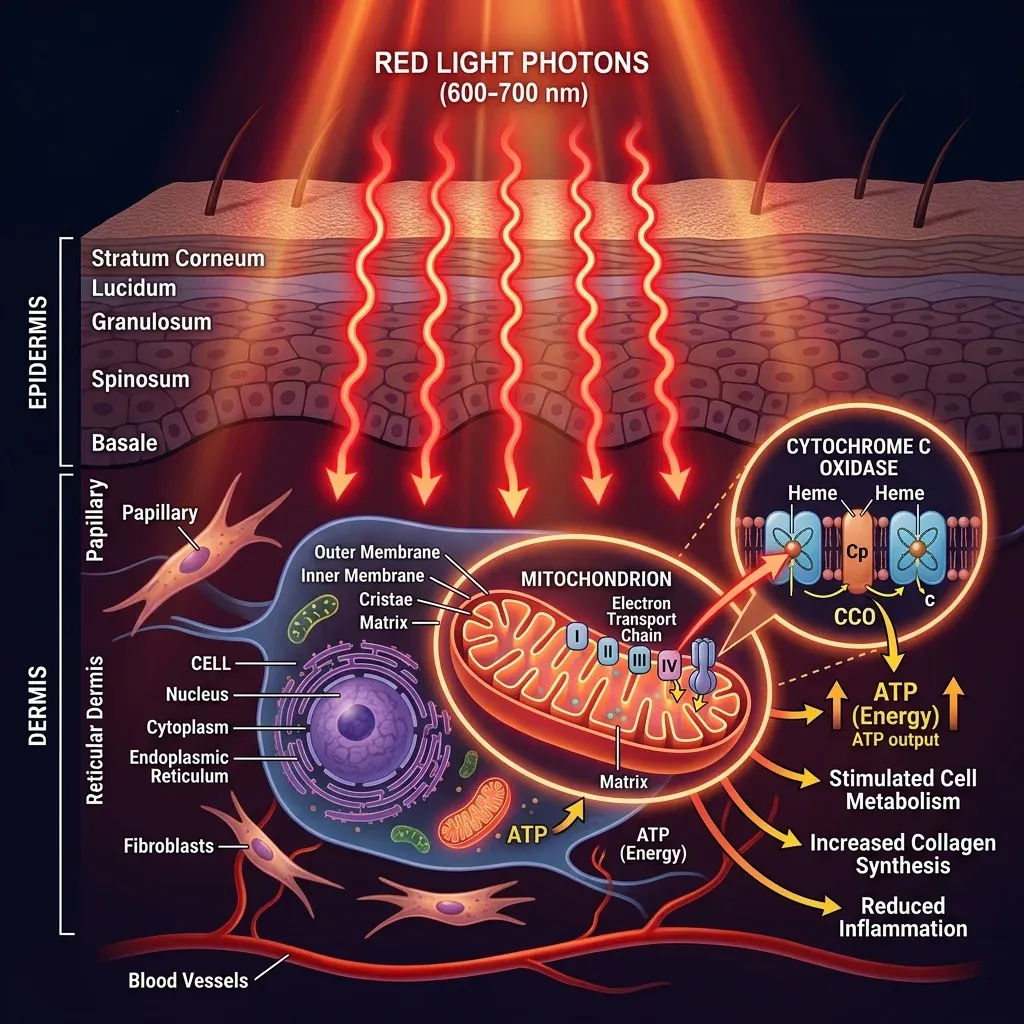
Not all light penetrates equally. Red light in the 600-700 nm range reaches the dermis -- the layer just below the skin surface where collagen and blood vessels live. Near-infrared light, from roughly 700 to 1100 nm, goes deeper into muscle and joint tissue. Different wavelengths get marketed for different purposes: shorter wavelengths for skin concerns, longer ones for pain and inflammation. The science behind wavelength-specific targeting is real, based on a principle called selective photothermolysis. But the dose has to be right.
Researchers describe a biphasic dose response, sometimes called the Arndt-Schulz law. Too little energy and nothing happens because the minimum threshold hasn't been reached. The right amount stimulates beneficial cellular responses. Too much energy and the stimulation reverses into inhibition -- the cells perform worse. "More is better" doesn't apply here, and the dosing question remains one of the field's biggest unresolved problems.
84 million Google results for "FDA approved red light therapy" -- and almost all of them are wrong
One of the most widespread misunderstandings in the red light therapy space involves three words: FDA approved. The FDA does not approve medical devices like red light therapy panels. It clears them. As the American Academy of Dermatology explains, "FDA cleared" means the agency considers the device to pose a low risk to the public. Terms like "FDA approved" or "FDA certified" have no legal meaning when applied to medical devices.
What has the FDA cleared red light devices for? Two categories: treating signs of skin aging and hair regrowth. FDA clearance tells you the device probably won't hurt you. It tells you nothing about whether it will deliver the results you're hoping for. Dr. Rahman at Stanford put it plainly: FDA clearance for these devices focuses mainly on safety.
FDA clearance tells you a device is safe. It does not tell you it works for the specific claim on the marketing copy.
One area where red light therapy has earned clinical recognition beyond the FDA's device clearance process: photobiomodulation is now included in treatment guidelines for oral mucositis -- painful mouth sores caused by cancer chemotherapy -- approved by both the UK's National Institute for Health and Care Excellence (NICE) and the Multinational Association of Supportive Cancer Care (MASCC). Red light is also used in photodynamic therapy, where it activates a topical drug to destroy precancerous and early-stage skin cancer cells. Cleveland Clinic notes this application has been medically accepted for years.
When you see a product claiming it's "FDA approved for anti-aging, pain relief, muscle recovery, and cognitive enhancement," the claim is overstated. The regulatory picture is narrow: safety-cleared for skin and hair, guideline-approved for oral mucositis in cancer patients, and established in photodynamic therapy. Everything else is off-label or unregulated territory.
The $200 mask vs the $80-per-session clinic: what you get
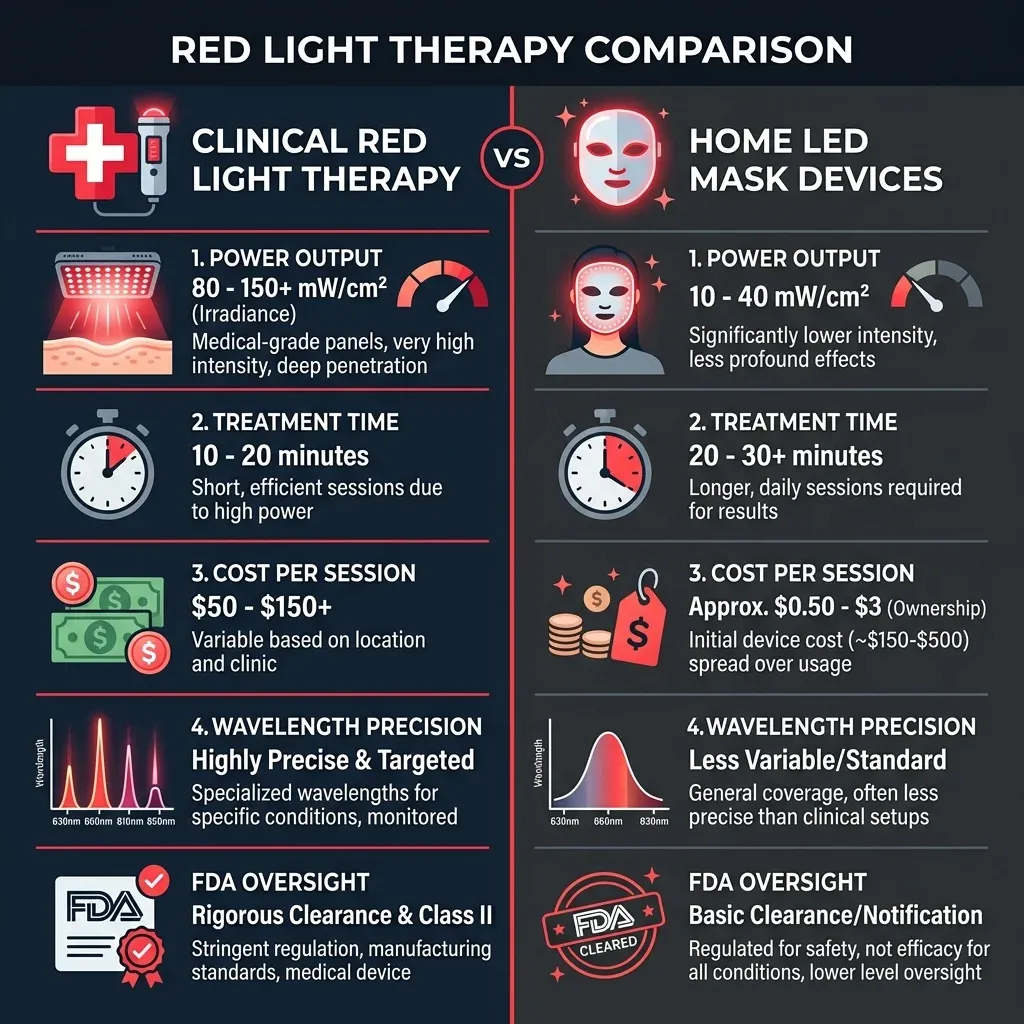
Walk into a dermatologist's office for red light therapy and you'll sit under a panel or bed delivering precisely calibrated wavelengths at power densities that home devices can't match. Buy a $200 LED mask on Amazon and you're getting a fraction of that output. Three separate sources -- Stanford Medicine, Cleveland Clinic, and the American Academy of Dermatology -- all make the same point: clinical devices are more powerful than home devices and produce better results.
Dr. Rachel Reynolds at Harvard-affiliated Beth Israel Deaconess Medical Center explains the practical difference. Professional devices "are likely to have the ability to better control the dose and provide a greater range of doses that can be calibrated to suit whatever condition is being treated." Home devices vary wildly in output. Dr. Rahman at Stanford adds that the strength and duration of treatment is "largely unknown when people buy tools for use at home."
| Factor | Clinical devices | Home devices |
|---|---|---|
| Power density | Higher (calibrated per treatment) | Lower (fixed output) |
| Wavelength precision | Exact nm controlled | Varies by manufacturer |
| Cost per session | $80+ per visit | $0 after purchase ($100-$1,000+ upfront) |
| Dose control | Adjusted by clinician | Fixed timer, user-dependent |
| Supervision | Medical professional present | Self-administered |
| Treatment frequency | 1-3x/week, clinician-guided | Multiple times/week for 4-6 months |
One clinical study using a high-end LED mask (the Dior x Lucibel, emitting 630 nm at 15.6 J/cm2) tested 20 volunteers who used it for 12 minutes, twice a week for three months. All participants reported visible improvement in skin quality, and the effects persisted for a month after they stopped. Worth noting: this was a high-end device delivering energy density at the upper range of what home devices offer, with a protocol designed by researchers. A random mask from an Instagram ad operating at unknown power density with unclear wavelength specifications is a different proposition.
Dr. Reynolds' advice for anyone going the home route: "For the devices to be effective, they must be used multiple times a week for four to six months. It's slow and steady. It's not going to be anyone's quick fix." The commitment gap is real. Most people who buy a red light mask use it enthusiastically for two weeks and then it lives in a drawer. If you're not prepared for months of consistent use, the investment probably isn't worth it regardless of the device quality.
The conditions where research holds up
A 2025 umbrella review -- the most comprehensive analysis published to date -- synthesized 15 meta-analyses covering 204 randomized controlled trials and more than 9,000 participants. The researchers assessed evidence certainty using the GRADE framework, which is the standard for evaluating how much confidence you should place in a finding. The conditions with moderate certainty of evidence supporting photobiomodulation:
| Condition | Effect size (eSMD) | Evidence certainty |
|---|---|---|
| Androgenetic alopecia (hair density) | 1.32 | Moderate |
| Fibromyalgia (fatigue reduction) | 1.25 | Moderate |
| Burning mouth syndrome (pain) | -0.92 | Moderate |
| Knee osteoarthritis (disability) | 0.65 | Moderate |
| Cognitive function | 0.49 | Moderate |
Hair regrowth is the most consistently supported application. The AAD reports that in large randomized controlled trials, red light therapy led to increased hair thickness, length, and density in people with androgenetic alopecia. One study found low-level laser therapy was as effective as minoxidil for regrowing hair, with the best results in patients who received both treatments together. The AAD's assessment: red light "offers a safe, non-invasive, and potentially effective treatment" for hereditary hair loss. The caveat from Dr. Rahman at Stanford: the effects stop when you stop treatment, and it won't revive dead follicles -- if you're fully bald in an area, red light won't bring those follicles back.

Skin rejuvenation has decent support too. Red light stimulates collagen production and increases fibroblast activity, the cellular processes behind firmer, smoother skin. In one study cited by the AAD, 90 patients received 8 LED treatments over 4 weeks, and more than 90% noticed improvement including softer skin, less redness, and lighter dark spots. Dr. Reynolds at Harvard, who describes herself as a former skeptic, now says the evidence convinced her: "I thought this was just the latest fad to get people to spend their money. But there's legitimate medical literature supporting it."
What makes these findings credible: they're consistent across multiple independent research groups, use proper controls (placebo/sham devices), and the effect sizes are large enough to be clinically meaningful. When an effect size exceeds 0.8, researchers consider it large. Hair density at 1.32 and fibromyalgia fatigue at 1.25 both clear that bar.
The claims that run ahead of the data
Scroll through TikTok or Instagram and you'll find red light therapy credited with fixing everything from depression to erectile dysfunction to athletic recovery. Some of these claims have a kernel of research behind them. Most overstate what the evidence supports.
Take athletic performance. A meta-analysis of 39 trials involving 861 participants found phototherapy showed "some effect" on time to exhaustion and repetitions, but the evidence quality ranged from "very low to moderate." A more recent 2025 meta-analysis of 12 studies found PBMT added an average of 3.87 extra repetitions compared to placebo -- statistically significant (p = 0.01) but hardly the transformative performance boost that influencer content suggests. The researchers themselves rated the evidence as "low or very low." And a meta-analysis of 6 RCTs involving 205 injured athletes found that while PBM reduced pain, it did not get athletes back to playing any faster.
Depression is another area where early results exist but aren't mature enough for strong recommendations. An analysis of 11 RCTs found PBM reduced depression symptoms (SMD = -0.55), but the effect on sleep was not statistically significant, and the authors rated their own evidence quality as "moderate or very low." Similarly, knee osteoarthritis research across 10 studies and 542 participants showed pain reduction at rest versus placebo, but the certainty of evidence was rated "very low."
The pattern across these emerging applications is consistent: small positive effects, small study sizes, methodological limitations, and researchers themselves flagging the need for better trials. As the Glass 2021 review in the Aesthetic Surgery Journal put it, red light therapy's "ubiquity and commercial success have outpaced empirical approaches on which solid clinical evidence is established."
Dr. Rahman at Stanford framed it precisely: "There's real evidence that shows red light can change biology. But that's not the same as saying it's some kind of panacea for many different health conditions." Stanford sleep expert Jamie Zeitzer and sports physician Michael Fredericson both say the data for sleep and athletic performance applications is lacking. Claims about erectile dysfunction, weight loss, and dementia reversal remain speculative at this point.
| Claim | Evidence status | What the research shows |
|---|---|---|
| Hair regrowth | Supported | Multiple large RCTs; comparable to minoxidil for androgenetic alopecia |
| Skin anti-aging | Supported | Consistent findings across studies for wrinkles, texture, collagen |
| Oral mucositis (cancer treatment) | Guideline-approved | Included in NICE and MASCC treatment guidelines |
| Knee OA pain | Preliminary | Positive signal but very low evidence certainty |
| Athletic performance | Preliminary | Small measurable effects; low to very low evidence quality |
| Depression | Preliminary | 11 RCTs show effect but evidence quality low |
| Weight loss | Not supported | Temporary body contouring, not actual fat loss |
| Erectile dysfunction | Not supported | No scientifically validated results |
| Dementia reversal | Not supported | Animal studies only; human evidence absent |
What to look for, what to ignore, and who should skip it
If you've read this far and still want to try red light therapy, here's what matters when choosing a device -- and what's marketing noise.
Wavelength. The research literature consistently uses wavelengths between 630 and 850 nm. For skin concerns, 630 nm is the most-studied wavelength. For deeper tissue applications (joint pain, muscle recovery), 808-850 nm appears more often in clinical trials. Some devices advertise wavelengths like 940 nm for neurological benefits, but the evidence supporting these specific claims is thin. A device covering the 630-850 nm range gives you the best alignment with published research.
Power density. A device's irradiance (measured in mW/cm2) determines how much energy reaches your tissue. Many consumer devices don't disclose this specification, which makes it impossible to know whether you're getting a therapeutic dose. The Dior x Lucibel mask used in the published study delivered 21.7 mW/cm2. If a manufacturer won't tell you the irradiance, that's a red flag.
FDA clearance as a minimum. Look for the words "FDA cleared" or "FDA 510(k) cleared" on the packaging. As the AAD explains, this means the device poses low risk. It doesn't mean it works well. But a device without even this clearance has passed no regulatory review at all.

Who should avoid red light therapy. People with darker skin tones should consult a dermatologist first -- research shows increased sensitivity to visible light including red light, which can cause hyperpigmentation. Dr. Reynolds at Harvard recommends people with darker skin start with lower doses. Anyone with light-sensitive conditions (such as lupus) or taking photosensitizing medications (including certain antibiotics) should also skip it. And always use the eye protection that comes with your device -- red light can cause eye damage without proper shielding.
The safety profile is solid. Red light therapy is not toxic, not invasive, and doesn't use UV radiation. Multiple sources confirm no evidence of cancer risk. Side effects are minimal and temporary -- mostly mild redness or irritation. That said, long-term safety data doesn't exist yet, which is worth knowing if you plan to use a device daily for years.
What doesn't matter: brand ambassadors, influencer testimonials, devices that promise results in "just 5 minutes a day," and any product claiming to treat 15+ conditions. The research supports a narrow set of applications with moderate evidence, and a broader set with preliminary, low-certainty findings. Match your expectations to that reality.
Frequently Asked Questions
Does red light therapy actually work for wrinkles?
The evidence is positive but measured. Multiple clinical studies show red light stimulates collagen production and improves skin texture, and the AAD notes that more than 90% of patients in one study reported noticeable improvement after 8 sessions. Results require consistent use over months and depend on the device's power output. Clinical devices produce better results than most home devices. Expect subtle improvement, not dramatic transformation.
Is red light therapy safe for daily use?
Short-term use appears safe, with minimal side effects limited to temporary mild redness. Red light does not use UV radiation and has shown no cancer risk. However, long-term safety data is not yet available. Research on dosing suggests sessions spaced 48-72 hours apart may be more effective than daily use, as cells need time to process the energy stimulus. Always wear eye protection when using facial or full-body devices.
How long before you see results from red light therapy?
According to Dr. Reynolds at Harvard, home devices need to be used multiple times per week for four to six months to produce visible results. Clinical treatments may show changes faster due to higher power output. Hair regrowth studies typically run 12-26 weeks. Anyone promising visible results in under a month is overstating what the research supports.
Can red light therapy help with pain or inflammation?
There is early evidence. The 2025 umbrella review found moderate evidence for reducing disability in knee osteoarthritis and fatigue in fibromyalgia. A meta-analysis of injured athletes found pain reduction but no faster return to play. The evidence exists but is rated low to very low certainty by the researchers themselves. PBM may be worth trying alongside established treatments, but should not replace them.
What's the difference between red light therapy and infrared saunas?
Different technologies. Red light therapy uses specific wavelengths (typically 630-850 nm) at low power to trigger photobiomodulation at the cellular level without generating significant heat. Infrared saunas use far-infrared wavelengths (beyond 1100 nm) primarily to generate heat and induce sweating. The biological mechanisms are different, and research supporting one does not apply to the other.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











