
Your body's oxygen ceiling, explained
VO2 max is the maximum rate at which your body can consume oxygen during all-out exercise. The "V" stands for volume, "O2" for oxygen, and "max" for the upper limit. It is reported in milliliters of oxygen used per kilogram of body weight per minute (ml/kg/min).
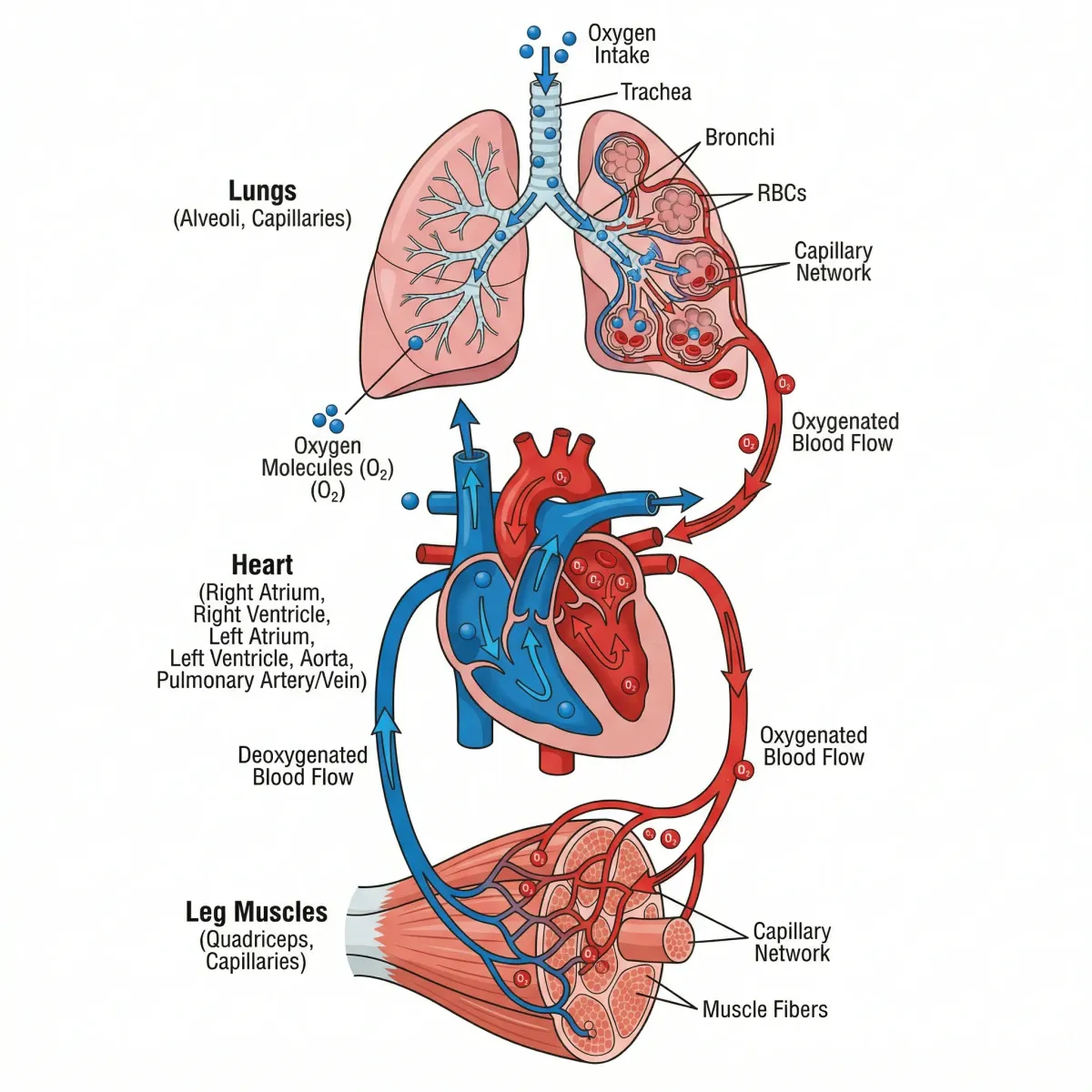
During any physical effort, your muscles demand oxygen to convert fuel into energy. Walk up a flight of stairs and the demand is modest. Sprint up ten flights and the demand spikes. At some point, no matter how hard you push, oxygen delivery and utilization plateau. That plateau is your VO2 max.
Three systems determine this ceiling. First, your lungs pull oxygen from inhaled air. Second, your heart and blood vessels transport that oxygen through the circulatory system. Third, your skeletal muscles extract and use it to produce ATP, the energy currency that powers contraction. A bottleneck in any of these three steps lowers the ceiling.
The American Heart Association published a scientific statement in 2016 calling cardiorespiratory fitness (CRF) a clinical vital sign that should be routinely assessed. The statement, authored by Ross et al. in Circulation, reviewed decades of evidence and concluded that low CRF is among the strongest predictors of death from any cause.
Clinicians often express CRF in metabolic equivalents, or METs, rather than raw VO2 numbers. One MET equals 3.5 ml/kg/min, roughly the oxygen cost of sitting still. If your VO2 max is 35 ml/kg/min, your peak capacity is about 10 METs, meaning you can sustain an effort ten times greater than rest. This MET framework makes fitness data comparable across ages, body sizes, and testing methods.
How VO2 max testing works
The gold standard test uses a metabolic cart, a rolling machine that collects and analyzes every breath you take during progressive exercise. You wear a sealed face mask or mouthpiece while running on a treadmill or pedaling a stationary bike. Every few minutes the intensity increases. The cart measures the volume of air you inhale and exhale, plus the concentration of oxygen and carbon dioxide in each breath. When your oxygen consumption stops rising despite increasing effort, you have hit your VO2 max.
This cardiopulmonary exercise test (CPET) yields the most accurate result and also provides other clinically valuable data: your ventilatory threshold, heart rate recovery, and the efficiency of your breathing. The AHA's 2016 scientific statement reviewed prediction equations from dozens of studies showing that treadmill protocols (particularly the Bruce and modified Balke protocols) produce reliable VO2 estimates even without direct gas analysis.
| Test type | What it measures | Accuracy | Cost |
|---|---|---|---|
| CPET with metabolic cart | Direct gas exchange, true VO2 max | Gold standard | $150-$500 |
| Treadmill ETT (estimated) | Peak METs from speed/grade formula | Within 10-15% of direct measurement | $100-$300 |
| Cooper 12-minute run | Distance covered, estimates VO2 max | Moderate (outdoor, self-paced) | Free |
| 1-mile walk test (Rockport) | Finish time + heart rate, estimates VO2 | Moderate for low-fit populations | Free |
| Wearable estimate (Apple Watch, Garmin) | Algorithmic estimate from HR and pace | Rough ballpark, can be off by 10-20% | Device cost only |
If you cannot access a lab, field tests offer a reasonable approximation. The Cooper 12-minute run is straightforward: cover as much ground as possible on a track, then plug the distance into a validated formula. Your VO2 max in ml/kg/min equals roughly (distance in meters minus 504.9) divided by 44.73. For people who cannot run, the Rockport one-mile walk test uses your walking time and post-exercise heart rate to generate an estimate.
Consumer wearables have brought VO2 max tracking to millions of wrists, though the estimates carry wide margins. They correlate heart rate patterns with pace data during outdoor runs. The algorithms get better as they learn your physiology, but they are not lab-grade. Track the trend over months rather than obsessing over any single reading.
The longevity connection: what 122,007 patients revealed
In 2018, a team led by Kyle Mandsager at the Cleveland Clinic published one of the largest studies ever conducted on fitness and lifespan. The retrospective cohort study followed 122,007 consecutive patients who completed exercise treadmill testing between 1991 and 2014, with a median follow-up of 8.4 years. The findings upended a popular debate about whether extreme fitness might eventually cause harm.
The researchers classified patients into five fitness tiers based on age- and sex-matched CRF: low (bottom 25th percentile), below average (25th-49th), above average (50th-74th), high (75th-97.6th), and elite (top 2.3%). Death occurred in 13,637 patients during 1.1 million person-years of observation.
Being in the lowest fitness group carried a 5-fold higher mortality risk compared to the fittest individuals (adjusted HR 5.04; 95% CI, 4.10-6.20). There was no observed upper limit of benefit. Even at the extremes, the fittest patients lived longer.
The risk of low fitness exceeded the risk of smoking (HR 1.41), diabetes (HR 1.40), and coronary artery disease (HR 1.29). Being sedentary and unfit was statistically more dangerous than being a smoker, a diabetic, or having documented heart disease.

Critically, the benefit of elite fitness over high fitness persisted even in patients over age 70 (adjusted HR 0.71) and in those with hypertension (adjusted HR 0.70). The study left no room for hedging: there is no level of fitness beyond which more becomes harmful. Physicians should push patients toward the highest CRF they can manage.
The AHA's review reinforced this, citing evidence that each 1-MET increase in CRF corresponds to a 12-15% reduction in all-cause mortality. Put concretely: if your current capacity is 8 METs and you train until you hit 10 METs, your mortality risk drops by roughly 24-30%. No pill on the market matches that.
The relationship between CRF and mortality applies beyond cardiovascular death. Higher VO2 max is associated with lower risk of cancer, dementia, and metabolic disease. The AHA's statement noted that CRF independently predicts outcomes even after controlling for traditional risk factors like cholesterol, blood pressure, and blood glucose. Fitness does something medication cannot replicate on its own.
Where you stand: age and sex-based benchmarks
VO2 max declines with age at a rate of roughly 10% per decade after age 30, though this rate varies significantly based on training status. Trained individuals decline more slowly. Women generally have VO2 max values 20-25% lower than men of the same age due to differences in hemoglobin concentration, heart size, and lean body mass.
The following table reflects typical VO2 max ranges. These are drawn from population data including the FRIEND registry (Fitness Registry and the Importance of Exercise National Database), which compiled CPET results from over 7,000 Americans to establish national fitness norms.
| Age group | Men - Poor | Men - Average | Men - Good | Men - Excellent |
|---|---|---|---|---|
| 20-29 | < 33 | 33-42 | 43-52 | > 52 |
| 30-39 | < 31 | 31-38 | 39-48 | > 48 |
| 40-49 | < 28 | 28-35 | 36-44 | > 44 |
| 50-59 | < 25 | 25-33 | 34-41 | > 41 |
| 60-69 | < 22 | 22-30 | 31-37 | > 37 |
| 70+ | < 19 | 19-26 | 27-33 | > 33 |
| Age group | Women - Poor | Women - Average | Women - Good | Women - Excellent |
|---|---|---|---|---|
| 20-29 | < 27 | 27-35 | 36-44 | > 44 |
| 30-39 | < 25 | 25-32 | 33-41 | > 41 |
| 40-49 | < 23 | 23-29 | 30-37 | > 37 |
| 50-59 | < 20 | 20-27 | 28-34 | > 34 |
| 60-69 | < 18 | 18-24 | 25-31 | > 31 |
| 70+ | < 15 | 15-21 | 22-28 | > 28 |
These numbers matter more than most people realize. In the Mandsager study, the low-fitness group (roughly the bottom quartile) had a five-fold higher mortality risk. Moving from poor to average already delivers a substantial mortality reduction. You do not need to reach elite status. The steepest part of the survival curve runs between the bottom and the middle of the distribution.
If you already track biological age markers, VO2 max is one of the strongest functional measures to include. Unlike epigenetic clocks, which require blood draws and lab processing, VO2 max testing gives you a number you can act on immediately through training.
Training protocols that move the needle
VO2 max responds to training. And the people starting from the lowest baseline gain the most. A 2015 meta-analysis by Milanovic et al. in Sports Medicine pooled data from 28 controlled trials and found that both high-intensity interval training and steady-state endurance training produced large improvements in VO2 max, with HIIT showing a modest edge.
| Training type | VO2 max improvement | Time per session | Sessions per week | Best for |
|---|---|---|---|---|
| 4x4 min HIIT | ~5.5 ml/kg/min | 25-40 min | 2-3 | Time-efficient, measurable gains |
| 10x1 min HIIT | ~4-5 ml/kg/min | 20-25 min | 3 | People who prefer shorter bursts |
| Zone 2 endurance | ~4.9 ml/kg/min | 45-90 min | 3-5 | Building aerobic base, recovery |
| Combined (HIIT + Zone 2) | ~6-7 ml/kg/min | Varies | 4-5 total | Maximizing adaptation |
| Sprint intervals (SIT) | ~4-5 ml/kg/min | 10-20 min | 3 | Young, healthy, time-crunched |
The 4x4 protocol
The Norwegian 4x4 method is the most studied protocol for VO2 max gains: four bouts of four minutes at 85-95% of your maximum heart rate, with three minutes of easy recovery between each. A review in the World Journal of Cardiology by Ito (2019) reported a 70-75% positive improvement rate across trials in both cardiac patients and healthy adults.
The session takes about 25 minutes of actual work plus warm-up and cool-down. On a bike, treadmill, rower, or even an uphill trail, the execution is the same: push hard enough that speaking becomes difficult during the four-minute intervals, then bring your heart rate back down during recovery.
Zone 2: the slow burn that builds the foundation
Intensity is only half the equation. Zone 2 training, the conversational-pace effort where you can still hold a sentence, builds the mitochondrial density and capillary network your aerobic system runs on. It sits at roughly 60-70% of max heart rate, right in the fat-burning sweet spot.
The Milanovic meta-analysis found endurance training alone improved VO2 max by 4.9 ml/kg/min on average. While slightly less than HIIT in controlled trials, zone 2 training carries lower injury risk, generates less fatigue, and allows higher weekly volume. Most exercise physiologists now recommend a polarized approach: 80% of training time in zone 2, 20% at high intensity. This pattern is common among elite endurance athletes for a reason.
Why the combination works
HIIT primarily strengthens the central plumbing: bigger stroke volume, higher cardiac output, more oxygen delivered per heartbeat. Zone 2 strengthens the peripheral hardware: more mitochondria per muscle fiber, better fat utilization, a denser web of capillaries reaching muscle tissue. Combine them and you are improving both sides of the VO2 max equation at once. The National Heart, Lung, and Blood Institute notes that regular moderate-to-vigorous physical activity strengthens the heart muscle and improves its ability to pump blood to the lungs and muscles, widening capillaries and increasing oxygen delivery.
A practical starting point for someone who currently does little structured exercise: begin with three zone 2 sessions per week (30-45 minutes each), then add one HIIT session after four weeks. Build gradually. The American College of Sports Medicine recommends at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic activity per week, plus resistance training on two or more days.
Do not skip strength training either. VO2 max depends partly on how much metabolically active muscle tissue you carry. Lose muscle to inactivity or aging and you shrink the engine that uses oxygen, no matter how efficiently your heart pumps.
Myths vs. evidence
| Myth | What the evidence says |
|---|---|
| VO2 max is genetic and cannot be improved | Genetics set a ceiling, but training can improve VO2 max by 15-20% in most people. Untrained individuals often see gains of 5-6 ml/kg/min within 8-12 weeks. |
| Too much exercise is dangerous for your heart | The Mandsager study of 122,007 patients found no upper limit of fitness benefit. Elite fitness (top 2.3%) carried the lowest mortality risk, even beyond the high-fitness group. |
| Only young people can improve their VO2 max | The AHA's review found that adults in their 60s and 70s still improve VO2 max with training. The Mandsager study showed elite fitness benefited patients over 70 (HR 0.71 vs high fitness). |
| You need a lab test to know your VO2 max | Lab testing is the gold standard, but field tests (Cooper run, Rockport walk) provide useful estimates. Wearables offer rough trend tracking over time. |
| Steady-state cardio is the best way to improve VO2 max | HIIT produces slightly larger VO2 max gains than endurance training alone (5.5 vs 4.9 ml/kg/min in meta-analysis), though both are effective. A combination appears optimal. |
| VO2 max only matters for athletes | Low CRF carries a mortality risk five times higher than elite fitness and exceeds the risk of smoking or diabetes. It matters for everyone. |
Frequently Asked Questions
What is a good VO2 max for my age?
For men aged 40-49, an average VO2 max falls between 28 and 35 ml/kg/min, with values above 36 considered good. For women of the same age, average is 23-29, with good being 30 or above. But the mortality data suggests that even moving from poor to average delivers a significant reduction in death risk, so the goal is to improve from wherever you start, not to hit a specific number.
How quickly can I improve my VO2 max?
Most studies show measurable improvements in 4-8 weeks of consistent training. The Milanovic meta-analysis found average gains of 5-6 ml/kg/min across 28 trials, with people starting from lower baselines seeing the largest improvements. The rate of gain slows as you approach your genetic ceiling, but it rarely stops entirely with continued training stimulus.
Is VO2 max the same as cardiorespiratory fitness?
VO2 max is the single best laboratory measure of cardiorespiratory fitness (CRF), and the two terms are often used interchangeably. CRF can also be estimated through peak METs on a treadmill test or even non-exercise prediction equations that use age, weight, resting heart rate, and activity level. The AHA considers CRF, however measured, a clinical vital sign.
Does creatine or any supplement improve VO2 max?
Creatine helps with short-burst power and may indirectly support higher-quality training sessions, but it does not directly raise VO2 max. No supplement meaningfully replaces training. Beetroot juice (dietary nitrate) has shown small improvements in exercise efficiency in some studies, but the effect on VO2 max itself is marginal. Training remains the primary lever.
Can I rely on my Apple Watch or Garmin for VO2 max?
Consumer wearable estimates use algorithms based on heart rate and pace data during outdoor exercise. They can be off by 10-20% compared to lab testing, and they tend to underperform for people who do not run regularly outdoors. That said, tracking the trend over months is more valuable than any single number. If your wearable shows your estimated VO2 max climbing over 12 weeks of training, that directional signal is meaningful even if the absolute number is imprecise.
Related Articles
- Zone 2 Cardio for Fat Burning and Longevity — A deep look at the low-intensity training zone that builds the aerobic foundation for higher VO2 max.
- Biological Age Testing: How to Measure and Improve Your Pace of Aging — VO2 max is one of the strongest functional biomarkers of aging alongside epigenetic clocks.
- Resistance Training for Women Over 40: Bone Density, Metabolism, and Hormones — Strength training preserves the muscle mass that supports oxygen extraction and VO2 max.
- Autophagy: How to Trigger It Through Fasting, Exercise, and Diet — Exercise-induced autophagy is one mechanism linking high CRF to lower disease risk.
- Creatine Benefits Beyond Muscle: Brain, Bone, and Longevity — How creatine supports training quality without directly improving VO2 max.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











