
What Counts as a Muscle-Building Peptide?
Bodybuilding forums use the word "peptide" loosely. In the strict sense, a peptide is a short chain of amino acids. In the gym, the label gets stretched to include growth hormone secretagogues, growth factors, fragments of growth hormone, and peptide-adjacent compounds sold in the same underground menu. That loose language matters because a compound can sound gentle while still pushing a banned hormone pathway.
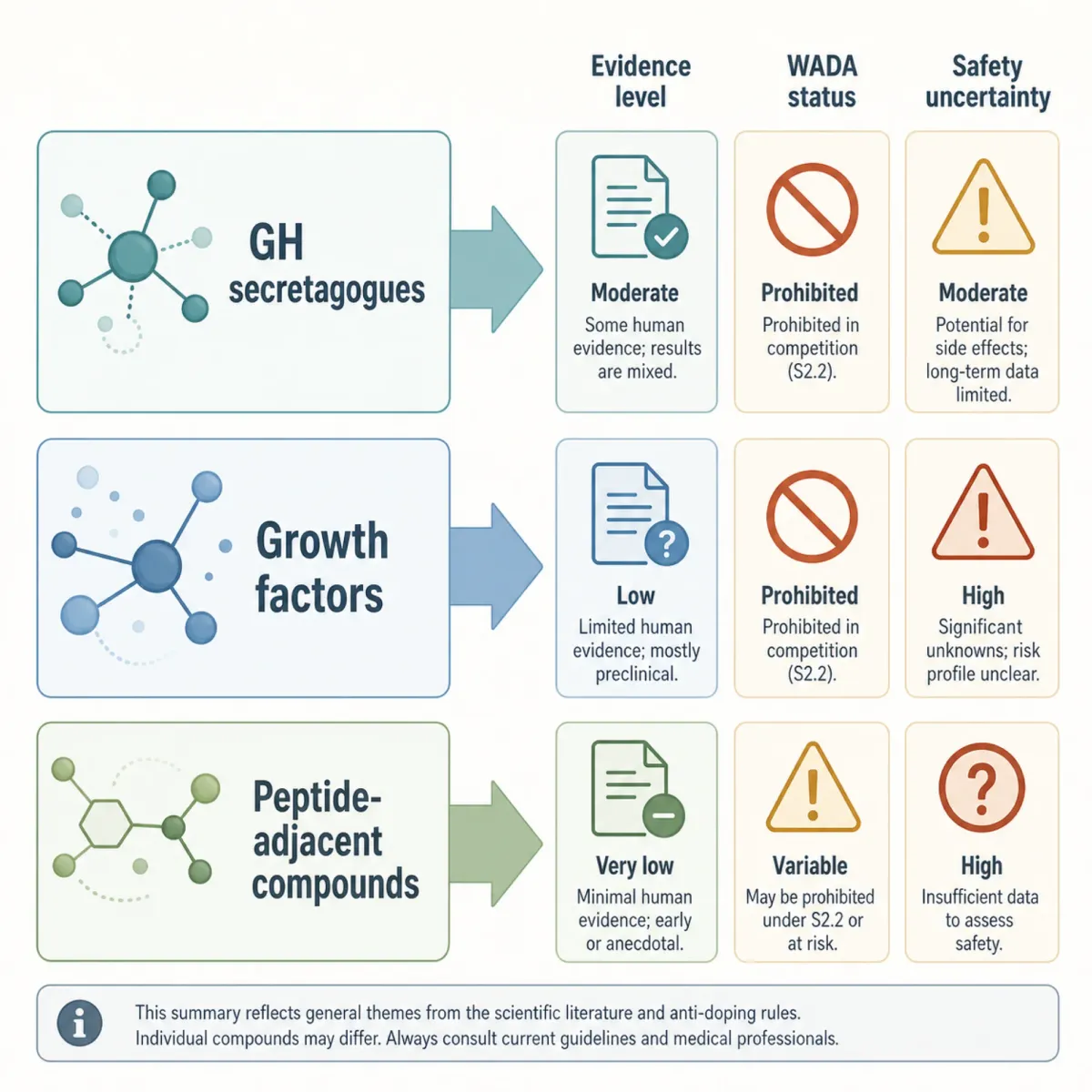
The cleanest way to sort the category is by signal. Growth hormone secretagogues are meant to nudge the pituitary into releasing growth hormone, a hormone associated with lean body mass, fat mass, exercise tolerance, maximum oxygen uptake, and muscle strength in clinical literature reviewed by John T. Sigalos and Alexander W. Pastuszak. Think of the endocrine system like a thermostat: the secretagogue is not the furnace, but it can keep pressing the button that asks for more heat.
That distinction is why peptide marketing can feel persuasive. Sigalos and Pastuszak note that growth hormone secretagogues promote pulsatile growth hormone release that remains subject to negative feedback in their clinical review. In plain English, the body still has some brakes. The problem is that brakes are not the same thing as proof of safety, especially when healthy lifters use compounds studied mainly in medical contexts.
Bottom line: "peptide" does not mean legal, approved, muscle-specific, or low risk. It only tells you something about structure or signaling.
The 7 Peptides Bodybuilders Talk About Most
The list below is not a recommendation. It is a map of what gets discussed, why the claims sound attractive, and where the evidence gets thin. The most evidence-backed statement is often not "this builds muscle in healthy bodybuilders." It is "this affects a pathway that bodybuilders care about."
| Peptide or family | Why bodybuilders talk about it | Evidence caution |
|---|---|---|
| CJC-1295 | A long-acting GHRH analog; in healthy men it raised basal GH 7.5-fold. | The study measured endocrine response, not long-term bodybuilding outcomes. |
| Ipamorelin | Discussed as a GH secretagogue and paired in commercial "lean mass" stacks. | WADA lists ipamorelin among prohibited GH secretagogues at all times. |
| Sermorelin | A GHRH analogue marketed as a softer GH-support option. | WADA lists sermorelin among prohibited GHRH analogues in S2. |
| Tesamorelin | Discussed for body recomposition because it affects the GH/IGF axis. | WADA lists tesamorelin among prohibited GHRH analogues in S2. |
| Hexarelin | Marketed as a stronger GH-releasing peptide for mass phases. | Hexarelin appears in WADA's prohibited GHRP examples as examorelin in S2. |
| IGF-1 analogues | Promoted for direct anabolic signaling and muscle-fiber growth claims. | IGF-1 and analogues are prohibited growth factors under WADA S2.3. |
| MGF and PEG-MGF | Sold around satellite-cell and repair language after hard training. | Mechano growth factors are named as prohibited growth factors by WADA in S2.3. |
CJC-1295 is the most interesting evidence story because the clinical signal is measurable. In a study by Madalina Ionescu and Lawrence A. Frohman, healthy men had overnight blood sampling before and after CJC-1295; the study reported preserved GH pulsatility, a 7.5-fold rise in trough GH, a 46% rise in mean GH, and a 45% rise in IGF-I. That is a real endocrine effect. It is not the same as proof that healthy lifters gain contractile muscle safely over years.
Ipamorelin, sermorelin, tesamorelin, and hexarelin sit in the same practical neighborhood: they are discussed because they talk to the GH axis. The marketing pitch usually sounds less intimidating than anabolic steroids because it frames these compounds as "signals" rather than replacement hormones. But anti-doping rules do not grade substances by how soft the copy sounds. WADA names ipamorelin, sermorelin, tesamorelin, and hexarelin-related GHRPs in the same prohibited S2 framework that covers GH-releasing factors and secretagogues.
Tesamorelin and sermorelin are especially easy to misread because they appear in medical and wellness contexts. A clinic page can discuss them as prescription or supervised therapies, while a bodybuilding forum turns the same names into recomposition shorthand. Those are different conversations. The source that matters for sport eligibility is not the clinic page; it is the prohibited-list category that names the pathway under GHRH analogues.
IGF-1 analogues and MGF are a step closer to the muscle itself in the way they are marketed. Commercial pages describe IGF-1 LR3, MGF, and PEG-MGF around hyperplasia, satellite cells, and repair language in bodybuilding-market content. That is useful as a snapshot of what lifters hear. It is weaker as proof. WADA's list treats IGF-1 analogues and mechano growth factors as prohibited growth factors because they affect tissue-growth pathways.
The seventh bucket is not one molecule but a pattern: GH fragments and analogues marketed for cutting, recovery, or "clean" recomposition. WADA lists GH fragments such as AOD-9604 and hGH 176-191 in the same S2 section. That matters because many lifters think risk rises only when something is overtly anabolic. In practice, fat-loss fragments, repair peptides, and growth-factor mimetics can all cross the same legal and testing line.
The practical read: these compounds sit closer to hormone manipulation than to supplements. If a product page makes them sound like creatine with a lab coat, the language is doing too much work.

Where the Evidence Stops and Gym-Floor Claims Begin
The stronger the claim, the more you should ask what population was actually studied. A wasting-state trial, an endocrine-response study, or a disease-focused muscle disorder paper cannot be copy-pasted onto a healthy 27-year-old trying to add shoulder width.
Sigalos and Pastuszak found that GHSs might improve growth velocity in children, stimulate appetite, improve lean mass in wasting states and obese individuals, increase fat-free mass, and improve sleep across available human studies. That is a broad clinical signal, but it is not a green light for physique use. Their same review says few long-term, rigorously controlled studies have examined GHS efficacy and safety in humans.
Myostatin hype has a similar problem. Myostatin blockade is fascinating because myostatin helps restrain muscle growth; bodybuilders hear that and imagine an off switch for limits. But the PubMed record connected to the review "Are big muscles necessarily good muscles?" points to a phase I/II MYO-029 trial in adult muscular dystrophy, not a proven hypertrophy program for healthy athletes.
| Claim type | What is better supported | What remains weak |
|---|---|---|
| Endocrine effect | CJC-1295 changed GH and IGF-I markers in one human study. | Long-term physique outcomes in healthy bodybuilders. |
| Secretagogue safety | Short-term studies often describe tolerability in selected groups. | Cancer incidence, mortality, and years-long use. |
| Myostatin manipulation | Disease-focused and mechanistic muscle research exists in PubMed-linked literature. | Safe enhancement in healthy lifters. |
The useful analogy is a dyno test for a car engine. A lab can show the engine makes more power under a controlled condition. It does not prove the car is safe on public roads, insurable, legal, or reliable after 80,000 miles.

The 3 Compounds Many Lifters Quietly Avoid
The underground peptide conversation does not stay neatly inside peptide chemistry. Cutting agents, tanning peptides, metabolic modulators, and "research only" substances get sold to the same audience. The better athletes learn to avoid the ones where risk overwhelms reward.
| Avoid list | Why it shows up | Why cautious lifters back away |
|---|---|---|
| Melanotan II | Tanning and stage appearance. | It is illegal to buy in the United States and unregulated online according to Healthline's medical review. |
| BPC-157 and other unapproved research compounds | Recovery claims and injury chatter. | WADA's S0 category prohibits unapproved substances and specifically names BPC-157 as an example. |
| GW1516/DNP/PGCL-style cutting compounds | Fat-loss and conditioning promises. | WADA lists GW1516 as prohibited, while DNP is named under S0 and has fatal hyperthermia risk on the Prohibited List. |
Melanotan II is the easiest to misunderstand because it is not pitched as a strength drug. It is pitched as a shortcut to a darker look. Healthline's review says tanning injections are currently illegal to buy in the United States and can increase skin-cancer risk through several pathways. It also notes that melanotan II can cross the blood-brain barrier and may cause appetite loss, sexual dysfunction, and fatigue because it binds a wider range of receptors.
DNP and PGCL-style cutting claims are even more blunt. A patent document describing a fat-loss composition says DNP increases metabolic rate and body temperature by uncoupling oxidative phosphorylation, with no ceiling to its temperature-increasing effect in its background section. The same document says acute human exposure of 20 to 50 mg/kg can be lethal. That is not a "hardcore" risk. That is a fire alarm.
The practical implication is simple: if a compound is mainly discussed in the same breath as secrecy, contest prep desperation, or "research only" loopholes, treat the marketing as a warning label.

The Legal, Testing, and Quality-Control Trap
WADA does not treat most of this category as harmless wellness experimentation. Its S2 category names GH fragments such as AOD-9604 and hGH 176-191, GHRH analogues such as CJC-1295, sermorelin, and tesamorelin, GH secretagogues such as ibutamoren and ipamorelin, and GHRPs such as hexarelin as prohibited at all times. It also lists IGF-1 analogues, mechano growth factors, TB-500, and other growth factors that affect muscle, tendon, ligament protein synthesis, vascularisation, energy use, regenerative capacity, or fibre-type switching under S2.3.
That list is broader than many gym conversations admit. It is not just "steroids are banned." The signal pathways that make peptides attractive for hypertrophy, recovery, and recomposition are exactly the pathways anti-doping rules watch.
Quality control is the quieter trap. Healthline notes that online tanning-injection sellers are not monitored by a governing health organization, creating a high risk that products are mislabeled or contain impurities in its safety review. That warning was about tanning peptides, but the logic applies across the gray market. A vial can be risky because of the molecule, the label, the contaminant, or the fact that no one accountable made it.
Side Effects That Matter Before Any Physique Claim
The side-effect conversation should start before the before-and-after photo. Sigalos and Pastuszak report concern that GHSs may increase blood glucose because of decreased insulin sensitivity in available human studies. For a bodybuilder already pushing calories, stimulants, sleep debt, and stress hormones, that is not a footnote.
The longer-term unknowns are larger. The same review says more work is needed to understand the long-term impact of GHSs on human anatomy and physiology, including cancer incidence and mortality with prolonged use. That is the part marketing pages tend to blur. They sell the "signal"; they do not own the decade-long uncertainty.
Injection-related risks also do not require a rare molecule. Healthline warns that tanning injections carry risks seen with improperly prepared injections, including contamination concerns, and notes the broader risk of mislabeled or impure products when bought online. The mechanism is like buying a race tire from a mystery warehouse. Even if the tread pattern looks right, you do not know the rubber compound, age, storage conditions, or whether the label is true.
For readers, the practical question is not "Can this pathway build muscle?" It is "What level of evidence would justify changing a hormone pathway when training, protein, sleep, and progressive overload already move the needle?" For most noncompetitive lifters, that answer is higher than the internet makes it sound.

A Safer Way to Read Peptide Hype
Read every peptide claim in two passes. First ask, "What pathway does this affect?" Then ask, "What human outcome was actually measured?" If the evidence only shows a hormone marker, do not let a marketing page silently upgrade that into permanent muscle gain.
A good rule: the more precise the claim sounds, the more precise the source should be. A statement about a GH marker should point to a clinical study like the CJC-1295 PubMed record with its measured endocrine outcomes. A statement about sport eligibility should point to WADA's Prohibited List rather than a clinic FAQ. A statement about long-term safety should admit when Sigalos and Pastuszak say more long-term evaluation is needed for cancer incidence and mortality.
Commercial peptide pages can still tell you something useful: what the market is selling and what bodybuilders are hearing. They should not be treated as the proof layer. In this topic, the proof layer is thinner, more conditional, and more regulatory than the sales pitch, especially when competition eligibility or long-term endocrine risk is on the table.
That does not make every peptide claim fake. It means the burden of proof should rise with the size of the promise. A modest recovery claim needs a different evidence bar than a claim about new muscle fibers, long-term hormone manipulation, or staying eligible in tested sport. The closer a compound moves toward GH, IGF-1, or growth-factor signaling, the more the conversation should shift from "Does anyone use it?" to "Who studied it, in whom, for how long, and under what rules?" That last question is usually where the pitch gets quiet.
If a peptide pitch skips legality, testing, insulin sensitivity, long-term safety, and product purity, it is not an evidence review. It is a sales funnel.

Frequently Asked Questions
Are muscle-building peptides legal for athletes?
Many are not allowed in tested sport. WADA lists GH fragments, GHRH analogues, GH secretagogues, GHRPs, IGF-1 analogues, mechano growth factors, and TB-500-related compounds as prohibited at all times.
Is CJC-1295 proven to build muscle?
CJC-1295 has human evidence for endocrine effects: one study reported a 7.5-fold increase in trough GH and a 45% increase in IGF-I. That does not prove safe, durable muscle gain in healthy bodybuilders.
Why do bodybuilders talk about IGF-1 and MGF?
They sit close to muscle-growth signaling. WADA lists IGF-1 analogues and mechano growth factors as prohibited growth factors under S2.3, which is a clue that the pathway is powerful enough to be regulated.
Which peptide-adjacent compounds are the biggest red flags?
Melanotan II, BPC-157-style unapproved research compounds, and GW1516/DNP/PGCL-style cutting compounds deserve special caution because the risk story is dominated by unregulated sale, prohibited status, or severe toxicity signals in anti-doping rules.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











