
What Happens to Your Body After 40
Somewhere around 40, things start shifting. Muscle tissue shrinks. Bones thin out. The hormones that used to regulate your sleep, your weight, your energy start doing things they never did before. It is not dramatic. Most women do not notice it happening until the cumulative effect catches up years later.
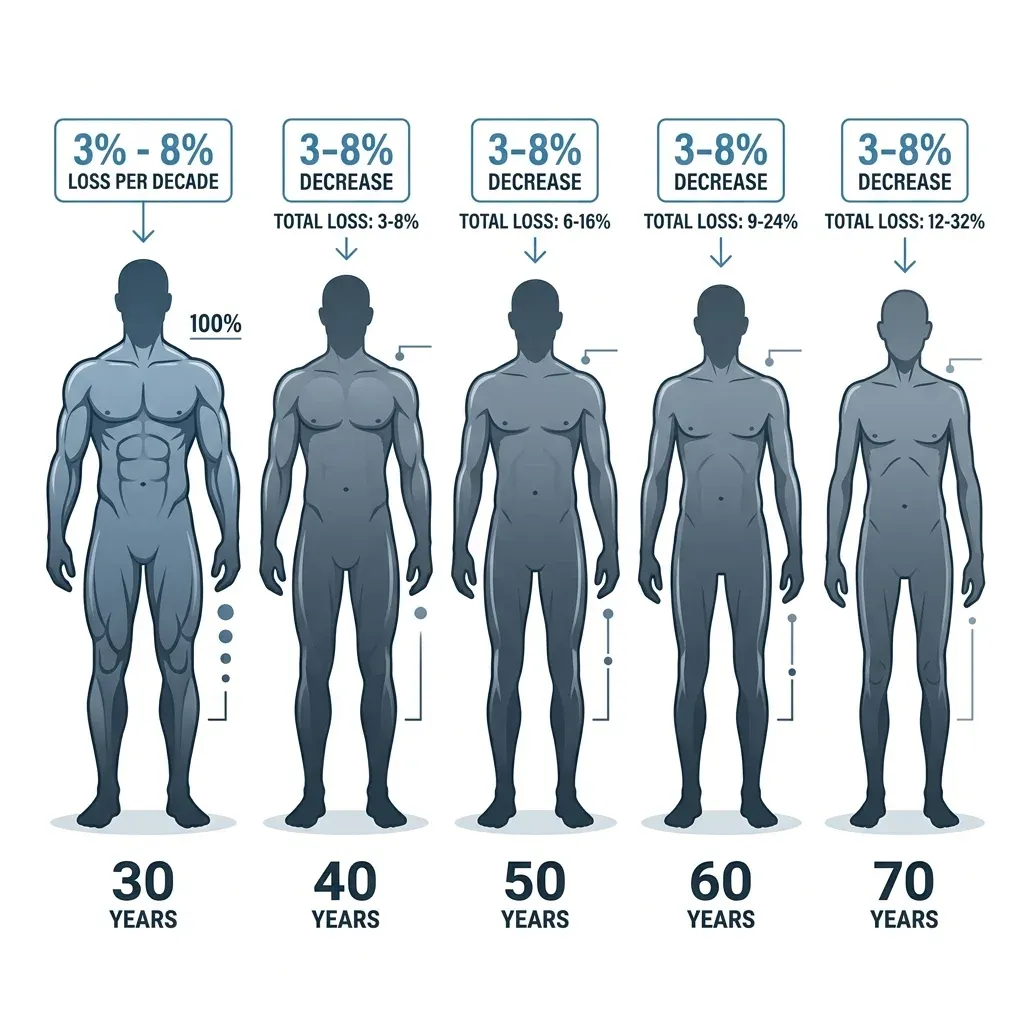
The clinical term for age-related muscle loss is sarcopenia, and it begins earlier than most people realize. Research published in Current Sports Medicine Reports found that inactive adults lose between 3% and 8% of their muscle mass per decade, a process accompanied by a gradual reduction in resting metabolic rate and an increase in fat accumulation. For women specifically, these changes intersect with the hormonal shifts of perimenopause and menopause, which accelerate both bone and muscle loss due to declining estrogen levels.
Bone density follows a similar trajectory. Women can lose up to 20% of their bone density in the five to seven years following menopause, according to the National Osteoporosis Foundation. The lumbar spine and femoral neck — the area connecting the thighbone to the hip joint — are especially vulnerable, and fractures at these sites carry serious consequences for independence and long-term health.
The bottom line: After 40, your body is quietly losing muscle and bone while gaining fat. Resistance training is one of the few interventions that can address all three simultaneously.
How Lifting Weights Rebuilds Bone from the Inside Out
Bones are not static structures. They are living tissue constantly being broken down and rebuilt through a process called remodeling. When you apply mechanical load to a bone — the kind of force generated during a squat, deadlift, or overhead press — specialized cells called osteoblasts respond by laying down new bone tissue. This is why astronauts lose bone density in zero gravity: without load, the remodeling process tips toward breakdown.
The evidence supporting resistance training for bone health in women after menopause is extensive. A meta-analysis of 80 controlled exercise trials involving 5,581 postmenopausal women, published in Osteoporosis International (2023), found consistent improvements in bone mineral density across three critical sites: the lumbar spine (SMD 0.29), femoral neck (SMD 0.27), and total hip (SMD 0.41). The total hip showed the most robust response, and the benefits held regardless of whether women had existing osteopenia or osteoporosis.
But not all resistance training produces the same bone-building response. A 2025 meta-analysis published in the Journal of Orthopaedic Surgery and Research drilled into the specific training parameters that matter. Across 17 randomized controlled trials involving 690 postmenopausal women, the researchers found that high-intensity training — working at 70% or more of your one-repetition maximum — produced the strongest effects on bone density at the femoral neck and total hip. Three training sessions per week was the optimal frequency, and programs lasting 48 weeks or longer showed the most meaningful changes.
A separate network meta-analysis published in Scientific Reports (2025), which examined 56 randomized controlled trials covering 4,263 postmenopausal women, confirmed that resistance training was most effective for lumbar spine density (SMD 0.86), while a combination of resistance and aerobic exercise ranked highest for femoral neck improvements.
| Bone Site | Best Exercise Type | Effect Size (SMD) | Key Study |
|---|---|---|---|
| Lumbar Spine | Resistance training | 0.86 – 0.88 | Zhao et al., 2025; Li et al., 2025 |
| Femoral Neck | Combined RT + aerobic | 0.27 – 0.89 | Mohebbi et al., 2023; Zhao et al., 2025 |
| Total Hip | Resistance training | 0.30 – 0.41 | Mohebbi et al., 2023; Zhao et al., 2025 |
What these numbers mean in practical terms: resistance training does not just slow bone loss — it can reverse it. Research in Endocrinology and Metabolism notes that for bones to respond with new tissue formation, they must be exposed to mechanical loads that exceed the forces experienced during daily activities like walking. This is precisely why resistance training outperforms walking and light aerobic exercise for bone density. The loads involved in compound lifts generate the kind of strain that triggers osteogenesis.
The Metabolism Question: Does Muscle Really Burn More Calories?
One of the most repeated claims in fitness is that building muscle "boosts your metabolism." The reality is more nuanced than the typical gym advice suggests, and the research reveals an important distinction between men and women.
The foundational logic is sound: muscle tissue is more metabolically active than fat tissue. Each pound of muscle burns roughly 6 calories per hour at rest compared to about 2 calories for an equivalent amount of fat. So adding lean mass should, in theory, raise your resting metabolic rate.
And some studies support this. Wayne Westcott's review in Current Sports Medicine Reports reported that ten weeks of resistance training could increase resting metabolic rate by approximately 7% while adding 1.4 kg of lean mass and reducing fat weight by 1.8 kg. A randomized controlled trial published in the European Journal of Clinical Nutrition found that nine months of periodized resistance training increased resting metabolic rate by about 5% on average, with individual responses partially explained by changes in fat-free mass and thyroid hormones.
However, a critical nuance emerges when you look specifically at women. A study in Medicine and Science in Sports and Exercise that tracked both men and women through 24 weeks of strength training found a significant gender difference: men saw a 9% increase in resting metabolic rate, while women showed no statistically significant increase. And a randomized controlled trial in older women (ages 65-79) found that neither high-intensity nor low-intensity resistance training significantly altered basal metabolic rate over a full year, despite producing substantial strength gains of 40% in just 15 weeks.

The takeaway: resistance training changes your body composition, shifting it toward more muscle and less fat. But the direct metabolic boost for women may be smaller than the fitness industry claims. The real advantage is indirect: more lean tissue means more calories burned across the whole day, and heavy sessions keep your metabolism elevated for hours afterward.
| Metabolic Claim | What Studies Actually Show |
|---|---|
| "RT boosts metabolism by 7%" | True in mixed-gender studies, but driven primarily by male response |
| "Muscle burns 50 calories per pound per day" | Closer to 6 calories per pound per hour — much lower than commonly cited |
| "RT increases RMR 5% in 9 months" | Supported by RCT data, with wide individual variability |
| "Women see the same RMR boost as men" | Not supported — 24-week study showed no significant increase in women |
Hormones, Hot Flashes, and the Barbell Connection
Most women going through perimenopause or menopause hear about hormone replacement therapy as the primary option. Resistance training works alongside HRT, and for some women, addresses overlapping symptoms through entirely different pathways.
The hot flash data is striking. A systematic review and meta-analysis published in Menopause (2023) examined 12 randomized clinical trials involving 452 postmenopausal women and found that resistance training reduced hot flash frequency dramatically — by a factor of 13 compared to no exercise. When compared directly to aerobic exercise alone, resistance training cut hot flash frequency by 50%. That is not a small difference. Something about loading muscles under heavy resistance changes the hormonal picture in ways that lighter exercise does not.
Several hormonal pathways are involved:
- Insulin sensitivity: Adding resistance training to an exercise program enhances glucose disposal in postmenopausal women, with improvements tied to reductions in both visceral and subcutaneous abdominal fat. Insulin resistance tends to climb during menopause, making this particularly relevant.
- Cortisol regulation: Chronically elevated cortisol drives weight gain and wrecks sleep. Consistent resistance training helps normalize the cortisol response over time.
- Growth hormone: Heavy compound movements trigger growth hormone release, supporting tissue repair and fat metabolism. Both tend to decline during perimenopause.
- Thyroid function: Changes in resting metabolic rate after resistance training correlate with thyroid hormone levels, suggesting training supports rather than suppresses thyroid activity.
The fat loss numbers are worth paying attention to. The same meta-analysis found that resistance training reduced fat mass by 7.80 kg more than aerobic exercise alone in postmenopausal women — which should make anyone reconsider the default advice of "just do more cardio" for weight management during menopause.
Building Your Training Program: What the Evidence Recommends
The research is surprisingly specific about what works. Here are the training parameters with the strongest evidence behind them.
| Parameter | Evidence-Based Recommendation | Source |
|---|---|---|
| Intensity | 70-85% of 1RM for bone density benefits | Zhao et al., 2025 |
| Frequency | 3 sessions per week | Zhao et al., 2025 |
| Session Duration | 40-60 minutes | Zhao et al., 2025 |
| Program Length | 48+ weeks for significant bone changes | Zhao et al., 2025 |
| Exercise Selection | Multi-joint compound movements | Hong & Kim, 2018 |
Start with compound movements. Squats, deadlifts, lunges, overhead presses, rows, and bench presses load multiple joints and large muscle groups simultaneously. These movements generate the highest mechanical forces on bone and recruit the most muscle tissue per exercise.
Progressive overload is non-negotiable. Your body adapts to the stress you place on it. If you lift the same weight at the same rep range week after week, the adaptive stimulus fades. Increasing weight, reps, or sets over time — even in small increments — keeps the bone-building and muscle-building signals active.
Both high and low intensity work — but for different outcomes. Research in women ages 65-79 found that both high-intensity training (80% of 1RM) and low-intensity training (40% of 1RM) produced similar and substantial strength gains over 52 weeks. However, the high-intensity approach showed stronger bone density effects. If your primary goal is bone health, train heavier. If joint limitations prevent heavy loading, lower intensity still delivers meaningful strength improvements.
A sample weekly structure might look like this:
- Day 1 (Lower Body): Barbell squats, Romanian deadlifts, walking lunges, leg press, calf raises
- Day 2 (Upper Body): Bench press, bent-over rows, overhead press, lat pulldown, bicep curls
- Day 3 (Full Body + Core): Deadlifts, push-ups, single-arm rows, goblet squats, planks
Pair this with adequate protein intake — research consistently shows that women over 40 benefit from higher protein consumption (1.2-1.6 g/kg body weight daily) to support muscle protein synthesis, especially when training regularly.

Myths vs. Facts About Women and Weight Training
| Myth | Fact |
|---|---|
| "Lifting heavy will make women bulky" | Women produce roughly 15-20 times less testosterone than men. Building significant muscle mass requires years of dedicated training, caloric surplus, and often pharmacological assistance. Most women who lift heavy develop a lean, defined appearance. |
| "Cardio is better than weights for weight loss" | Resistance training reduces fat mass more effectively than aerobic exercise alone in postmenopausal women. One meta-analysis found RT resulted in 7.80 kg greater fat reduction compared to aerobic training. |
| "You need lighter weights and more reps after 40" | Research shows women ages 65-79 safely performed exercises at 80% of their maximum with 40% strength gains in 15 weeks. Age alone is not a reason to train light. |
| "Walking is enough to protect your bones" | Walking provides minimal mechanical load on bone. Studies show bones need forces exceeding daily activities to trigger new bone formation. Resistance training is significantly more effective for BMD. |
| "Weight training is dangerous for older women" | A meta-analysis of 12 RCTs in postmenopausal women reported zero serious adverse events from resistance training programs. |
Frequently Asked Questions
How many times per week should women over 40 lift weights?
Research supports three sessions per week as optimal for bone density improvements. This frequency was associated with significant improvements at the lumbar spine, femoral neck, total hip, and trochanter in a 2025 meta-analysis of 17 randomized controlled trials. If you are just starting, two sessions per week is sufficient to build foundational strength before progressing.
Can resistance training replace hormone therapy for menopause symptoms?
Resistance training is not a replacement for hormone therapy, but it is a powerful complement. Studies show RT reduces hot flash frequency by up to 50% compared to aerobic exercise alone and improves insulin sensitivity, sleep quality, and mood. For women who cannot or choose not to use HRT, structured resistance training addresses many of the same symptoms through different biological mechanisms.
Is it safe to start lifting weights if you already have osteoporosis?
Yes, with appropriate guidance. A meta-analysis of 80 exercise trials found that the bone-building benefits of exercise were consistent regardless of existing bone status — women with osteopenia or osteoporosis benefited as much as women with normal bone density. Starting with lighter loads and gradually progressing under professional supervision is recommended.
How long does it take to see bone density improvements from resistance training?
Bone remodeling is a slow process. Research indicates that programs lasting 48 weeks or longer produce the most significant bone density changes, particularly at the femoral neck and total hip. Measurable improvements typically require six months to one year of consistent training, though strength and functional improvements appear much sooner — often within the first 10-15 weeks.
Do I need to lift heavy to get bone benefits, or will light weights work?
For bone density specifically, high-intensity training at 70% or more of your one-repetition maximum shows the strongest effects. However, lighter loads still produce meaningful strength gains. A study in women aged 65-79 found that training at 40% of maximum produced strength improvements similar to training at 80%. The best approach is to start at a manageable intensity and progressively increase load over time.
Related Articles
- Perimenopause Symptoms and Natural Management Strategies — A comprehensive look at what happens during the transition years and evidence-based approaches to managing symptoms.
- How Cortisol Drives Weight Gain and What Actually Helps — Understanding the stress hormone that resistance training helps regulate.
- High Protein Diet for Women: How Much You Actually Need — Why protein requirements increase with age and how to meet them for optimal muscle recovery.
- Creatine Benefits Beyond Muscle: Brain, Bone, and Longevity — The supplement that supports both muscle performance and bone density preservation.
- Zone 2 Cardio for Fat Burning and Longevity — How to combine low-intensity cardio with resistance training for comprehensive fitness after 40.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











