
Walk into any peptide forum and ask which growth-hormone secretagogue builds more lean muscle, and you will get two confident answers. The bodybuilder corner says Hexarelin — it is the most potent GH-releaser in the GHRP family. The longevity-clinic corner says Ipamorelin — the cleanest, the safest for long cycles, the one without the cortisol baggage. Both are right about something different. Neither is right about lean muscle. The most honest answer hides in a small body of clinical data: no human trial has ever directly compared these two peptides for lean-mass outcomes, and the only long-term Hexarelin study in healthy adults found zero change in lean body mass after 16 weeks of dosing.
The GHS-Receptor Showdown: Why These Two Peptides Aren't Interchangeable
Imagine the somatotroph cell of your anterior pituitary as a fire alarm with two pull-cord switches. One cord is the GHRH receptor — your body uses it to schedule daily growth-hormone pulses. The other is the GHS-R1a, the so-called ghrelin receptor. Hexarelin and Ipamorelin both yank that second cord. After that, every detail diverges.
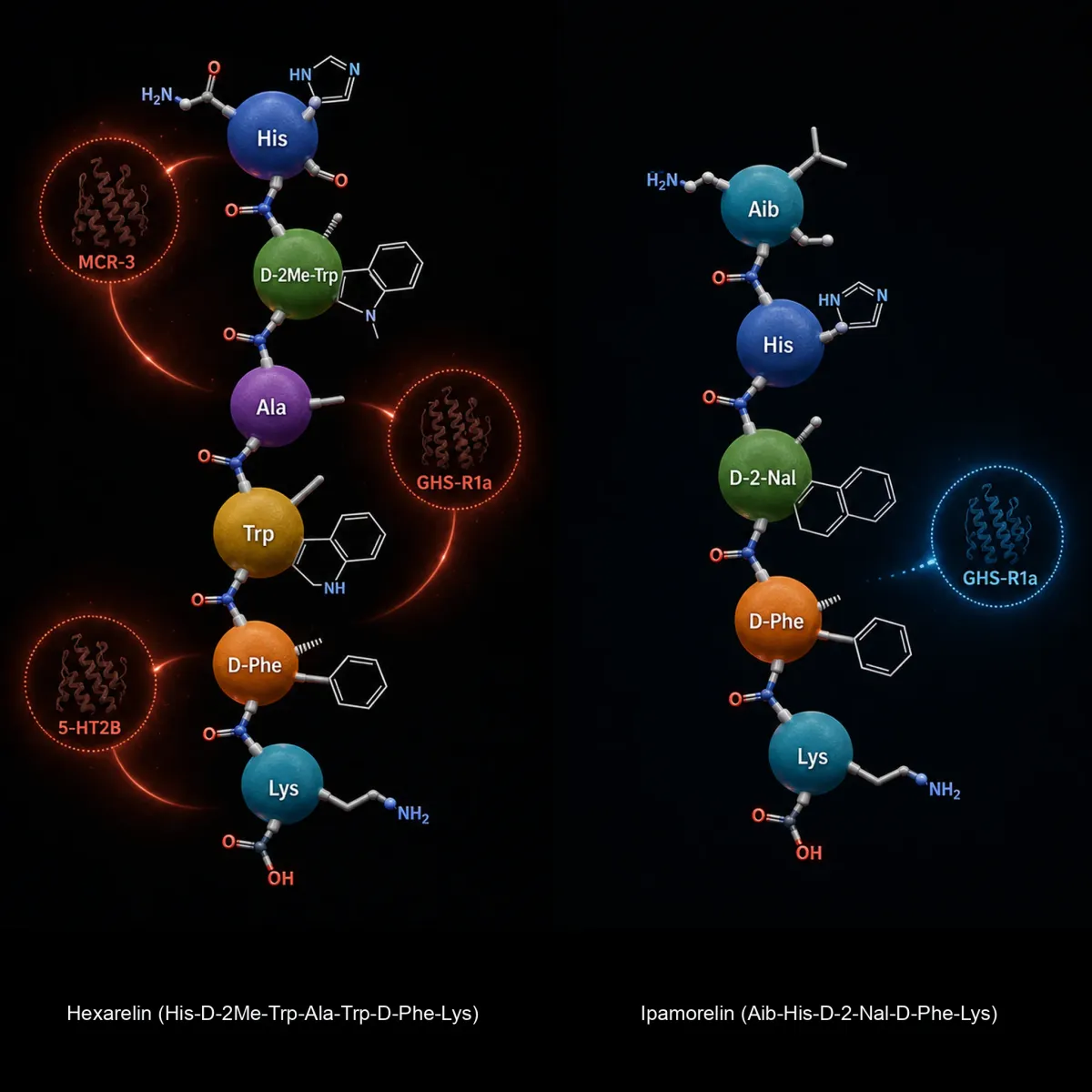
Hexarelin is a hexapeptide — six amino acids — described in Klinger and colleagues' 1996 European Journal of Endocrinology paper as His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH2. Ipamorelin is a pentapeptide, Aib-His-D-2-Nal-D-Phe-Lys-NH2, designed at Novo Nordisk by stripping the central Ala-Trp dipeptide out of GHRP-1 and replacing it with a bridging amino isobutyric acid residue. Karin Raun's team published the discovery paper in 1998. The structural change was not cosmetic — it produced a molecule that binds the same receptor with dramatically different downstream behavior.
In primary rat pituitary cells, Raun's team measured Ipamorelin's EC50 at 1.3 nmol/L versus 2.2 nmol/L for GHRP-6, with similar maximum efficacy. In conscious swine — closer to human GH physiology than a rat — Ipamorelin's ED50 was 2.3 nmol/kg versus 3.9 nmol/kg for GHRP-6. On the GH-release axis alone, these compounds are competitive.
That is not where the story ends. Hexarelin does something Ipamorelin does not: it also binds CD36, a scavenger receptor expressed on cardiomyocytes, vascular endothelium, and fat tissue. The clinical pharmacology literature describes this off-target binding as the molecular signature behind Hexarelin's cardioprotective effects in animal models — effects unrelated to GH release that Ipamorelin, by design, cannot reproduce. The receptor pharmacology already telegraphs the real comparison: not "which one releases more GH," but "what else does each peptide touch on the way out." For someone trying to gain lean muscle, that distinction matters more than the pulse magnitude.
Hexarelin's Knockout Punch: Highest GH Pulse, Steepest Tradeoffs
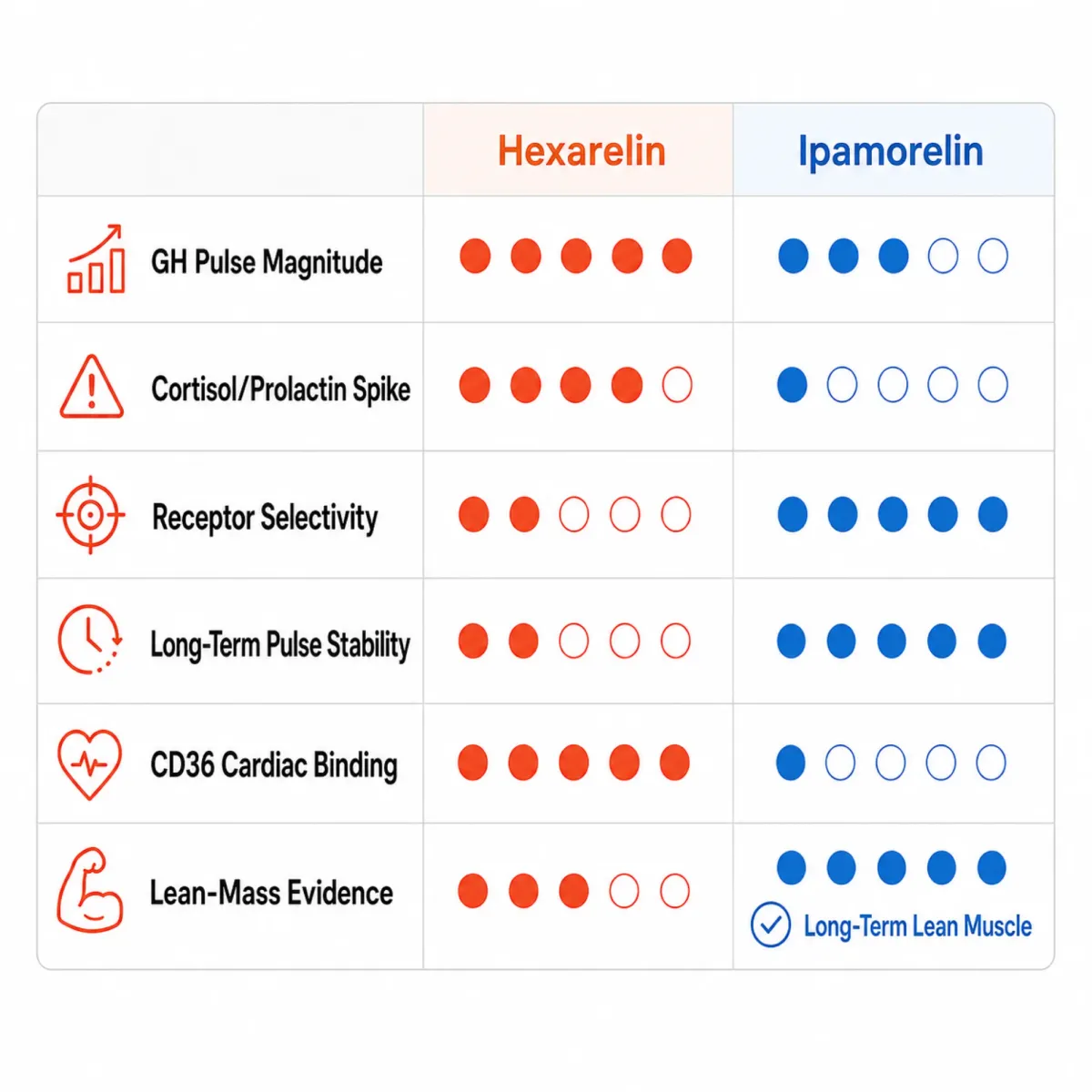
Hexarelin earned its reputation as the heaviest hitter in the GHRP family for a simple reason: pound for pound, the GH pulse it triggers is large, fast, and reproducible. BenchChem's compiled human dose-response data show an ED50 of approximately 0.48 µg/kg, with the GH curve flattening between 1.0 and 2.0 µg/kg. Doubling the dose from 1.0 to 2.0 µg/kg adds only about 6% more GH release. You hit the ceiling fast.
The ceiling has a price tag attached. The cortisol dose-response curve is more linear and more punishing — 0.5 µg/kg produces a significant cortisol response in healthy adults, and prolactin elevation tracks alongside it. ACTH, cortisol, and prolactin rise together because Hexarelin lacks the receptor selectivity Ipamorelin has. Lower-dose protocols at 0.125 to 0.25 µg/kg can elicit a useful pulse with minimal cortisol overshoot, but at that dose Hexarelin loses the very edge that justified using it.
The Hexarelin tradeoff in one line: the dose that produces a meaningful GH pulse in a single injection (~1 µg/kg) is also the dose that drags cortisol and prolactin upward. The dose that avoids the side-effect tax is too small to differentiate Hexarelin from cleaner alternatives.
Half-life compounds the inconvenience. Hexarelin's terminal elimination after IV bolus runs about 55 minutes — long enough for a single training-window pulse, short enough that holding a steady-state effect requires multiple daily injections. Subcutaneous bioavailability is roughly 77%, intranasal about 5%.
Ipamorelin's Quiet Win: Selectivity Without the Side-Effect Tax
The single most quoted finding in the entire growth-hormone-secretagogue literature comes from Raun's 1998 Ipamorelin paper: in conscious swine, Ipamorelin failed to release ACTH or cortisol at levels significantly different from GHRH stimulation. That cleanliness held even at doses more than 200-fold higher than the ED50 for GH release. Two-hundred-fold. Translated to clinic practice, you essentially cannot dose Ipamorelin to a level that triggers the cortisol-prolactin cascade Hexarelin produces at routine doses.
None of the GH secretagogues Raun's team tested — Ipamorelin, GHRP-2, GHRP-6 — affected plasma FSH, LH, prolactin, or TSH at GH-releasing doses. Of those, only Ipamorelin also left ACTH and cortisol alone. That is the clinical signature longevity physicians cite when they treat Ipamorelin as a long-term-tolerable peptide and Hexarelin as a four-week experiment. Ipamorelin's elimination half-life sits around two hours — about double Hexarelin's — giving it a smoother pulse profile that mimics the body's natural GH rhythm rather than overdriving it.
The honest counterweight: Ipamorelin's clinical development pipeline never produced a marketable drug. Novo Nordisk originally developed it, then licensed it to Helsinn Therapeutics, who ran Phase II trials for postoperative ileus before shelving the program for lack of efficacy in that indication. The compound was abandoned because it didn't move the bowel-recovery endpoint, not because of safety. As a side effect, exhaustive multi-year human toxicology data does not exist. Ipamorelin's "safer" reputation is well-earned but not bulletproof — the selectivity is real, the long-term cancer-risk surveillance data is not.
The Lean Mass Question: What the Animal Studies Actually Show
Here is the part of the comparison that bodybuilding forums almost universally get wrong. No peer-reviewed randomized controlled trial has ever directly compared Hexarelin versus Ipamorelin for lean mass in healthy adults. None. Every confident "Hexarelin builds more muscle" or "Ipamorelin recomposes better" claim is extrapolated from animal studies, separate single-arm trials, or forum anecdote.
The animal data favor Ipamorelin in a specific scenario users overlook. Andersen and colleagues in 2001 gave rats a catabolic glucocorticoid alongside daily Ipamorelin. The Ipamorelin arm showed three times more periosteal bone formation than the glucocorticoid-only group while preserving muscle strength. That is a protective signal, not a hypertrophy signal — Ipamorelin prevents catabolic muscle loss under stress; it does not necessarily build new tissue under normal conditions.
The most damning single piece of human evidence comes from Rahim and colleagues' 1998 long-term Hexarelin trial in the Journal of Clinical Endocrinology and Metabolism. Healthy adults received twice-daily subcutaneous Hexarelin at 1.5 µg/kg for sixteen weeks. After the full course, total body fat showed no significant change (P = 0.6), lean body mass showed no significant change (P = 0.3), and bone mineral density showed no significant change (P = 0.3). Sixteen weeks of the most potent GHRP at near-maximum dose did not produce measurable lean-mass changes. The authors concluded that "the biological impact of this hexarelin schedule on the GH-IGF-I axis seems to be minimal" — scientist for "the hypothesis did not pan out."
The contrarian wrinkle on the Ipamorelin side that wellness clinics gloss over: in hypogonadal males and rodent models, Ipamorelin's ghrelin-mimicking activity has stimulated body weight gain and increased adiposity, opposite of the fat-loss recomposition promise. Ghrelin is an appetite signal — stimulate its receptor without caloric restraint and you may gain weight, not lose it.
So if both peptides have weak direct human-RCT evidence for lean mass and the controlled Hexarelin data shows null body-composition effects, where does the comparison settle? On indirect evidence: the integrity of the pulse over time.
Cycling, Desensitization, and Why Hexarelin Stops Working
Cycle planning is where the practical case for Ipamorelin gets sharpest, because Hexarelin has a documented problem the bodybuilding community discovered the hard way: the receptor stops responding.
Pull the same data from Rahim's 1998 long-term Hexarelin trial. The mean area under the GH curve at baseline was 19.1 µg/L per hour. After one week of dosing, it had already dropped to 13.1. By week 4, it was 12.3. By week 16, it sat at 10.5 — a roughly 45% reduction in the GH pulse the same dose of Hexarelin could produce, with the change reaching statistical significance at P < 0.01. Four weeks after stopping the peptide entirely, AUC GH had recovered to 19.4 — essentially identical to baseline. The desensitization was real, dose-related, and reversible.
The pediatric data tell the same story from a different angle. Klinger and colleagues in 1996 gave seven prepubertal short children intranasal Hexarelin at 60 µg/kg three times a day for six to ten months. Pretreatment hGH peak response to a test dose was 70.6 mU/L. After just seven days of dosing, peak response had dropped to 34.1 mU/L — more than half — and stabilized at around 37.5 mU/L for the duration of the six-month treatment. Three months after stopping, response recovered to 42.1 mU/L. Despite that desensitization, growth velocity in those children rose significantly, from 5.3 cm per year to 7.4 cm per year. Hexarelin's biological end-effect held up even when the apparent pulse magnitude tanked — which is why the authors framed it as "partial desensitization that does not interfere with biological effects."
The pediatric framing cuts both ways. For lean-mass-seeking adults, body-composition signals are far less sensitive than linear growth in pre-pubertal children. The Rahim adult trial that measured lean body mass directly found nothing — partial desensitization plus modest GH-IGF-1 stimulation produced no measurable lean tissue change at 16 weeks.
Ipamorelin behaves differently in real-world cycle reports. Its gentler pulse places less internalization pressure on the GHS-R1a. Practical cycling guides recommend 200 to 300 mcg per injection, dosed once to three times daily, for 6 to 12 week cycles with 4-week rest periods. 300 mcg is the per-injection plateau — exceeding it provides no additional GH release because the receptor saturates.
For a multi-month protocol, the implication is direct: Hexarelin's response curve slopes downward from week one. Ipamorelin's curve stays flatter through typical 8-to-12-week cycles. If your goal is sustained GH-IGF-1 axis stimulation, the peptide that does not erode under its own dosing is the one that will end the cycle still working.
Cardiac Side Effects vs. Cardiac Protection: A Tale of Two Peptides
Hexarelin has one genuinely impressive corner of its evidence base, and it has nothing to do with lean muscle. Rossoni and colleagues' 2000 study in Pharmacological Research: rats given Hexarelin at 80 µg/kg subcutaneously for seven days had hearts that resisted ventricular dysfunction induced by calcium-paradox injury. Recovery of left ventricular developed pressure was twice that of controls. Creatine kinase release was reduced by 40% (P < 0.001).
The mechanism is the punchline. Plasma and heart IGF-1 in Hexarelin-treated rats were identical to controls. The cardioprotection was independent of the GH/IGF-1 axis — Hexarelin was acting on the heart directly. Subsequent receptor pharmacology placed the explanation on Hexarelin's binding to CD36 on cardiomyocytes and vascular endothelium, a receptor Ipamorelin doesn't engage.
That is real, replicable mechanistic data — in rats. There is no equivalent randomized human trial showing Hexarelin-driven cardioprotection in patients with heart failure, post-MI status, or pre-bypass risk. The CD36 story produced mechanistic interest but no approved cardiac indication.
Acutely, the same molecule drags cortisol up at routine GH-releasing doses, which is not a desirable trait for the populations you'd otherwise want to protect. For a body-composition user, the cardiac story is a tiebreaker that doesn't break the tie — it answers a different question than "what builds lean mass."
The Verdict for Lean Muscle: Why Most Long-Term Users Land on Ipamorelin
The most defensible head-to-head answer for lean muscle has nothing to do with peak pulse magnitude. It comes from three observations.
First, the only long-term human Hexarelin trial that measured body composition directly found no significant change in lean body mass after 16 weeks (P = 0.3) — the closest thing to a definitive human verdict on chronic Hexarelin recomposition. The verdict is null.
Second, Hexarelin's response curve flattens within weeks. Even granting that high-pulse GH spikes drive hypertrophy in a way the Rahim trial missed, Hexarelin loses the very property — large-amplitude pulse — you would be paying the cortisol tax to obtain. Ipamorelin's pulse is smaller acutely but holds over the multi-month cycles real body-composition change requires.
Third, the practical synergy bodybuilding clinics spent fifteen years optimizing favors Ipamorelin. Co-administered with a GHRH analog like CJC-1295, both peptides produce synergistic GH release greater than either alone — but Ipamorelin's clean pulse layered on CJC-1295's prolonged signal mimics physiologic GH release more faithfully than the spiky Hexarelin alternative. CJC-1295 + Ipamorelin protocols (detailed in our companion article on the CJC-1295 and Ipamorelin stack) settle on 100 to 200 mcg of CJC-1295 with 200 to 300 mcg of Ipamorelin, twice daily, in 8 to 12 week cycles.
The honest counterpoint comes from Rahim's 1999 cortisol-axis paper: after 16 weeks of twice-daily Hexarelin at 1.5 µg/kg, the area under the cortisol curve had decreased from 1506 to 1222 nmol/L per hour (P = 0.008), then rebounded to 1586 four weeks after stopping. That is not a license for chronic use — it's evidence the pituitary-adrenal axis adapts by partially shutting down, exactly the same desensitization mechanism dragging the GH response down. The body produces less of everything in response to repeated overstimulation.
For a healthy adult choosing the workhorse of a 12-week recomposition cycle, the evidence-aligned answer is Ipamorelin, ideally stacked with CJC-1295 to amplify pulse amplitude without the cortisol cost. Hexarelin earns a narrow niche: short experiments of four weeks or less, mostly for users with a specific interest in engaging CD36 — and that interest, in 2026, is research curiosity, not lean-muscle outcomes.
The question "which one wins for lean muscle" was quietly answered decades ago by the failure of every direct human trial to show meaningful body-composition gains from any GHRP-class peptide alone. Lean mass comes from training, calories, protein, and adequate IGF-1 baseline. The peptides modulate that system — they don't replace it. The one that modulates cleanly and consistently for the full cycle is the one worth using.
Frequently Asked Questions
Is Hexarelin stronger than Ipamorelin for GH release?
On a single-dose basis in humans, yes — Hexarelin produces a larger absolute GH pulse at around 1 µg/kg. But the difference shrinks fast: the curve plateaus by 1.0 to 2.0 µg/kg, and chronic dosing erodes the response by roughly 45% within sixteen weeks. Ipamorelin's smaller per-injection pulse holds steadier across multi-month cycles, which is what matters for body composition.
Does Hexarelin cause permanent receptor desensitization?
No. The desensitization in Rahim's 1998 trial was partial — about a 45% drop at week 16 — and fully reversible within four weeks of stopping. Klinger's 1996 pediatric data showed the same pattern: response dropped sharply within a week, recovered three months after cessation. Hexarelin loses effectiveness during the cycle, then comes back.
Can you stack Hexarelin with CJC-1295 instead of Ipamorelin?
Mechanistically yes, both peptides synergize with GHRH analogs. In practice, almost no clinic builds CJC-1295 + Hexarelin protocols because Hexarelin's cortisol and prolactin elevation plus desensitization cancel the smooth physiologic-pulse advantage CJC-1295 provides. CJC-1295 + Ipamorelin remains dominant because the components match each other's profile.
Why do bodybuilding forums still recommend Hexarelin?
Two reasons. First, the acute GH pulse is large and feels noticeable — users report a flush, hunger, and post-injection grogginess they interpret as proof the compound is working. Second, short cycles of four weeks or less avoid the worst desensitization decay. For a quick experiment, Hexarelin produces measurable acute effects; for a 12-week recomposition cycle, those effects mostly disappear by week three or four.
Is Ipamorelin actually safe long-term?
The mechanistic safety profile is strong — no significant ACTH, cortisol, prolactin, FSH, LH, or TSH effects even at 200 times the GH-releasing dose. The caveat is that exhaustive multi-year human toxicology data does not exist because Novo Nordisk and Helsinn shelved the molecule after Phase II ileus trials failed. Clinic prescribing rests on the selectivity profile plus a generation of off-label use without major reported events. "Long-term safe" remains a reasonable working assumption rather than a documented certainty.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











