If you have IBS, you already know that food can feel unpredictable. One meal feels fine, the next brings bloating, cramps, urgency, or a full day of discomfort. The low-FODMAP diet is one of the best-studied nutrition tools for IBS symptom control, but many guides are too vague to use in real life.
This guide is different. You will get a practical, step-by-step system you can use at home: what to do first, what to eat during elimination, exactly how to reintroduce foods, and how to avoid staying on an over-restrictive diet. We will keep this evidence-based and realistic, drawing on major gastroenterology guidance from the American College of Gastroenterology, the American Gastroenterological Association, and public guidance from NIDDK and NICE.
If you also want to support your broader gut strategy, pair this process with a bigger-picture plan on microbiome habits, sleep, and stress using our guide to gut health personalization and microbiome testing. Think of low-FODMAP as a diagnostic nutrition experiment, not a permanent food identity.
Quick reality check: low-FODMAP is not meant to be strict forever. The goal is short-term symptom control, then careful reintroduction and personalization so your diet stays varied.
Why the low-FODMAP approach helps many people with IBS
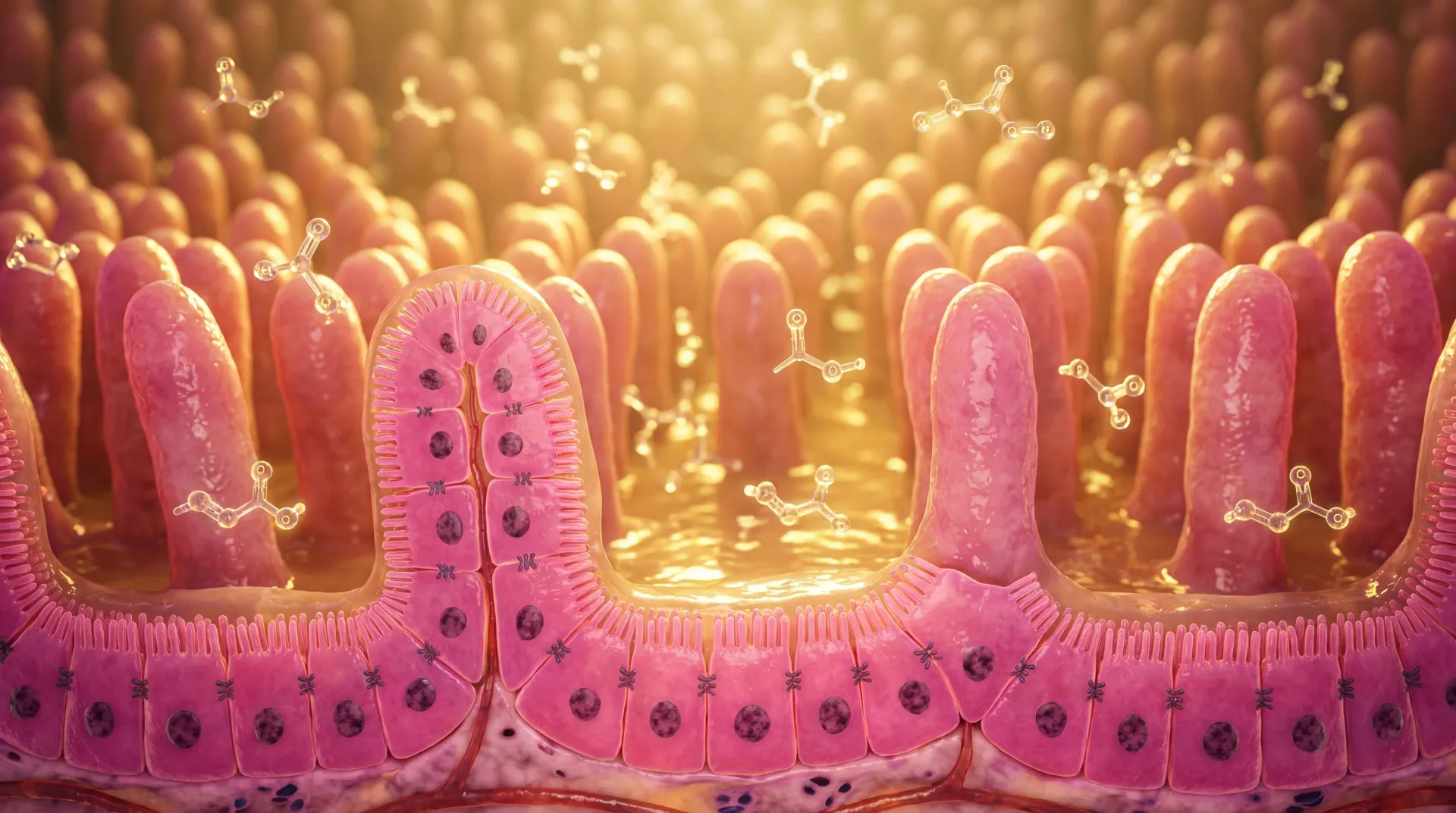
FODMAP stands for fermentable oligosaccharides, disaccharides, monosaccharides, and polyols. These are short-chain carbohydrates that can be poorly absorbed in the small intestine. In susceptible people, they draw water into the gut and ferment quickly in the colon, which can increase gas and distension. For someone with IBS and visceral hypersensitivity, that can translate into pain, bloating, altered stool patterns, and urgency.
The most important point is this: FODMAP foods are not "bad" foods. Many are nutritious. The issue is dose and individual tolerance. Two people with IBS can react differently to the same meal, and the same person can tolerate different amounts depending on stress, sleep, menstrual cycle timing, and meal composition.
Evidence quality is strong enough that major GI organizations include this pattern in IBS management. The ACG guideline recommends a limited trial of a low-FODMAP diet to improve global symptoms, and multiple meta-analyses report meaningful symptom improvement in many patients with IBS. A 2021 systematic review and meta-analysis found low-FODMAP approaches improved global symptoms compared with control diets in several studies (Frontiers in Nutrition review).
In a controlled trial comparing low-FODMAP and modified NICE dietary advice, both helped, while low-FODMAP delivered larger improvements for some symptom domains (Bohn et al., Gastroenterology). That is why the best practical question is usually not "Does it work perfectly for everyone?" but "How do I run it correctly, then keep only what helps me?"
| FODMAP Group | Common Examples | Typical IBS Trigger Pattern | Lower-FODMAP Alternatives |
|---|---|---|---|
| Fructans | Wheat breads, onion, garlic | Bloating and gas after savory meals | Rice, oats, sourdough spelt portions, garlic-infused oil |
| Galacto-oligosaccharides (GOS) | Beans, chickpeas, lentils (large portions) | Gas and abdominal pressure | Canned/rinsed legumes in small serves, tofu, tempeh |
| Lactose | Milk, soft cheeses, ice cream | Urgency, bloating, loose stool in lactose-sensitive people | Lactose-free milk, hard cheeses, lactose-free yogurt |
| Excess Fructose | Honey, apples, mango, high-fructose corn syrup | Bloating and stool changes when intake is high | Kiwi, berries, citrus, maple syrup |
| Polyols | Sorbitol/mannitol sweeteners, stone fruits, mushrooms | Gas, cramping, laxative-like stool effects | Table sugar in moderate amounts, grapes, carrots, spinach |
One practical tip from day one: keep your expectations realistic. Low-FODMAP is a symptom-management framework, not a cure for IBS. You are looking for trend-level improvement over 2-6 weeks, not perfection after 48 hours.
Before you start: diagnosis, red flags, and setup
Before elimination, make sure you are solving the right problem. IBS is a clinical diagnosis with specific criteria, but not every digestive symptom is IBS. The ACG guideline emphasizes targeted evaluation and ruling out key alternative diagnoses when appropriate, especially in IBS with diarrhea. Your clinician may evaluate for celiac disease, inflammatory bowel disease signs, or other causes based on your symptom profile and age.
Red flags that need medical review before self-directed diet trials include rectal bleeding, unexplained weight loss, iron-deficiency anemia, fever, nighttime symptoms that wake you, severe progressive pain, family history of colorectal cancer or IBD, or symptom onset later in life. If any of those apply, pause and get a clinical workup first.
Next, define your baseline. If you skip this step, you cannot tell whether the diet is helping. For 7 days, track:
- Meal times and core foods
- Bloating severity (0-10)
- Pain severity (0-10)
- Stool frequency and stool form
- Urgency episodes
- Sleep duration and stress level
This baseline lets you compare "before versus after" and avoid placebo-driven guesswork. It also helps your clinician or dietitian spot non-food drivers. The AGA clinical update highlights that structured counseling and quality implementation matter as much as the food list itself.
Set your kitchen up for success before day 1:
- Build a 10-12 item repeatable grocery list
- Plan 3 breakfasts, 3 lunches, and 4 dinners you can rotate
- Choose one symptom-tracking tool (notes app, spreadsheet, paper)
- Remove obvious high-polyol sweeteners from your home and work bag
- Add emergency low-FODMAP snacks for commute and travel days
| Pre-Start Task | Why It Matters | Time Required |
|---|---|---|
| 7-day baseline symptom log | Creates objective comparison for response | 5 minutes per day |
| Meal rotation template | Reduces decision fatigue and accidental triggers | 45-60 minutes once |
| Kitchen reset | Makes adherence easier during busy weekdays | 30-45 minutes |
| Clinician check for red flags | Avoids masking serious conditions | As needed |
If digestive symptoms overlap with other sensitivities, it can help to compare patterns with our article on allergies vs food sensitivities so you do not mislabel every reaction as a FODMAP issue.
Phase 1: a practical 2-6 week elimination process
During elimination, your goal is symptom stabilization, not long-term restriction. Most expert protocols use around 2-6 weeks, then move to reintroduction rather than extending strict elimination indefinitely. Monash guidance and GI dietetic practice both emphasize this time-limited approach because prolonged restriction can reduce diet variety and potentially affect microbiota exposure.
What to eat is easier when you think in meal templates instead of individual forbidden foods:
- Protein anchor: eggs, chicken, fish, tofu, tempeh, lean beef
- Carb base: rice, quinoa, oats, potatoes, suitable sourdough portions
- Vegetable pair: zucchini, carrots, spinach, bell peppers, tomatoes
- Flavor strategy: herbs, citrus, ginger, garlic-infused oil, scallion greens
- Dairy strategy: lactose-free milk and yogurt, hard cheese portions
Most adherence problems come from sauces, snacks, and weekend social eating, not from dinner proteins. Read labels for onion/garlic powders, inulin/chicory root fiber, concentrated apple/pear juices, and sugar alcohols (sorbitol, mannitol, xylitol, maltitol). If you use reduced-sugar products often, review hidden sweeteners and compare with our breakdown of artificial sweeteners: benefits and risks.
| Meal Type | Simple Low-FODMAP Build | High-Risk Add-On to Watch |
|---|---|---|
| Breakfast | Overnight oats with chia, kiwi, lactose-free yogurt | Honey-heavy granola or apple concentrate |
| Lunch | Rice bowl with grilled chicken, spinach, cucumber, olive oil | Onion-garlic dressing or wheat croutons |
| Dinner | Salmon, roasted potatoes, carrots, zucchini, herb sauce | Large garlic/onion sauces and high-fructose marinades |
| Snacks | Firm banana, walnuts, lactose-free kefir, rice cakes | Polyol sweeteners in "sugar-free" products |
At the end of week 2, look for trend shifts:
- Lower average bloating score
- Fewer urgency episodes
- More predictable stool pattern
- Reduced pain intensity or shorter flare duration
If there is no meaningful improvement by week 4 despite good adherence, do not force it endlessly. Re-check diagnosis, medication factors, stress load, constipation management, and fiber strategy. NICE and AGA both position diet as one part of IBS care, not a standalone solution for every case.
Phase 2: reintroduction to identify your true triggers
Reintroduction is where low-FODMAP becomes truly useful. Skipping this phase leaves you with an unnecessarily narrow diet and no clear map of what actually bothers you. The mission is to challenge one FODMAP group at a time, in rising doses, while keeping everything else stable.
Use a structured ladder for each challenge:
- Choose one FODMAP group to test (for example lactose).
- Day 1: small dose of a representative food.
- Day 2: medium dose if day 1 is tolerated.
- Day 3: larger dose if day 2 is tolerated.
- Washout for 2-3 days before the next group.
Record symptoms each day and classify each group as:
- Tolerated: minimal or no symptom change
- Dose-dependent: okay at small doses, not at larger doses
- Poorly tolerated: clear symptom flare at low dose
A practical detail many people miss: challenge foods should be "clean" examples of one group when possible. Testing garlic bread, for example, mixes fructans, wheat, fat load, and portion effects all at once. Better to test with one clear food in a controlled portion.
| FODMAP Group | Example Challenge Food | Day 1 | Day 2 | Day 3 |
|---|---|---|---|---|
| Lactose | Regular milk | 1/4 cup | 1/2 cup | 1 cup |
| Excess Fructose | Honey | 1 teaspoon | 2 teaspoons | 1 tablespoon |
| Fructans (grain) | Wheat pasta | 1/2 cup cooked | 1 cup cooked | 1.5 cups cooked |
| Fructans (vegetable) | Cooked onion | 1 tablespoon | 2 tablespoons | 1/4 cup |
| GOS | Chickpeas | 1 tablespoon | 1/4 cup | 1/2 cup |
| Polyols (sorbitol) | Blackberries | 2 berries | 5 berries | 10 berries |
How long should this phase take? Usually 6-10 weeks if done carefully. This seems long, but the output is valuable: a personalized tolerance map you can use for years. Long-term follow-up research shows that most people can liberalize substantially after structured reintroduction, rather than staying fully restricted (Whelan et al. follow-up data).
If you are unsure where fermented foods or probiotics fit, build them in only after core triggers are mapped. Then review strain-specific guidance in our article on probiotic strains and species and our broader evidence-based probiotics guide.
Phase 3: personalization for long-term eating freedom
Personalization is the end goal. Once you know your thresholds, you rebuild a varied diet around what you tolerate. This protects nutrition quality, social flexibility, and food enjoyment.
A useful framework is "safe base + strategic challenge":
- Keep your reliable base meals for high-pressure days
- Use your challenge map to expand choices on lower-stress days
- Treat tolerance as dose-dependent, not all-or-nothing
- Retest previously problematic groups every few months
Why retest? Tolerance can shift over time with stress management, bowel habit stabilization, and changes in meal context. Emerging evidence also highlights the microbiome tradeoffs of prolonged broad FODMAP restriction, which is one reason experts advocate re-expansion when possible (Staudacher et al. review on microbiota implications).
Nutrition quality matters here. A narrow long-term diet can lower fiber diversity and reduce intake of key micronutrients if not planned. Keep a "minimum diversity target" each week: several fruit options, multiple vegetables, at least two whole-grain sources you tolerate, and regular protein variety.
| Personalization Goal | Weekly Target | How to Track It |
|---|---|---|
| Fiber diversity | 8-12 different plant foods you tolerate | Simple checklist on phone notes |
| Symptom stability | Bloating and pain mostly in mild range | 3-day moving average symptom score |
| Diet flexibility | At least 2 social meals managed without major flare | Post-meal reflection: trigger, dose, context |
| Re-expansion | Retest 1 previously limited food every 2-4 weeks | Use same challenge ladder format |
A practical 14-day action plan you can actually follow
Use this two-week sprint to move from confusion to control. It is intentionally simple and repeatable.
| Day Range | Main Focus | What Success Looks Like |
|---|---|---|
| Days 1-3 | Kitchen setup and baseline logging | You have a repeatable meal rotation and symptom baseline |
| Days 4-7 | Strict elimination consistency | Fewer random trigger exposures from sauces/snacks |
| Days 8-10 | Refine portions and timing | More predictable symptom pattern across weekdays |
| Days 11-14 | Assess trend and prepare reintroduction plan | Clear decision: continue to week 4 or pivot strategy |
Daily checklist during this sprint:
- Eat from your planned template at least 80 percent of the time
- Hydrate consistently and avoid very large late-night meals
- Keep caffeine and alcohol patterns stable while testing food effects
- Log symptoms once in the afternoon and once before bed
- Do not add multiple new supplements during elimination
At the day-14 mark, compare averages versus baseline. If symptoms are clearly better, continue elimination up to a total of 4-6 weeks, then begin structured reintroduction. If no clear benefit appears, reassess with your clinician rather than extending strict restriction indefinitely.
Common mistakes, myths, and troubleshooting
Myth 1: "Low-FODMAP means no carbs." False. The plan modifies fermentable carbohydrate sources; it does not require a no-carb diet.
Myth 2: "If a food triggered me once, I must avoid it forever." Often false. Many triggers are dose-dependent and context-dependent. Re-testing is part of personalization.
Myth 3: "If symptoms improve, I should stay in elimination forever." Not recommended. Long-term strict restriction can reduce diet diversity and may negatively affect microbiota patterns, which is why reintroduction is essential.
Myth 4: "More restriction always means better symptom control." Usually false. Over-restriction increases stress and social burden and can paradoxically worsen symptom vigilance.
Troubleshooting if symptoms persist despite good adherence:
- Check constipation management and stool regularity first
- Audit hidden FODMAP exposures in condiments and supplements
- Review meal size and fat load, not only ingredient lists
- Assess stress/sleep triggers that amplify gut sensitivity
- Consider formal dietitian support for protocol accuracy
Also remember overlap conditions. Some people with IBS symptoms have additional factors such as pelvic floor dysfunction, reflux, small intestinal bacterial overgrowth patterns, bile acid diarrhea, or gynecologic contributors. Diet helps many cases, but persistent severe symptoms need broader evaluation.
If you want to keep your strategy practical, think in tiers:
- Tier 1: high-confidence personal triggers you limit regularly
- Tier 2: dose-dependent foods you use with portion control
- Tier 3: tolerated foods you can eat freely
This tier approach gives structure without fear-based eating and is often easier to maintain than a strict yes/no list.
Frequently Asked Questions
How long should I stay in the elimination phase?
Most people use 2-6 weeks, with reassessment around week 2 and week 4. If you see no meaningful trend improvement by week 4 despite solid adherence, continuing strict elimination is usually low value and should be re-evaluated with a clinician or dietitian.
Can I do low-FODMAP without a dietitian?
You can start on your own, but outcomes are often better with professional guidance, especially for reintroduction and long-term personalization. A dietitian can help you avoid unnecessary restriction and protect nutrition quality while still controlling symptoms.
Do I need to avoid gluten on a low-FODMAP diet?
Not automatically. Many people reduce wheat because of fructans, not gluten itself. Unless you have celiac disease or confirmed non-celiac wheat sensitivity, the target is FODMAP load and personal tolerance, not blanket gluten elimination.
What if my symptoms get worse during reintroduction?
Pause that challenge, return to your stable baseline for a few days, then continue with a smaller dose or a different representative food in the same FODMAP group. A flare during one challenge does not mean the whole protocol failed; it often gives useful dose-threshold information.
Can probiotics replace a low-FODMAP strategy?
Not usually. They can complement care in selected cases, but they do not map your personal food trigger thresholds. Use low-FODMAP phases to identify tolerances, then consider targeted probiotic strategies if appropriate for your symptom pattern and clinical guidance.
Related Articles
- Gut Health Personalization and Microbiome Testing Guide - Learn how stool patterns, lifestyle habits, and testing choices can support smarter gut decisions.
- Health Benefits of Probiotics: An Evidence-Based Ultimate Guide - Understand where probiotics can help, where they are overhyped, and how to evaluate labels.
- Probiotic Strains and Species - Compare strain-level evidence and practical use cases for digestion-focused goals.
- Allergies vs Food Sensitivities - Separate immune allergy signals from non-allergic food reactions and improve your symptom detective work.
- Artificial Sweeteners: Benefits, Risks, and Best Uses - Review sweetener tradeoffs and hidden ingredients that can affect digestive tolerance.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.