
What Is Inositol and Why Are Researchers Paying Attention?
Your body already makes inositol. Your kidneys produce roughly 2 grams per day, and the food you eat — citrus fruits, beans, whole grains, nuts — contributes another 0.5 to 1 gram on top of that. Despite sometimes being labeled "vitamin B8," inositol is not technically a vitamin at all. It is a six-carbon sugar alcohol that your cells use as a structural building block and, more importantly, as a chemical messenger.
Inositol sits inside cell membranes as phosphatidylinositol, where it helps relay signals from hormones like insulin, follicle-stimulating hormone (FSH), and thyroid-stimulating hormone. When insulin binds to a cell receptor, inositol-derived compounds carry that signal inward, telling the cell to open glucose transporters and pull sugar out of the bloodstream. When FSH reaches a follicle in the ovary, inositol mediates the downstream response that drives egg maturation.
Nine different structural forms (stereoisomers) of inositol exist, but two dominate the research: myo-inositol (MI) and D-chiro-inositol (DCI). They are not interchangeable. An enzyme called epimerase converts MI to DCI inside your tissues, and the ratio between them varies dramatically depending on where you are in the body — roughly 40:1 in blood plasma, but as high as 100:1 in healthy ovarian follicular fluid. When that ratio gets disrupted — which happens in insulin resistance — the consequences ripple outward into hormone production, ovulation, mood regulation, and metabolic health.
This is not a fringe supplement riding a social media wave. Over the past decade, inositol has accumulated a serious body of clinical trial evidence, including multiple systematic reviews and meta-analyses involving thousands of participants. The research concentrates in three areas: polycystic ovary syndrome, anxiety-spectrum disorders, and broader metabolic dysfunction.
The Two Forms That Changed How Clinicians Approach PCOS
Polycystic ovary syndrome affects between 5 and 20 percent of women during their reproductive years, depending on which diagnostic criteria you apply. The condition is not simply an ovarian problem. Insulin resistance drives it, which shows up in roughly 75 percent of lean women with PCOS and up to 95 percent of those who are overweight. That insulin resistance creates a hormonal cascade: excess insulin suppresses sex hormone-binding globulin (SHBG), leaving more free testosterone circulating. Simultaneously, hyperinsulinemia pushes ovarian theca cells to overproduce androgens. The result is the cluster of symptoms — irregular cycles, acne, excess hair growth, difficulty conceiving — that defines the condition.
Metformin has long been the standard insulin-sensitizing treatment for PCOS. It works, but it comes with a cost. The largest meta-analysis on inositol for PCOS — 26 randomized controlled trials covering 1,691 women — found that inositol matched metformin's effectiveness across most outcomes while producing dramatically fewer side effects: 7 percent with inositol versus 53 percent with metformin. That difference is not subtle. More than half of women on metformin reported bloating, nausea, or generalized weakness.
Here is what that same meta-analysis found when comparing inositol to placebo:
| Outcome | Effect vs Placebo | Statistical Significance |
|---|---|---|
| Menstrual cycle normalization | 1.79x more likely | P < 0.05 |
| Free testosterone | −0.41 ng/dL | P < 0.05 |
| Total testosterone | −20.39 ng/dL | P < 0.05 |
| BMI | −0.45 kg/m² | P < 0.05 |
| Fasting glucose | −3.14 mg/dL | P < 0.05 |
| SHBG | +32.06 nmol/L | P < 0.05 |
| AUC insulin | −2,081.05 µU/mL/min | P < 0.05 |
A separate, earlier meta-analysis of nine RCTs confirmed the insulin findings specifically: fasting insulin dropped significantly (SMD = −1.021, P = 0.009), and HOMA index — a standard measure of insulin resistance — also improved (SMD = −0.585, P = 0.041). Trial sequential analysis validated these results were not statistical flukes. Notably, improvements in SHBG only became significant in studies lasting 24 weeks or longer, suggesting that some hormonal benefits require patience to materialize.
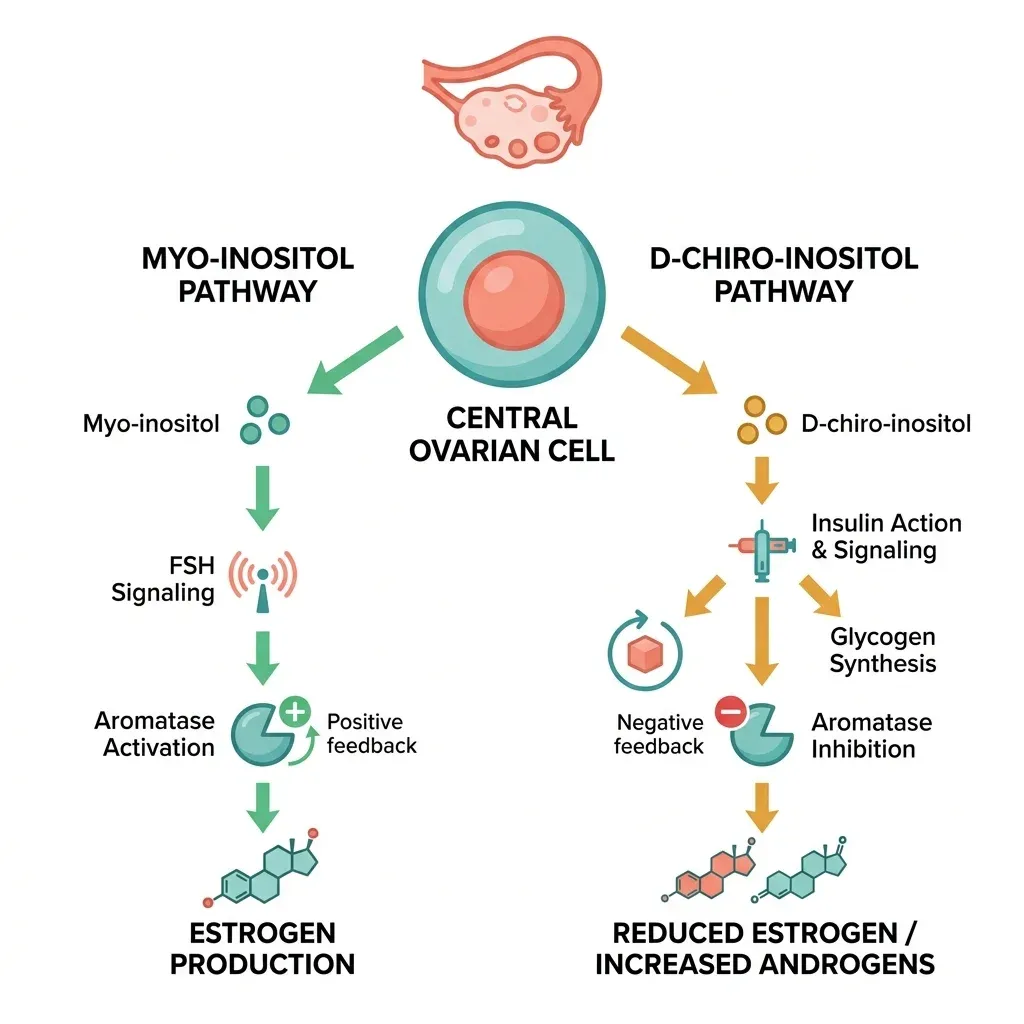
The critical detail: MI and DCI do opposite things inside the ovary. Myo-inositol enhances aromatase (the enzyme converting androgens to estrogens) and supports FSH signaling. D-chiro-inositol inhibits aromatase and can increase testosterone production in theca cells. This means high DCI doses can actually worsen PCOS symptoms — a finding confirmed in both animal and human studies.
A mouse model study testing multiple MI:DCI ratios found that only the 40:1 molar ratio achieved fast and nearly complete recovery from PCOS signs. Formulations with higher DCI content worsened pathological features. This matters because commercial supplements vary wildly in their ratios — from 0.4:1 all the way to 104:1 — and many consumers have no idea they may be taking a formulation that works against them.
In clinical practice, MI at 2 grams daily restored menstrual cycles in 88 percent of PCOS women within about 35 days. Among those who regained regular cycles, spontaneous ovulation followed in most cases. DCI at 1,200 mg daily for eight weeks reduced insulin area under the curve by 62 percent and free testosterone by 55 percent, with 86 percent of recipients ovulating compared to 27 percent on placebo.
Can a Sugar Molecule Calm Your Nervous System?
The psychiatric research on inositol predates the PCOS work by several years, and it follows a different line of reasoning entirely. In the brain, myo-inositol feeds into the phosphatidylinositol signaling system — a second-messenger pathway linked to serotonergic, cholinergic, and noradrenergic receptor systems. The hypothesis, first proposed in the 1990s, was straightforward: if inositol depletion disrupts these signaling cascades, then supplementing with inositol might restore them.
The most compelling evidence comes from panic disorder research. In a double-blind, placebo-controlled crossover trial, 21 patients with panic disorder received 12 grams of inositol daily for four weeks. Both the frequency and severity of panic attacks declined significantly compared to placebo, with minimal side effects. A subsequent head-to-head crossover trial pitted inositol directly against fluvoxamine (an SSRI commonly prescribed for panic disorder). Twenty patients received up to 18 grams of inositol daily for one month, then switched to fluvoxamine (up to 150 mg daily) for another month, or vice versa. Inositol reduced weekly panic attacks by an average of 4.0 compared to fluvoxamine's reduction of 2.4 (P = 0.049). Meanwhile, nausea and fatigue were significantly more common with fluvoxamine.
The researcher behind both of these trials, Joseph Levine, also tested inositol against depression and obsessive-compulsive disorder. The depression trial (28 patients) showed significant improvement at week four on the Hamilton Depression Scale. The OCD trial (13 patients) found meaningful symptom reduction. Importantly, inositol showed no benefit for schizophrenia, Alzheimer's disease, ADHD, or autism — conditions that do not respond to serotonin reuptake inhibitors. This selectivity supports the idea that inositol's psychiatric effects operate through serotonin-related pathways rather than some nonspecific mechanism.
A 2014 meta-analysis attempted to pool the available anxiety and depression data from double-blind RCTs. The results were mixed: the overall analysis did not reach statistical significance, partly because the total sample sizes were small (242 patients across seven depression trials, 70 across four anxiety trials). However, there was a marginal trend toward benefit for depression (P = 0.06) and a stronger signal for premenstrual dysphoric disorder specifically (P = 0.07). The authors concluded that inositol "may be beneficial for depressed patients, especially those with PMDD."
That PMDD finding matters for the hormonal balance picture. PMDD affects women during the luteal phase of their menstrual cycle, when progesterone rises and inositol-mediated signaling may be particularly relevant. For women dealing with both PCOS and mood symptoms, inositol sits at an unusual intersection: it may address the metabolic roots of their hormonal dysfunction while simultaneously influencing the neurotransmitter systems tied to their anxiety and mood disturbances.
Metabolic Ripple Effects: Blood Sugar, Cholesterol, and Blood Pressure
The benefits of inositol extend beyond reproductive hormones and brain chemistry. A 2025 meta-analysis of 18 randomized controlled trials (898 participants) examined inositol's cardiometabolic effects and found improvements across nearly every marker tested:
| Marker | Change | Evidence Certainty |
|---|---|---|
| Fasting insulin | −4.74 µU/mL | Moderate |
| HOMA-IR | −1.21 | Moderate |
| Triglycerides | −29.80 mg/dL | High |
| Total cholesterol | −18.26 mg/dL | Low |
| LDL cholesterol | −5.15 mg/dL | Moderate |
| HDL cholesterol | +2.76 mg/dL | Moderate |
| Systolic blood pressure | −5.34 mmHg | Low |
| Diastolic blood pressure | −6.12 mmHg | Very low |
| BMI | −0.57 kg/m² | Low |
| Waist circumference | −2.36 cm | Very low |
The strongest evidence was for triglyceride reduction (high certainty) and insulin resistance improvement (moderate certainty). Blood pressure effects, while numerically meaningful, had lower certainty — meaning the real-world effect could be smaller or larger than reported. Most studies lasted 12 weeks with dosages ranging from 600 mg to 4 grams daily.
For context, a triglyceride drop of nearly 30 mg/dL is clinically relevant. And an HOMA-IR reduction of 1.21 points can mean the difference between a lab result flagged as insulin resistant and one that falls within normal range. These are not trivial changes, though they need to be understood alongside the confidence levels — some of these findings need larger trials to confirm.
In postmenopausal women with metabolic syndrome, myo-inositol at just 2 grams per day improved glucose control, triglycerides, and HDL cholesterol, and 20 percent of participants no longer met the criteria for metabolic syndrome after treatment. That same review noted that MI appears to improve insulin resistance approximately twofold better than either pioglitazone or metformin — though this comparison should be interpreted cautiously, as it comes from indirect evidence rather than direct head-to-head trials across all populations.
The mechanism behind these broad metabolic effects ties back to inositol's role in insulin signaling. When insulin attaches to a cell receptor, inositol-derived phosphoglycans carry that signal forward in two ways: MI-derived messengers promote glucose transporter activation (GLUT4 translocation), while DCI-derived messengers activate glycogen synthase and pyruvate dehydrogenase. Both pathways reduce circulating glucose and insulin. Because elevated glucose actually competes with myo-inositol for cellular uptake and renal reabsorption, people with chronically high blood sugar may develop tissue-level inositol depletion — creating a cycle where insulin resistance begets further inositol deficiency, which worsens insulin resistance.
Dosage, Forms, and What Actually Matters on the Label
Not all inositol supplements are equivalent, and the differences are not just about quality — they are about fundamentally different compounds with different effects.
| Parameter | Myo-Inositol (MI) | D-Chiro-Inositol (DCI) |
|---|---|---|
| Primary action | Enhances FSH signaling, promotes aromatase, improves glucose uptake | Activates glycogen synthase, inhibits aromatase, reduces androgen-to-estrogen conversion |
| Ovarian effect | Supports egg maturation and follicle development | High doses impair oocyte quality and increase androgens |
| Typical PCOS dose | 2,000–4,000 mg/day | 50–600 mg/day (usually combined with MI) |
| Ideal ratio (combined) | 40:1 (MI:DCI) — matches physiological plasma ratio | |
| Psychiatric dose | 12,000–18,000 mg/day | Not studied for psychiatric use |
| Safety ceiling | Up to 18g/day for 3 months; 4g/day for 12 months | High doses (>1,200 mg/day) may worsen ovarian function |
The 40:1 ratio is not arbitrary. It reflects the natural concentration balance found in human blood plasma, and it is the only ratio that achieved full PCOS symptom recovery in preclinical models. Commercial supplements range from 0.4:1 to 104:1, with many popular products using ratios that have never been clinically validated. A product listing "inositol" without specifying whether it contains myo-inositol, D-chiro-inositol, or both — and in what ratio — is essentially asking you to guess.
Absorption is another underappreciated variable. Research shows that high doses of DCI (1 gram or more) competitively inhibit myo-inositol absorption in the gut through shared transporters (SMIT2). This means a supplement loaded with DCI could actually reduce your body's ability to absorb MI — the very compound most responsible for ovarian benefit. Co-administration with alpha-lactalbumin (a whey protein) has shown promise in improving inositol absorption, which may matter for the estimated 30 to 40 percent of PCOS patients who show "inositol resistance" — a partial or absent response to standard supplementation.

For hormonal balance purposes in PCOS, the most studied protocol is myo-inositol 2 grams twice daily (4 grams total), often combined with 200 to 400 micrograms of folic acid. Treatment periods in clinical trials range from 12 to 24 weeks, with some hormonal markers (especially SHBG) only improving after six months of consistent use. For anxiety and panic disorder, the doses tested are substantially higher — 12 to 18 grams daily — and these studies have not extended beyond a few months.
Myths vs Facts: Sorting Supplement Marketing from Science
| Myth | Fact |
|---|---|
| "Inositol is vitamin B8" | Inositol is not a true vitamin. Your body synthesizes it endogenously (~2g/day from the kidneys), and it is classified as a sugar alcohol, not an essential nutrient you must obtain from food. |
| "More DCI means better results for PCOS" | The opposite can be true. High DCI doses inhibit aromatase in the ovary, potentially increasing testosterone and worsening PCOS symptoms. Mouse and human studies confirm the 40:1 MI:DCI ratio works best. |
| "Inositol works as well as metformin with zero side effects" | Meta-analyses show non-inferiority to metformin for most PCOS outcomes. Side effects are far lower (7% vs 53%), but mild GI symptoms — diarrhea, nausea, gas — can still occur, particularly at higher doses. |
| "Inositol cures anxiety" | Small double-blind trials show significant panic attack reduction at 12-18g/day, but the overall meta-analytic evidence for anxiety and depression has not reached statistical significance. The data is promising for panic disorder specifically, not for generalized anxiety. |
| "Any inositol supplement will do" | Product ratios vary from 0.4:1 to 104:1 (MI:DCI). Many formulations have never been tested in clinical trials. The specific isomer, dose, and ratio all determine whether you get benefit, no effect, or potentially a negative outcome. |
Who Should (and Shouldn't) Consider Inositol
The strongest evidence supports inositol use for women with PCOS who have documented insulin resistance or who cannot tolerate metformin. In that population, the data — drawn from thousands of trial participants — consistently shows improvements in insulin sensitivity, menstrual regularity, androgen levels, and ovulation rates. If you are working with a provider to manage PCOS, inositol (specifically the 40:1 MI:DCI combination or MI alone at 4g/day) is worth discussing as either a standalone approach or an addition to existing treatment.
For women trying to conceive through IVF, myo-inositol supplementation at 4 grams daily has shown improved oocyte maturity (metaphase II rate) and fertilization rates in PCOS populations. A 2025 meta-analysis of 11 studies found a 1.55-fold higher rate of mature oocytes and 1.62-fold higher fertilization rate with MI supplementation. The effect was most pronounced in non-obese women with PCOS.
For panic disorder, the evidence is interesting but limited to small studies. If you are experiencing panic attacks and either prefer a non-pharmaceutical approach or want to augment existing treatment, the 12-18g/day dose range used in the clinical trials is the relevant one — and that is a substantially higher dose than what is in most off-the-shelf supplements. This should be discussed with a prescriber rather than self-managed.
Inositol is generally well tolerated and considered safe for use during pregnancy. Research on gestational diabetes prevention suggests 2 grams twice daily may reduce GDM incidence by 65 to 87 percent, though this application needs further confirmation in large-scale trials.
Who should proceed with caution: People on diabetes medications (inositol may enhance glucose-lowering effects), those taking lithium (inositol interacts with the lithium-inositol pathway), and anyone with bipolar disorder (mood stabilizers may specifically work by reducing inositol turnover). Always discuss supplementation with a healthcare provider before starting, particularly if you take prescription medications.
What inositol will not do: replace a comprehensive evidence-based treatment plan. It does not substitute for lifestyle modifications in PCOS, professional mental health treatment for severe anxiety disorders, or pharmaceutical intervention when those are medically indicated. The research positions it as a useful tool — sometimes a first-line option, sometimes an adjunct — but not a standalone solution for complex conditions.
Frequently Asked Questions
How long does it take for inositol to work for PCOS symptoms?
Insulin sensitivity markers (fasting insulin, HOMA-IR) can begin improving within 12 to 16 weeks. Menstrual cycle normalization often occurs within 35 days of starting supplementation. However, improvements in SHBG and longer-term hormonal markers typically require 24 weeks or more of consistent use. Ovulation restoration rates in studies ranged from 86 percent (with DCI at 1,200 mg/day) to 88 percent (with MI at 2g/day) over 3 to 6 months.
Is myo-inositol or D-chiro-inositol better for PCOS?
They serve different functions and are most effective together at a 40:1 ratio (MI to DCI). Myo-inositol supports ovarian function and FSH signaling, while D-chiro-inositol primarily addresses systemic insulin resistance. Taking DCI alone at high doses can actually worsen ovarian function by inhibiting aromatase. Most clinical guidelines recommend MI as the primary form, with small amounts of DCI in combination.
Can inositol replace anti-anxiety medication?
The evidence does not support using inositol as a direct replacement for prescribed anxiety medications. Small trials show meaningful panic attack reduction at 12-18 grams daily, but these doses are far above typical supplement amounts, the studies involved fewer than 25 participants each, and the meta-analytic evidence remains inconclusive. Discuss with your healthcare provider before making any changes to prescribed treatments.
What are the side effects of inositol?
At standard PCOS doses (2-4 grams daily), side effects are uncommon — occurring in roughly 7 percent of users in clinical trials. When they happen, they are typically mild gastrointestinal symptoms: nausea, diarrhea, gas, or abdominal discomfort. At the higher psychiatric doses (12-18 grams), mild GI effects become more common. Doses up to 18 grams for three months and 4 grams for 12 months have been documented as safe and well tolerated in published research.
Does inositol interact with metformin?
No dangerous interactions have been documented, and some researchers have investigated combining them. However, because both lower insulin and blood glucose through overlapping pathways, concurrent use should be monitored by a healthcare provider to avoid excessive glucose reduction. In clinical trials comparing them head-to-head, inositol showed similar effectiveness with fewer side effects, so the combination may not always be necessary.
Related Articles
- PCOS Natural Management — Diet, Supplements, and Lifestyle — A comprehensive overview of evidence-based approaches to managing polycystic ovary syndrome beyond medication.
- 7 Signs You May Have Anxiety (and What Your Body Is Really Telling You) — Understand the physical and emotional signals that point toward an anxiety disorder.
- Seed Cycling for Hormone Balance — Does It Work? — An honest look at the evidence behind this popular natural approach to hormonal regulation.
- How Cortisol Drives Weight Gain and What Actually Helps — The stress-hormone connection to metabolic dysfunction and strategies that address it.
- Ashwagandha Benefits, Dosage, and Side Effects — Another well-studied supplement for stress and hormonal support, with research to back it up.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











