
Nearly 1 Billion People Have Sleep Apnea — Most Don't Know It
Obstructive sleep apnea affects roughly one billion people worldwide, and an estimated 90% of them have never been diagnosed. Population studies show that at least 20.2% of men and 10.0% of women live with moderate-to-severe obstructive sleep apnea. An Icelandic population study published in the European Respiratory Journal found that roughly one in five middle-aged adults had moderate-to-severe OSA — yet the majority of them reported no symptoms and no daytime sleepiness.
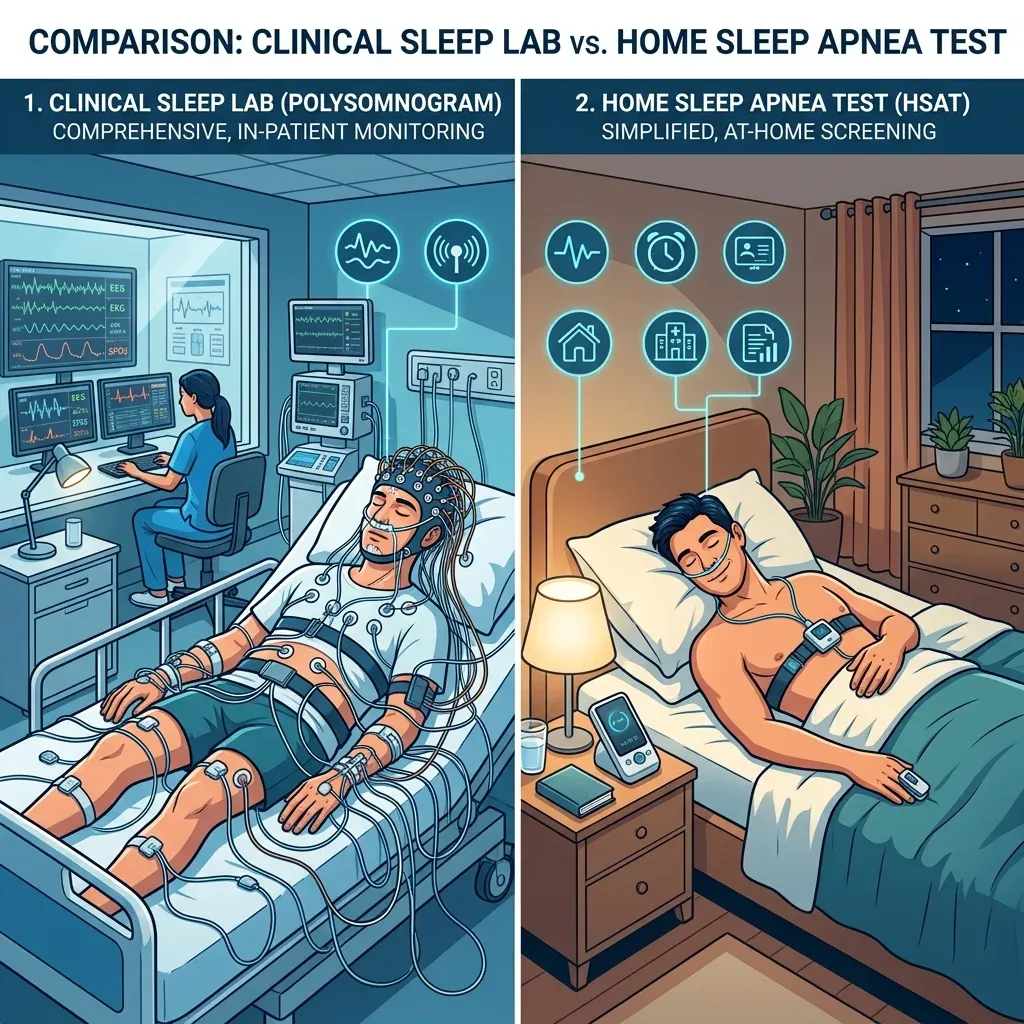
Part of the diagnosis bottleneck has been the test itself. For decades, confirming sleep apnea meant spending a night in a sleep lab, wired to equipment while a technician watched from the next room. That experience, combined with long wait lists and costs that can run into thousands of dollars, kept millions of people from ever getting tested.
Home sleep apnea tests opened a different path. These portable devices let you sleep in your own bed while sensors track your breathing overnight. They cost a fraction of a lab study, results come back within days, and for many patients they are clinically accurate enough to start treatment. But home tests have real limitations, and whether one makes sense for you depends on your symptoms, your medical history, and what your doctor thinks is happening while you sleep.
What a Home Sleep Test Actually Measures (and What It Misses)
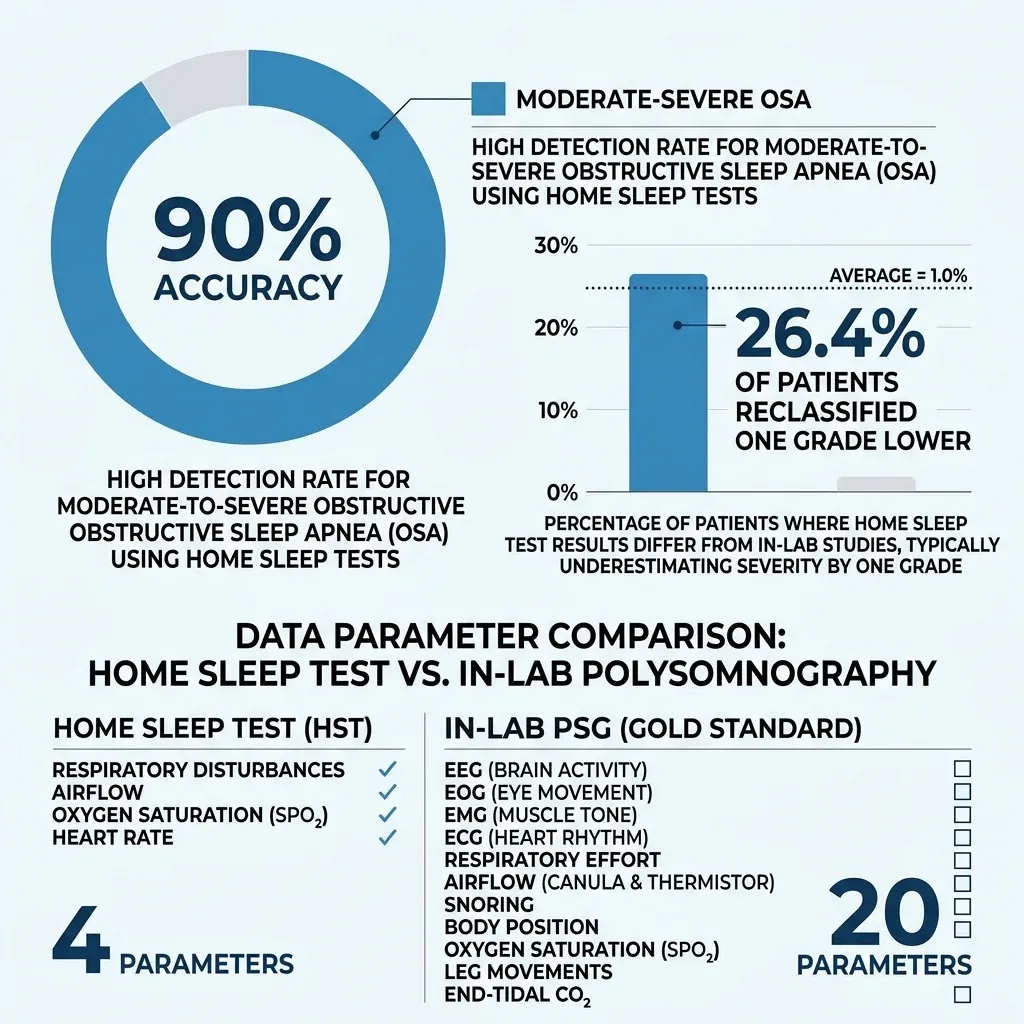
Think of a lab sleep study as a full-body surveillance system. A polysomnography setup tracks up to 20 different parameters: brain waves via electroencephalography, eye movements, chin and leg muscle activity, heart rhythm, airflow through your nose and mouth, chest and abdominal effort, blood oxygen, body position, and audio/video recording. It tells a sleep specialist not just whether you stopped breathing, but exactly when during which sleep stage, for how long, and what your brain and heart were doing when it happened.
A home sleep test, by comparison, is a targeted tool. Most devices classified as Type III under the AASM system measure four to six signals: airflow through a nasal cannula, respiratory effort via chest and abdominal belts, blood oxygen from a finger probe, and heart rate. Some newer models add body position sensors and microphones for snoring detection. What they almost universally lack is an electroencephalogram — the brain wave measurement that tells you whether someone is actually asleep or just lying in bed with their eyes closed.
That missing EEG creates a measurement problem. In a lab, the severity score called the apnea-hypopnea index (AHI) divides your total breathing events by your total sleep time. At home, without brain wave data, the device can only divide by total recording time — the entire period the device was running, including any time you spent awake, tossing, or reading your phone. The AASM calls this alternative metric the Respiratory Event Index (REI) rather than AHI, and it tends to produce a lower number for the same night of breathing disruptions.
AHI severity ranges: fewer than 5 events per hour is normal, 5 to 15 is mild, 15 to 30 is moderate, and 30 or above is severe. These cutoffs guide treatment decisions, so accuracy matters.
The practical implication: if you had 20 breathing events per hour of actual sleep but the device recorded an eight-hour window where you only slept six hours, your REI drops to 15 instead of 20. That could shift your classification from moderate to the boundary of mild — and mild OSA may be treated differently than moderate. Dr. Lawrence Epstein at Harvard Medical School describes home tests as "almost as accurate" as lab studies for people with moderate-to-severe sleep apnea and no other medical problems. For milder cases, that "almost" starts to matter more.
How Accurate Are Home Sleep Devices?
According to Mayo Clinic sleep experts Dr. Timothy Morgenthaler and Dr. Bhanu Prakash Kolla, home sleep tests accurately identify obstructive sleep apnea 90% of the time in people who show signs and symptoms of the condition. For the population these tests are designed for — adults with a high pre-test probability of moderate-to-severe OSA and no complicating medical conditions — that performance holds up well.
The problem shows up at the margins. A retrospective analysis by Bianchi and Goparaju examined 833 patients at a tertiary sleep center and found that when AHI was recalculated using total time in bed (simulating what a home test would report), 26.4% of patients with OSA were reclassified one severity grade lower. More than one in four patients looked less sick than they actually were. The same study found that among patients who appeared normal (AHI below 5), 66.4% actually had a respiratory disturbance index above 5 when respiratory effort-related arousals were counted — events that home tests cannot detect because they require EEG data.
Dr. Pahnwat Taweesedt at Stanford's Division of Sleep Medicine notes that newer devices using peripheral arterial tonometry (PAT) — a technology FDA-approved since 2001 that measures blood volume changes in your fingertip — show strong sensitivity for moderate-to-severe OSA but weaker sensitivity for mild cases. The technology is improving. The Onera Sleep Test System uses wireless patches that patients self-apply in under five minutes and shows high AHI correlation with lab studies. DormoVision X, which received FDA clearance in December 2024, can be configured for Type I, II, or III studies and supports multi-night assessment.
A Canadian systematic review (CADTH) looked at whether this scoring gap translates to worse patient outcomes. It does not appear to. The review found no significant differences in daytime sleepiness, hypertension, treatment adherence, or quality of life between patients diagnosed via home testing versus in-lab studies. The scores differ, but patients do about the same when matched to the right test.
One thing the AASM is firm about: diagnosis should never rely solely on automatically scored HSAT data. A board-certified sleep medicine physician must review the raw data. Auto-scoring algorithms can miss artifacts, misclassify events, and produce numbers that look definitive but carry hidden uncertainty.
Snoring, Fatigue, or Restless Legs: Which Symptoms Need the Lab?
The right test depends on what is keeping you up at night — or making you drag through the day.
Loud snoring with witnessed breathing pauses: This is the classic OSA presentation and the strongest candidate for home testing. If a bed partner reports snoring, gasping, or choking during sleep, and you have risk factors like excess weight or a large neck circumference, a home test can likely confirm or rule out moderate-to-severe obstructive sleep apnea.
Daytime fatigue and sleepiness: This is trickier. Excessive daytime sleepiness has a long list of possible causes. If your doctor suspects straightforward OSA based on your history and physical exam, a home test is reasonable. But fatigue can also signal narcolepsy, idiopathic hypersomnia, or periodic limb movement disorder — conditions that require an in-lab sleep study to diagnose because they depend on brain wave monitoring and leg movement sensors that home tests lack.
Insomnia: Chronic insomnia is actually a reason to avoid home testing. Severe insomnia can interfere with HSAT accuracy because if you barely sleep during the recording window, the device has too little data to produce a reliable score. People with significant insomnia who also need evaluation for sleep-disordered breathing should go straight to the lab, where a technician can observe the full picture and a sleep specialist can identify overlapping conditions.
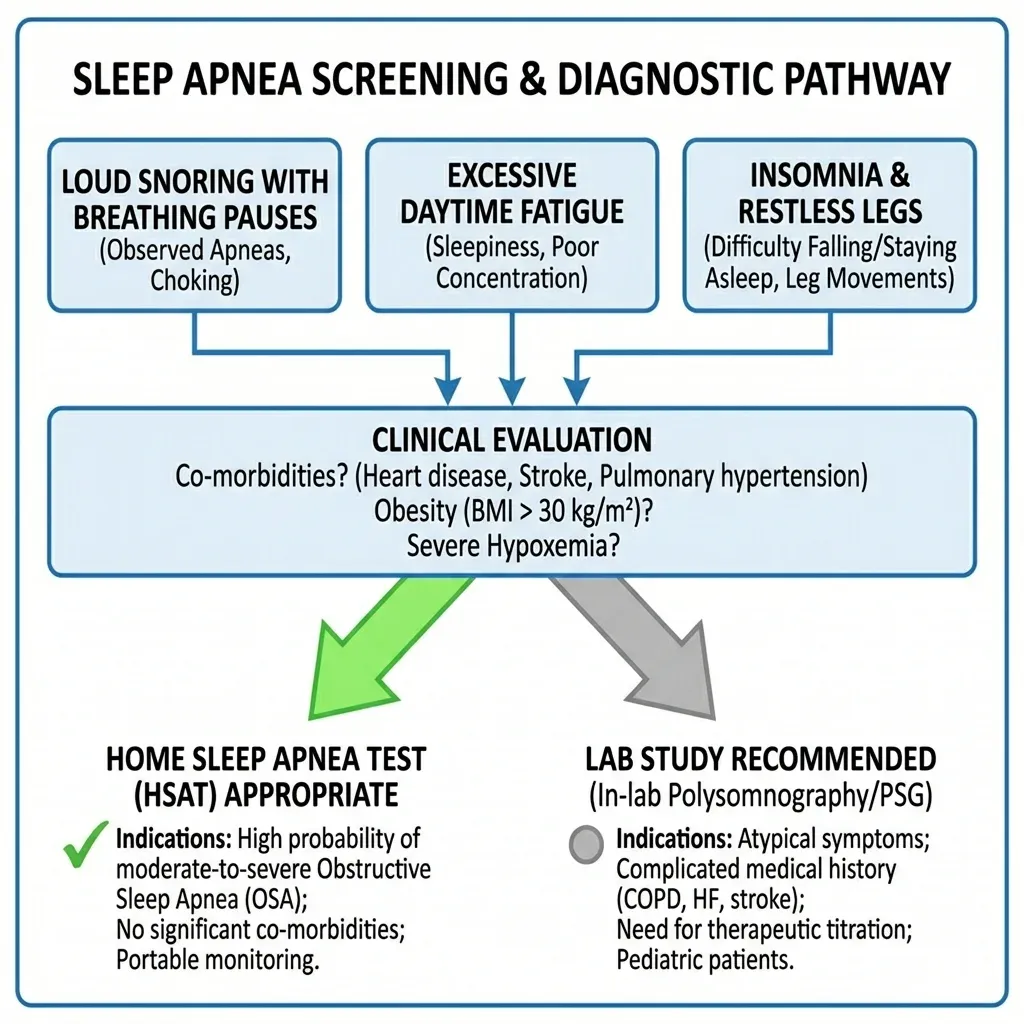
Restless legs or jerking during sleep: Periodic limb movements of sleep (PLMS) are a known blind spot for home sleep tests. Dr. Arveity Setty at Sanford Health notes that PLMS can cause insomnia or unrefreshing sleep and has been linked to cardiovascular complications — but home devices simply do not have the leg sensors to detect it. If you or your partner notice leg jerking or restlessness at night, an in-lab study is the appropriate test.
Sleepwalking, talking, or acting out dreams: Parasomnias like sleepwalking, night terrors, and REM sleep behavior disorder require the video monitoring, EEG, and EMG that only a full polysomnography provides. These conditions can be medically serious — REM behavior disorder, where people physically act out dreams, is linked to neurodegenerative diseases — and they cannot be evaluated with a breathing-focused home device.
| Symptom | Home Test | Lab Study | Why |
|---|---|---|---|
| Loud snoring + witnessed apneas | Yes | Backup if negative | Classic OSA pattern |
| Daytime sleepiness (OSA suspected) | Yes | If home test negative | May need further workup |
| Daytime sleepiness (cause unclear) | No | Yes | Narcolepsy, PLMD need EEG/EMG |
| Chronic insomnia | No | Yes | Low sleep time skews home results |
| Restless legs / leg jerking | No | Yes | Needs leg movement sensors |
| Sleepwalking / acting out dreams | No | Yes | Needs video, EEG, EMG |
Insurance Coverage: The Path from Home Test to CPAP
Cost is often what pushes patients toward home testing, and the difference is substantial. Home sleep tests typically range from $150 to $1,000, while in-lab polysomnography runs between $1,000 and $10,000, with the national average around $3,000. Johns Hopkins Medicine puts it more simply: a home test costs one-third to one-fifth of an in-lab study.
Medicare Part B covers all four types of sleep tests — Type I through Type IV — when you have clinical signs and symptoms of sleep apnea and a doctor orders the test. After meeting your Part B deductible, you pay 20% of the Medicare-approved amount. Type I studies (full lab polysomnography) are only covered when performed in a registered sleep lab facility.
Many private insurers have adopted a step-therapy approach. Insurance will often cover an in-lab sleep study only after a home test has been performed and is inconclusive, according to Mayo Clinic. This means the home test has become not just a convenience option but a required first step in many insurance pathways. If the home test clearly shows moderate-to-severe OSA, treatment can begin. If results are negative or borderline despite strong clinical suspicion, the insurer will then authorize a lab study.
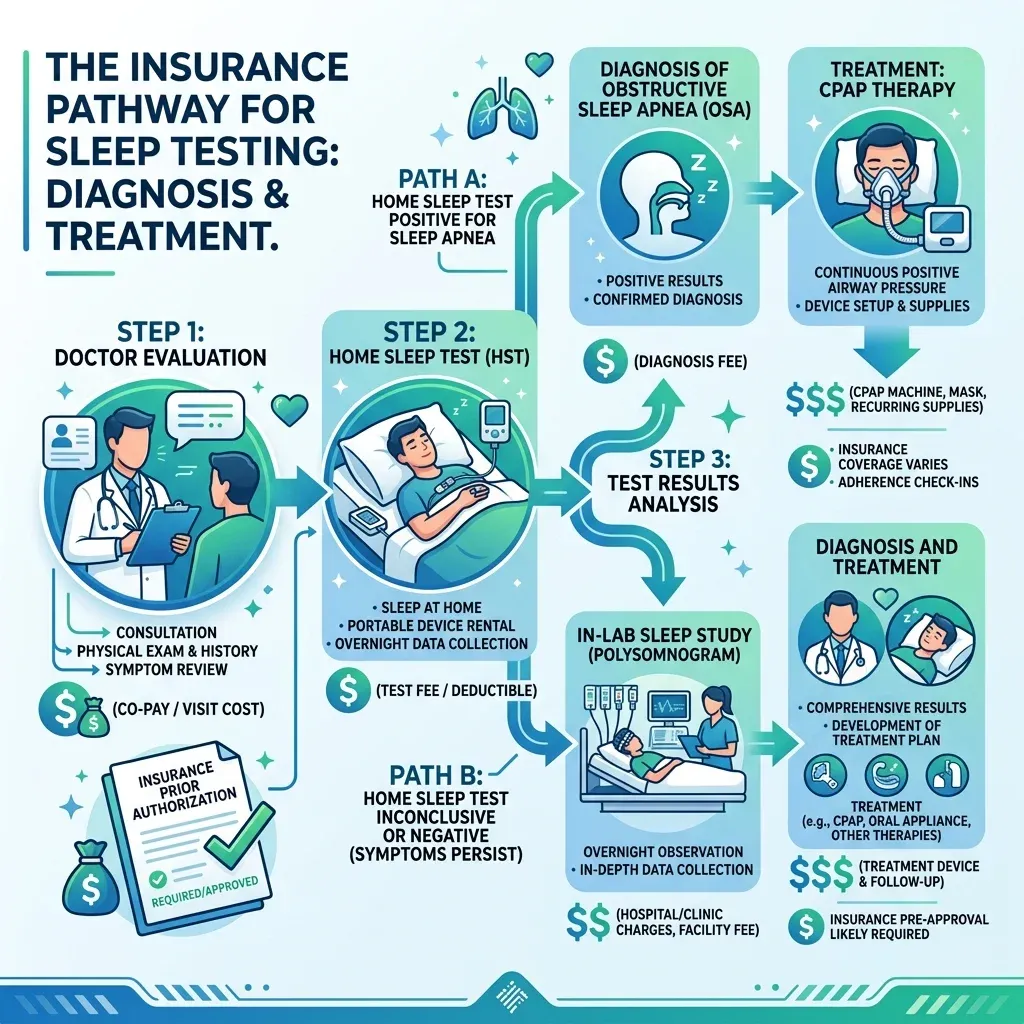
One wrinkle worth knowing about. For CPAP coverage specifically, Medicare and many private plans require documented evidence of sleep apnea meeting specific AHI or REI thresholds. If a home test underestimates your severity and your score falls just below the cutoff, you may face an additional lab study before your CPAP is covered. A split-night study — where the first half of the night diagnoses your apnea and the second half calibrates your CPAP pressure — can be more cost-effective than two separate lab visits.
When a Home Test Won't Cut It
The AASM draws specific boundaries around who should skip home testing. The 2017 clinical practice guideline, reinforced by the AASM's updated position statement, specifies that home testing is appropriate only for "uncomplicated adults presenting with signs and symptoms that indicate an increased risk of moderate to severe OSA."
In-lab polysomnography is recommended instead for patients with:
- Significant heart disease or heart failure — cardiac conditions can cause central sleep apnea patterns that home devices cannot distinguish from obstructive events
- Chronic lung disease (COPD, pulmonary fibrosis) — baseline oxygen levels may already be abnormal, and home test algorithms may misinterpret the data
- Neuromuscular disease — conditions like ALS or muscular dystrophy affect respiratory muscles in ways that require attended monitoring
- Chronic opioid use — opioids cause central apneas and irregular breathing patterns that home tests are not designed to detect
- History of stroke — stroke can produce complex breathing patterns during sleep
- Severe obesity (BMI above 40-50) — obesity hypoventilation syndrome overlaps with OSA but requires different monitoring and treatment
- Suspected non-respiratory sleep disorders — narcolepsy, parasomnias, or movement disorders need EEG and EMG data
The AASM also emphasizes that home testing should not be used for general screening of asymptomatic populations. Even though population studies show high OSA prevalence, the test is designed as a diagnostic tool for people who already have symptoms — not a fishing expedition for people who feel fine.
Children are another group where home testing has limited evidence. Dr. Taweesedt notes that while a few devices have pediatric FDA clearance (WatchPAT for ages 12+, SleepImage for ages 2+), a recent study found significant overestimation of AHI in obese adolescents. For children, in-lab polysomnography remains the standard.
Getting Reliable Results from Your At-Home Test
If you and your doctor decide a home test is the right move, the accuracy of your results depends partly on how well you manage the process. Unlike a lab study where a technician monitors everything, you are the technician at home.
Dr. Sapna Patil at Johns Hopkins recommends sleeping on both your back and your side during the test night. Sleep apnea is typically worse on your back, and having data from both positions gives your doctor a clearer picture of whether positional therapy might help.
The Sleep Foundation outlines a straightforward five-step process: get a prescription from your doctor, pick up or receive the device, take the test for one night following instructions carefully, return the equipment, and review results with your doctor. Along the way, avoid caffeine and alcohol on the test night (both alter breathing patterns), and ask your doctor whether to take any regular sleep medications.

Sensor displacement is the most common cause of unusable data. The nasal cannula can shift if you toss and turn, and the finger oximeter can slip off. Some patients tape the finger sensor in place as a precaution. If the device shows a recording failure in the morning, contact your provider — you may need to repeat the test rather than rely on a partial night of data.
If your home test comes back negative but you still feel terrible, do not treat that as a final answer. As AASM guidelines make clear, a negative or inconclusive HSAT in someone with high clinical suspicion should be followed by an in-lab polysomnogram. The home test can confirm apnea, but it cannot definitively rule it out.
Frequently Asked Questions
Can a home sleep test detect central sleep apnea?
Generally, no. Most home sleep tests are designed to detect obstructive sleep apnea, where the airway physically collapses. Central sleep apnea, where the brain fails to send proper breathing signals, requires the EEG and detailed respiratory monitoring available only in a lab setting. Some newer devices with effort belts may provide clues, but further validation is still needed before they can reliably diagnose central apnea at home.
How long does a home sleep test take?
The test itself is a single night. You wear the device while you sleep, and most people find it less disruptive than expected. Results are typically available within a few days to two weeks, depending on how quickly the data is uploaded and reviewed by a sleep medicine specialist.
What happens if my home test results are inconclusive?
Your doctor will likely recommend an in-lab polysomnography study. This is standard practice. Mayo Clinic sleep specialists note that inconclusive results in someone with strong clinical suspicion of OSA should always trigger a lab follow-up. Many insurance plans will cover the lab study after an inconclusive home test.
Do I need a prescription for a home sleep test?
Yes. A home sleep apnea test must be ordered by a medical provider based on your symptoms and medical history. The AASM position statement specifies that the appropriateness of an HSAT must be based on a face-to-face examination, either in person or via telemedicine. Over-the-counter consumer sleep trackers are not the same as medical-grade home sleep tests.
Will my insurance cover a home sleep test?
Most insurance plans, including Medicare Part B, cover home sleep tests when they are medically necessary and ordered by a doctor. You will typically pay a copay or coinsurance after meeting your deductible. Check with your insurer before the test to confirm coverage and whether the prescribing provider is in-network.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











