
What Happens When Estrogen Takes the Lead
Your body produces three types of estrogen, each with a different job. Estradiol (E2) is the most potent form, made primarily by the ovaries during reproductive years. Estrone (E1) takes over after menopause, produced mainly in fat tissue. Estriol (E3), the weakest of the three, rises during pregnancy. Under normal conditions, progesterone keeps these estrogens in check — the two hormones work like counterweights on a scale.
Estrogen dominance describes what happens when that scale tips. The VA Whole Health Library defines it as "increased estrogen levels relative to progesterone levels in the body." This means the problem is not always excess estrogen in absolute terms. A woman with normal estrogen levels but low progesterone can experience the same symptoms as someone with genuinely elevated estrogen. The ratio matters more than the raw numbers.
When estrogen goes unopposed, it drives cell growth in tissues that are estrogen-sensitive — the uterine lining, breast tissue, and even the thyroid. That persistent growth signal is what connects estrogen dominance to conditions like polycystic ovary syndrome (PCOS), endometriosis, uterine fibroids, and fibrocystic breast changes. According to Cleveland Clinic, this unopposed condition allows estrogen to work excessively, potentially causing cell overgrowths like uterine tumors.
Key point: Estrogen dominance is about the ratio of estrogen to progesterone, not just high estrogen alone. You can have normal estrogen levels and still be estrogen-dominant if your progesterone is too low.
The Warning Signs Your Body Sends
The symptoms of estrogen dominance overlap with many other conditions, which is part of why it often goes unrecognized. They tend to creep in gradually rather than appearing all at once.
In women, the most common signals involve the menstrual cycle. Heavy periods, cycles that arrive unpredictably, and worsening PMS symptoms all point toward an estrogen-progesterone imbalance. Cleveland Clinic notes that when progesterone drops, the resulting hormonal shift triggers weight gain, depression, heavy bleeding, reduced libido, and gallbladder complications.
Beyond the reproductive system, estrogen dominance affects sleep, mood, and body composition. Many women report difficulty falling asleep, increased anxiety, persistent bloating, and stubborn weight gain around the hips and thighs — areas where estrogen preferentially directs fat storage. Research published in Endocrine Reviews confirms that estrogen controls where the body deposits fat, and disruptions in estrogen receptor signaling cause visceral fat accumulation and features of metabolic syndrome.
| System | Common Symptoms |
|---|---|
| Menstrual | Heavy or irregular periods, worsening PMS, spotting between periods |
| Reproductive | Breast tenderness, fibrocystic breasts, difficulty conceiving |
| Neurological | Headaches/migraines, mood swings, anxiety, brain fog |
| Metabolic | Weight gain (hips/thighs), bloating, water retention, fatigue |
| Sleep | Insomnia, difficulty staying asleep, night sweats |
| Other | Hair thinning, low libido, thyroid disruption |
Men are not immune. Excess estrogen in men — whether from increased aromatase activity in fat tissue or environmental exposures — can manifest as gynecomastia (breast tissue growth), reduced sex drive, and erectile dysfunction. A review in Physiological Reviews found that men with aromatase overexpression develop gynecomastia and testicular changes, confirming that estrogen excess is not exclusively a female concern.
Root Causes Behind the Imbalance
Estrogen dominance rarely has a single cause. It usually results from several converging factors — biological, environmental, and behavioral.
Excess Body Fat
Fat tissue actively produces estrogen through an enzyme called aromatase, which converts androgens into estrogens. The more fat you carry, the more estrogen your body manufactures outside the ovaries. After menopause, adipose tissue becomes the primary estrogen source. This creates a feedback loop: excess estrogen promotes fat storage, and more fat produces more estrogen.
Chronic Stress and Cortisol
When stress is constant, your adrenal glands prioritize cortisol production. Both cortisol and progesterone are built from the same precursor molecule (pregnenolone), and under chronic stress, more pregnenolone gets funneled toward cortisol at progesterone's expense. The result is a cortisol-driven drop in progesterone that leaves estrogen relatively unopposed — even if estrogen levels themselves have not changed.
Xenoestrogens: The Environmental Factor
Synthetic chemicals found in plastics (BPA, phthalates), pesticides, and personal care products can bind to estrogen receptors and mimic estrogen's effects. These xenoestrogens add to your total estrogenic load without showing up on a standard hormone test. Cleveland Clinic identifies them as a significant contributing factor, recommending organic foods and glass or steel containers as basic precautions.
Alcohol Consumption
A narrative review of 43 studies found that alcohol consumption exceeding 25 grams daily (roughly two standard drinks) increased estrone and estradiol levels by 10 to 20 percent. Alcohol impairs the liver's ability to break down and clear estrogen, and even moderate intake has measurable hormonal effects.
Sedentary Lifestyle
The same review linked sedentary behavior exceeding 10 hours daily to elevated unconjugated estrogens. Physical inactivity reduces the body's ability to metabolize estrogen efficiently and contributes to the excess body fat that further drives estrogen production.
Gut Dysbiosis
Your gut bacteria play a direct role in estrogen regulation through a mechanism called the estrobolome — a specific set of bacterial genes that can reactivate estrogen the liver already deactivated. When gut bacteria are out of balance, more estrogen gets pushed back into circulation. (More on this in the next section.)
How Your Liver and Gut Process Estrogen
Estrogen clearance runs through two organs most people do not associate with hormones: the liver and the gut. When either falters, estrogen accumulates.
Liver Phase I: Breaking Estrogen Down
The liver metabolizes estrogen through three distinct pathways, each producing metabolites with very different biological effects. A review published in Cancer Letters mapped these pathways in detail:
| Pathway | Metabolite Produced | Effect on the Body |
|---|---|---|
| 2-hydroxylation | 2-hydroxyestrone (2-OHE) | Protective — weak estrogen activity, may block stronger estrogens |
| 4-hydroxylation | 4-hydroxyestrone (4-OHE) | Potentially harmful — can form DNA-damaging adducts |
| 16-hydroxylation | 16α-hydroxyestrone (16-OHE1) | Proliferative — promotes cell growth, linked to inflammation |
The ratio between these metabolites matters clinically. According to a pilot study in the journal Thyroid, a 2-OHE to 16-OHE1 ratio below 2.0 correlates with increased cancer risk, while ratios above 2.0 indicate more protective estrogen metabolism. The goal of many natural interventions is to push more estrogen through the 2-hydroxylation (protective) pathway.
Liver Phase II: Packaging for Removal
After Phase I breaks estrogen into metabolites, Phase II enzymes attach molecules like glucuronic acid or sulfate to these metabolites — a process called conjugation. This makes the metabolites water-soluble so the body can excrete them through bile (into the intestines) and urine. The COMT enzyme also methylates catechol estrogens into methoxyestrogens, which actively suppress tumor cell proliferation.
Anything that compromises liver function — excessive alcohol, a diet low in the B vitamins and magnesium that fuel these enzymes, or high toxic burden — slows this clearance process and allows estrogen to recirculate.
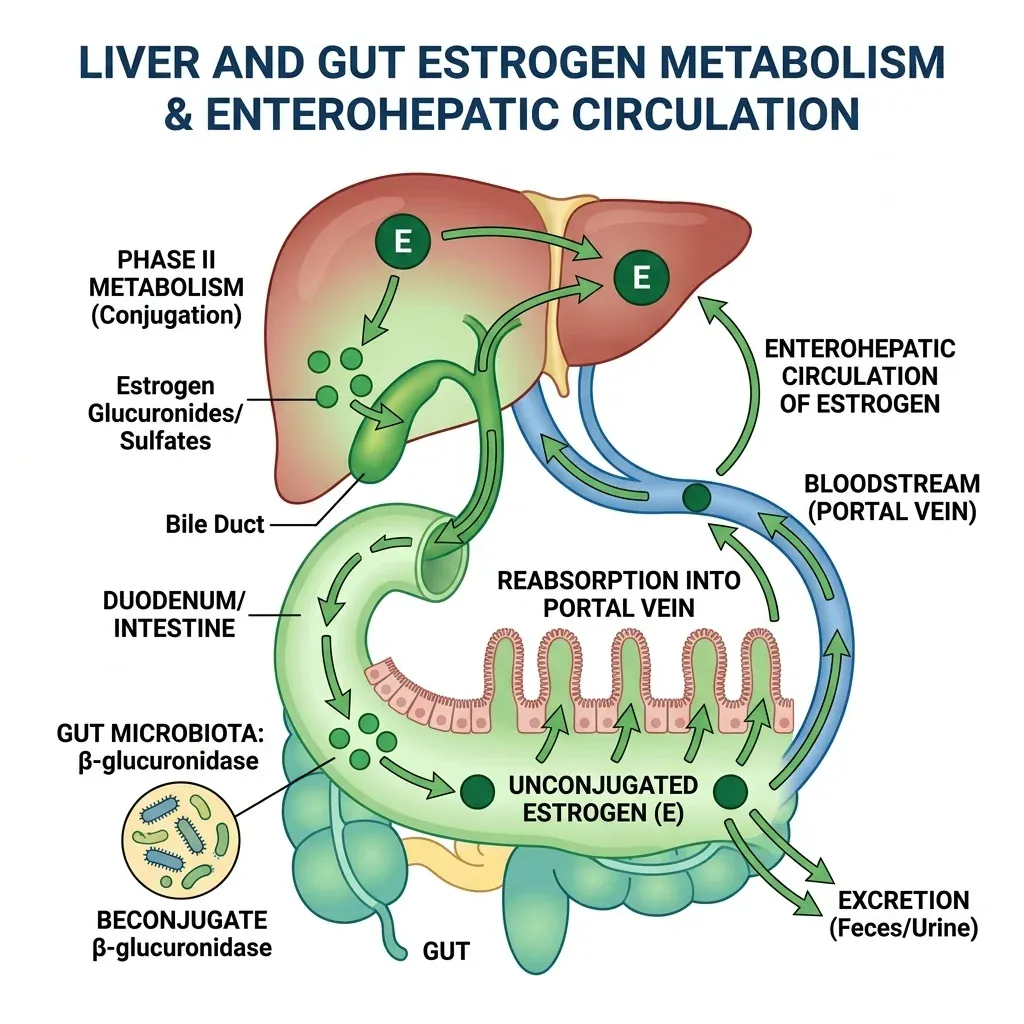
The Gut Connection: Your Estrobolome
Here is where the story takes an unexpected turn. After the liver packages estrogen for excretion and sends it into the intestines via bile, gut bacteria get a vote on whether that estrogen actually leaves the body. A specific collection of gut bacterial genes — called the estrobolome — produces the enzyme beta-glucuronidase (gmGUS). This enzyme strips the glucuronic acid tag the liver attached, reactivating the estrogen and allowing it to be reabsorbed into the bloodstream through enterohepatic circulation.
In a balanced gut, this recycling system works as designed, maintaining healthy estrogen levels. But when dysbiosis occurs — from antibiotics, poor diet, or chronic stress — beta-glucuronidase activity can spike. A 2017 review in Maturitas confirmed that this mechanism links gut dysbiosis to conditions including obesity, endometriosis, PCOS, and estrogen-sensitive cancers. The same disruption works in reverse: when gut diversity plummets (as it often does after menopause), reduced beta-glucuronidase activity leads to lower circulating estrogen and worsening menopausal symptoms.
The takeaway: Your liver deactivates estrogen, but your gut decides how much of it actually gets eliminated. A healthy microbiome is essential for proper estrogen clearance.
Testing and Assessment: Know Your Numbers
If your symptoms point toward estrogen dominance, testing can confirm it — but timing, methodology, and which markers you measure all matter.
Blood Tests
A standard hormone panel measures estradiol (E2), estrone (E1), and progesterone via a simple blood draw. For premenopausal women, timing is critical — progesterone peaks in the luteal phase (about a week after ovulation), so testing in the follicular phase gives misleadingly low readings.
| Marker | What It Tells You | Optimal Timing |
|---|---|---|
| Estradiol (E2) | Primary active estrogen level | Day 3 of cycle (follicular) or day 21 (luteal) |
| Progesterone | Whether ovulation occurred; estrogen counterbalance | Day 19-22 (luteal phase peak) |
| SHBG | How much estrogen is free vs. bound | Any time (relatively stable) |
| Estrone (E1) | Fat-derived estrogen (relevant post-menopause) | Any time |
Sex hormone-binding globulin (SHBG) deserves particular attention. A pooled analysis of nine prospective studies found that higher SHBG levels were inversely associated with breast cancer risk, suggesting that the bioavailable (unbound) estrogen fraction drives the effects you feel. Low SHBG effectively amplifies estrogen's impact even when total levels appear normal.
Urinary Estrogen Metabolite Testing
Urinary testing goes deeper by measuring how your body is processing estrogen — specifically the ratio of protective 2-hydroxyestrone to proliferative 16α-hydroxyestrone. In the DIM pilot study discussed earlier, a 2-OHE:16-OHE1 ratio below 2.0 was associated with increased cancer risk. This type of test can reveal whether your liver is favoring protective or problematic metabolic pathways.
When to Test
Testing makes sense with persistent matching symptoms — irregular cycles, unexplained midsection weight gain, or a family history of estrogen-sensitive cancers. Perimenopause is another common window, as progesterone drops faster than estrogen during this transition, creating relative estrogen dominance even as overall hormone levels decline.
Myths vs. Facts About Estrogen Dominance
| Myth | Fact |
|---|---|
| Estrogen dominance means your estrogen is too high | It refers to the ratio of estrogen to progesterone. You can have normal estrogen with low progesterone and still be estrogen-dominant. |
| Only women are affected | Men produce estrogen via aromatase in fat, brain, skin, and bone tissue. Excess estrogen in men causes gynecomastia and metabolic changes (Physiological Reviews). |
| Estrogen dominance is an established medical diagnosis | It is a clinical concept used in integrative and functional medicine, not a formal diagnosis in conventional endocrinology. The underlying hormonal imbalances are real and measurable. |
| You need to eliminate all estrogen | Estrogen is essential for bone density, cardiovascular health, brain function, and metabolism. The goal is balance, not elimination. |
| Soy foods worsen estrogen dominance | Whole soy foods contain phytoestrogens that are much weaker than human estrogen (100-1000x weaker binding affinity). The VA Whole Health Library actually recommends whole soy foods as part of an estrogen-balancing diet. |
| Supplements alone can fix it | Supplements can support estrogen metabolism, but without addressing root causes (diet, stress, body composition, gut health), results will be limited. |

Natural Strategies to Restore Hormonal Balance
No single intervention corrects estrogen dominance alone. The combination of dietary changes, targeted movement, stress management, and gut support creates conditions that allow your body to rebalance.
Eat More Cruciferous Vegetables
Broccoli, cauliflower, Brussels sprouts, kale, and cabbage contain compounds called glucosinolates that break down into indole-3-carbinol (I3C) and its metabolite 3,3'-diindolylmethane (DIM). These compounds shift estrogen metabolism toward the protective 2-hydroxylation pathway. In a case-control study at Roswell Park Cancer Institute involving nearly 3,000 participants, the highest cruciferous vegetable intake was associated with a 32% reduction in breast cancer odds (OR: 0.68; 95% CI: 0.55-0.86), with broccoli and cauliflower showing the strongest protective effects.
How you prepare them matters. Raw or lightly steamed cruciferous vegetables retain more of their active compounds than heavily cooked versions. The same study found that raw consumption showed stronger protective associations than cooked preparations.
Consider I3C or DIM Supplementation
For concentrated support, the VA recommends indole-3-carbinol at 300 mg daily. A pilot study published in Thyroid tested DIM at 300 mg daily in women with thyroid proliferative disease and found that it shifted the protective 2-OHE to 16-OHE1 ratio above 2.0 in all seven patients — five of whom started below the risk threshold. An earlier dose-response study showed that 150 mg of DIM increased the protective ratio by 76%, while 300 mg increased it by 170%.
I3C has more clinical trial data than DIM, though both target the same metabolic pathways. A review in Nutrition Reviews concluded that I3C produces "beneficial shifts in hormone markers" with a stronger evidence base. Talk to your healthcare provider before starting either, particularly if you take thyroid medication or hormonal therapies.
Combine Diet and Exercise
The combination outperforms either strategy alone. A narrative review of 43 studies (28 randomized controlled trials) found that combined diet and exercise interventions produced a 20.3% decrease in estradiol, an 11.1% decrease in estrone, and a 25.8% increase in sex hormone-binding globulin. By comparison, exercise alone reduced estrone by only 5.5%, and diet alone reduced estradiol by 16.2%. Structured exercise at 60 to 80 percent of maximum heart rate produced measurable estrogen reductions, though outcomes were partially mediated through weight loss.
Body fat reduction is particularly effective because it removes the tissue that produces estrogen outside the ovaries — especially relevant after menopause when adipose tissue becomes the primary estrogen source.
Support Your Liver
The liver needs specific nutrients to run its estrogen-clearing Phase I and Phase II pathways efficiently. B vitamins (especially B6, B12, and folate) fuel the COMT enzyme that methylates catechol estrogens into protective methoxyestrogens. Magnesium supports multiple detoxification enzymes. A high-quality diet rich in anti-inflammatory compounds — while limiting alcohol — gives the liver the raw materials it needs to process estrogen properly.
Fiber is the other critical piece. It binds to estrogen in the intestines and escorts it out through stool, reducing the amount available for reabsorption via the enterohepatic cycle. Aim for 25 to 35 grams daily from vegetables, legumes, flaxseed, and whole grains.
Restore Gut Health
Because your estrobolome controls how much deactivated estrogen gets recycled back into circulation, gut health directly affects estrogen levels. Probiotics, prebiotic fibers (from garlic, onions, asparagus, and bananas), and fermented foods support microbial diversity. Reducing unnecessary antibiotic use also protects the estrobolome. The VA's Whole Health Library recommends probiotics specifically as part of an estrogen-dominance management plan.
Manage Stress
Chronic stress drains progesterone by diverting its precursor (pregnenolone) toward cortisol production. Meditation, deep breathing, regular sleep schedules, and appropriate exercise help preserve progesterone and maintain the estrogen-to-progesterone ratio.
Reduce Xenoestrogen Exposure
Practical steps include switching to glass or stainless steel containers, choosing personal care products without parabens and phthalates, filtering drinking water, and prioritizing organic produce for items most heavily treated with estrogenic pesticides.
Nutrients That Support Progesterone
Cleveland Clinic highlights that vitamin C, zinc, magnesium, and B vitamins support healthy progesterone production. Seed cycling — rotating flaxseed and pumpkin seeds in the first half of the menstrual cycle with sunflower and sesame seeds in the second — is a popular dietary approach to support hormone balance, though clinical evidence remains limited.
Frequently Asked Questions
Can estrogen dominance cause weight gain even with a healthy diet?
Yes. When the estrogen-to-progesterone ratio is skewed, the body holds onto fat — particularly around the hips, thighs, and lower abdomen — regardless of caloric intake. Research in Endocrine Reviews confirms that disruptions in estrogen receptor signaling cause visceral fat accumulation that resists standard dietary approaches. Addressing the hormonal imbalance alongside diet is usually necessary.
How long does it take to rebalance estrogen levels naturally?
Most women notice symptom improvements within 2 to 3 menstrual cycles when consistently applying dietary and lifestyle changes. Measurable shifts in estrogen metabolite ratios have been documented within 14 days of DIM supplementation, though sustained improvement requires ongoing lifestyle modification.
Is estrogen dominance the same as having high estrogen?
No. Estrogen dominance refers to the ratio of estrogen to progesterone, not the absolute level of estrogen. You can have estrogen within the normal range and still experience estrogen dominance if your progesterone is too low — a common occurrence during perimenopause, periods of high stress, or with anovulatory cycles.
Should I avoid all soy if I have estrogen dominance?
Whole soy foods (edamame, tofu, tempeh, miso) contain phytoestrogens that bind to estrogen receptors with 100 to 1,000 times weaker affinity than human estrogen. In moderate amounts, they may offer a protective effect by occupying receptors without producing strong estrogenic activity. The VA Whole Health Library includes whole soy in its recommended dietary approach for estrogen dominance.
Can men have estrogen dominance?
Yes. Men produce estrogen through aromatase activity in fat, brain, skin, and bone. When aromatase activity increases — driven by excess body fat, alcohol, or xenoestrogens — men develop gynecomastia, reduced libido, and metabolic changes. A review in Physiological Reviews documented that men with aromatase overexpression develop breast tissue growth and testicular changes.
Related Articles
- Hormone Replacement Therapy (HRT) — Benefits, Risks, and Modern Evidence — A comprehensive look at when HRT makes sense and what current research says about safety.
- Perimenopause Symptoms and Natural Management Strategies — How to navigate the hormonal shifts that begin years before menopause.
- Seed Cycling for Hormone Balance — Does It Work? — The evidence behind this popular dietary approach to supporting estrogen and progesterone balance.
- Thyroid Health and Hashimoto's: Symptoms, Diet, and Natural Support — Thyroid and estrogen are deeply interconnected — this guide covers the thyroid side.
- How Cortisol Drives Weight Gain and What Actually Helps — Understanding the stress-cortisol-progesterone connection that contributes to estrogen dominance.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











