Your Adrenal Glands Run a 24-Hour Cortisol Shift — Here's What That Looks Like
Sitting on top of each kidney, your two adrenal glands weigh about as much as a grape. For organs that small, they carry an outsized workload. They produce cortisol, adrenaline, aldosterone, DHEA, and small amounts of sex hormones — each doing something distinct to keep your body functioning under both ordinary and extreme conditions.
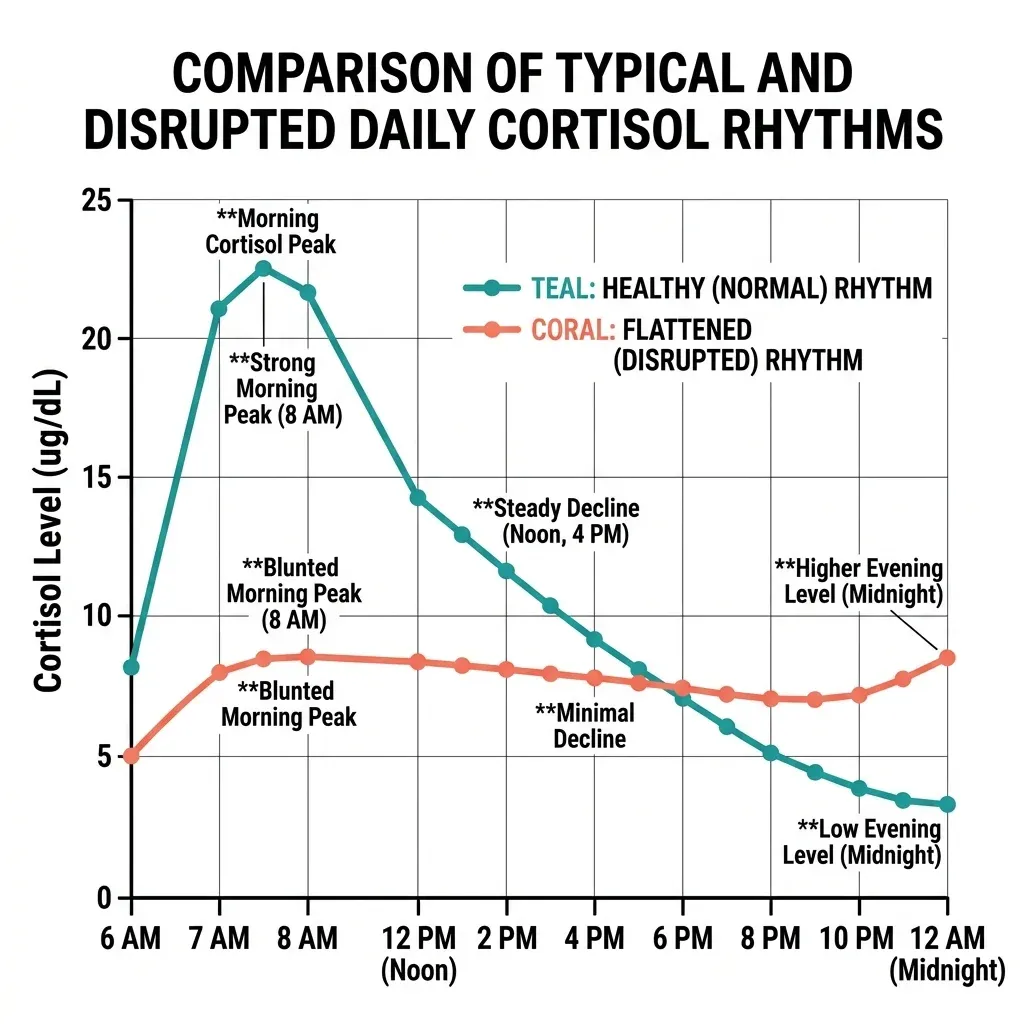
Cortisol gets the most attention in the "adrenal fatigue" conversation, so it's worth understanding how it actually behaves. Your adrenal glands don't release cortisol at a steady drip. Instead, cortisol follows a circadian rhythm that peaks within 30 to 45 minutes after waking, then gradually declines throughout the day and hits its lowest point around midnight. On top of that daily cycle, cortisol pulses roughly every hour in what researchers call an ultradian rhythm — brief surges and dips that your tissues actually rely on to stay responsive.
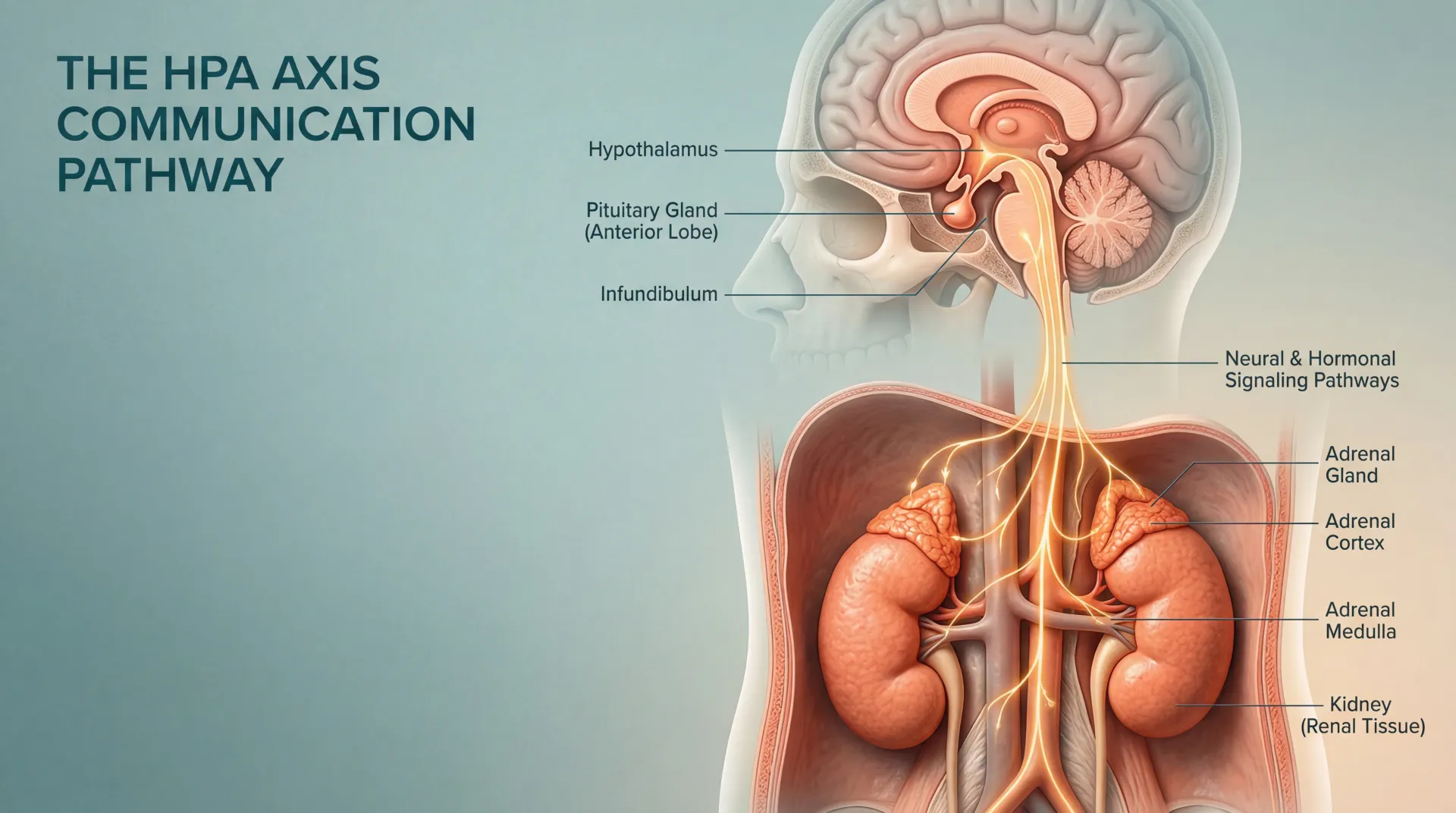
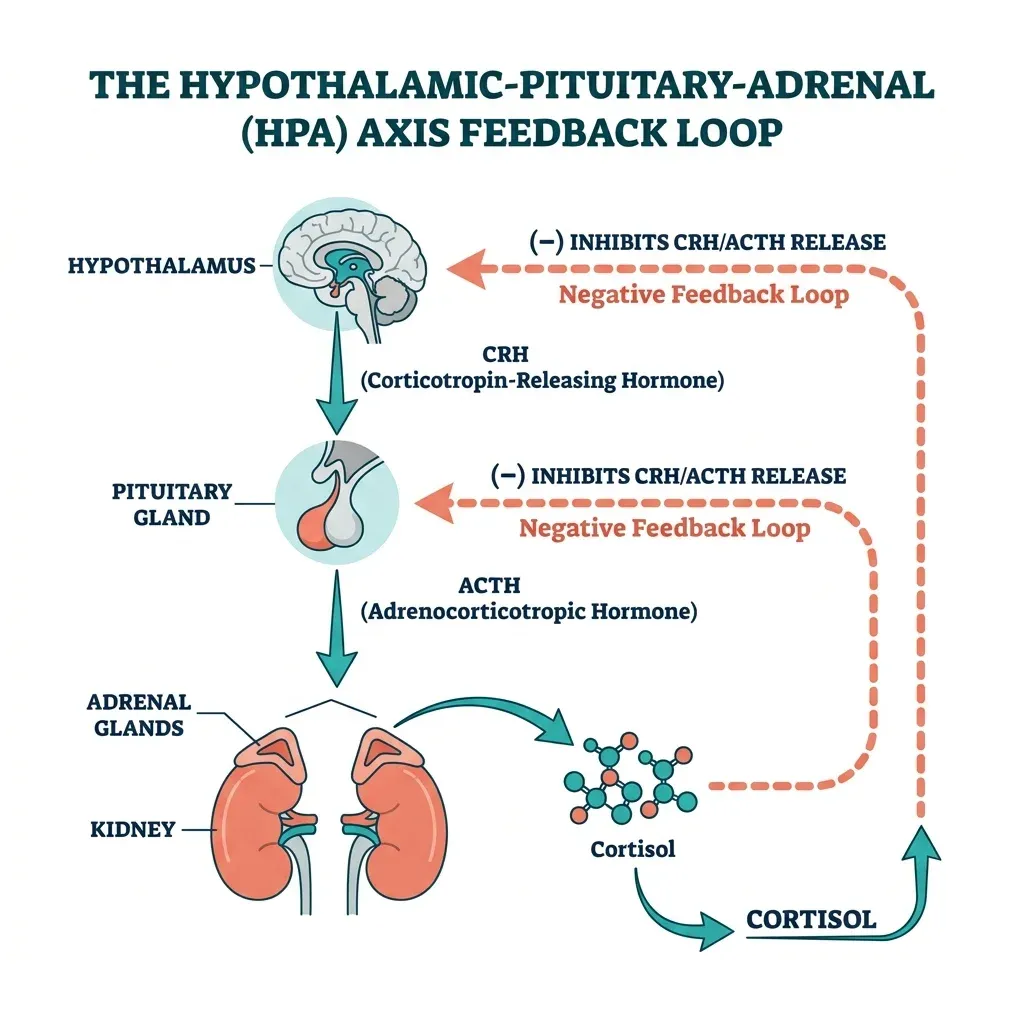
This system doesn't operate in isolation. It's part of a three-organ communication chain called the hypothalamic-pituitary-adrenal (HPA) axis. The hypothalamus releases corticotropin-releasing hormone (CRH), which tells the pituitary gland to secrete adrenocorticotropic hormone (ACTH), which signals the adrenal glands to produce cortisol. Once cortisol rises high enough, it feeds back to the hypothalamus and pituitary to slow the whole cascade down. This negative feedback loop is what keeps cortisol from climbing indefinitely — and it operates with a precision that chronic stress can gradually erode.
The system also has a self-correcting physical component that only became clear in recent research. A study published in Molecular Systems Biology demonstrated that the functional mass of hormone-secreting glands adjusts over weeks through a process the researchers call dynamical compensation. Under sustained stress, the adrenal cortex physically enlarges. When stress subsides, it gradually shrinks back. This isn't organ damage — it's deliberate physiological adaptation, and understanding it changes how we interpret what's happening in people who feel persistently fatigued.
A Chiropractor Named It in 1998 — and the Idea Stuck
The term "adrenal fatigue" was coined in 1998 by James Wilson, a chiropractor and naturopath, in his book Adrenal Fatigue: The 21st Century Stress Syndrome. The premise was straightforward: prolonged stress depletes the adrenal glands' ability to produce enough cortisol, leaving people in a state of persistent low-grade hormonal deficiency. Fatigue, brain fog, sleep problems, cravings for salt and sugar, difficulty recovering from illness — all supposedly traceable back to "tired" adrenals.
The concept resonated immediately with people who felt unwell but couldn't get a satisfying medical explanation. Standard blood work came back normal. Doctors found nothing diagnosable. But they still felt terrible. "Adrenal fatigue" offered a narrative that matched their experience: your body is exhausted because your stress hormones are depleted.
What gave the idea traction was that it sat in a plausible-sounding space between two real conditions. Addison's disease (primary adrenal insufficiency) occurs when the adrenal glands are damaged and genuinely cannot produce enough cortisol — it's rare, clinically distinct, and can be life-threatening without treatment. Cushing's syndrome represents the opposite extreme, with dangerously elevated cortisol from tumors or prolonged steroid use. "Adrenal fatigue" positioned itself as a milder version of Addison's — not quite organ failure, but enough depletion to cause problems.
The distinction matters because actual adrenal insufficiency looks nothing like what gets labeled "adrenal fatigue." Cleveland Clinic endocrinologist Pratibha Rao puts it directly: adrenal glands "don't simply tire out." True adrenal insufficiency involves extreme fatigue, unintentional weight loss, dangerously low blood pressure, low blood sugar, and can progress to adrenal crisis — a medical emergency. These patients need hormone replacement to survive.
58 Studies, One Answer: "No Substantiation"
In 2016, endocrinologists Flavio Cadegiani and Claudio Kater did something nobody had done before: they systematically reviewed every available study that could test whether adrenal fatigue was real. Their systematic review in BMC Endocrine Disorders started with 3,470 articles and narrowed them to 58 that met inclusion criteria for actually measuring adrenal function in fatigued people.
The findings were unambiguous. Across all study types — whether measuring morning cortisol, cortisol awakening response, or full daily salivary cortisol curves — the researchers found "an almost systematic finding of conflicting results." Some studies showed lower cortisol in fatigued groups. Others showed higher cortisol. Most showed no meaningful difference at all. Their conclusion: there is "no substantiation that 'adrenal fatigue' is an actual medical condition."
They also flagged a critical methodological problem: the most rigorous tools for assessing HPA axis function — like the insulin tolerance test and CRH stimulation test — were almost never used in fatigue research. The studies relied heavily on salivary cortisol samples, which are prone to collection errors, timing inconsistencies, and confounding from sleep patterns, medications, and even what people ate that morning.
The Endocrine Society, which represents over 18,000 endocrinologists worldwide, states plainly: "No scientific proof exists to support adrenal fatigue as a true medical condition." The symptoms attributed to it are "common and non-specific, meaning they can be found in many diseases."
This doesn't mean the people reporting these symptoms are making them up. It means the explanation — that their adrenal glands are depleted — doesn't match what researchers actually find when they measure adrenal function. The symptoms are real. The proposed mechanism isn't.
| Claim | What the Evidence Shows |
|---|---|
| Stress depletes adrenal glands | Adrenal glands physically enlarge under sustained stress, increasing cortisol output |
| Fatigued people have low cortisol | Systematic review of 58 studies found conflicting results — no consistent pattern |
| Saliva tests can diagnose it | No validated diagnostic test exists; salivary cortisol is highly variable |
| Adrenal supplements restore function | Unnecessary hormone supplementation can suppress natural production for months |
| It's a milder form of Addison's | Adrenal insufficiency is a clinically distinct condition requiring medical diagnosis |
HPA Axis Dysregulation: What Chronic Stress Actually Does to Your Hormones
If "adrenal fatigue" isn't supported by evidence, what is happening to people who feel terrible after prolonged stress? Something more nuanced than simple gland depletion.
The HPA axis is a feedback system, and feedback systems don't just "run out" — they can become dysregulated in multiple directions. Research from the University of Cincinnati's Department of Psychiatry shows that chronic stress can produce at least three distinct hormonal patterns: baseline cortisol hypersecretion, sensitized responses to new stressors, or what they term "adrenal exhaustion" — and which pattern emerges depends on the severity, duration, and type of stress combined with individual factors like genetics, sex, age, and developmental history.
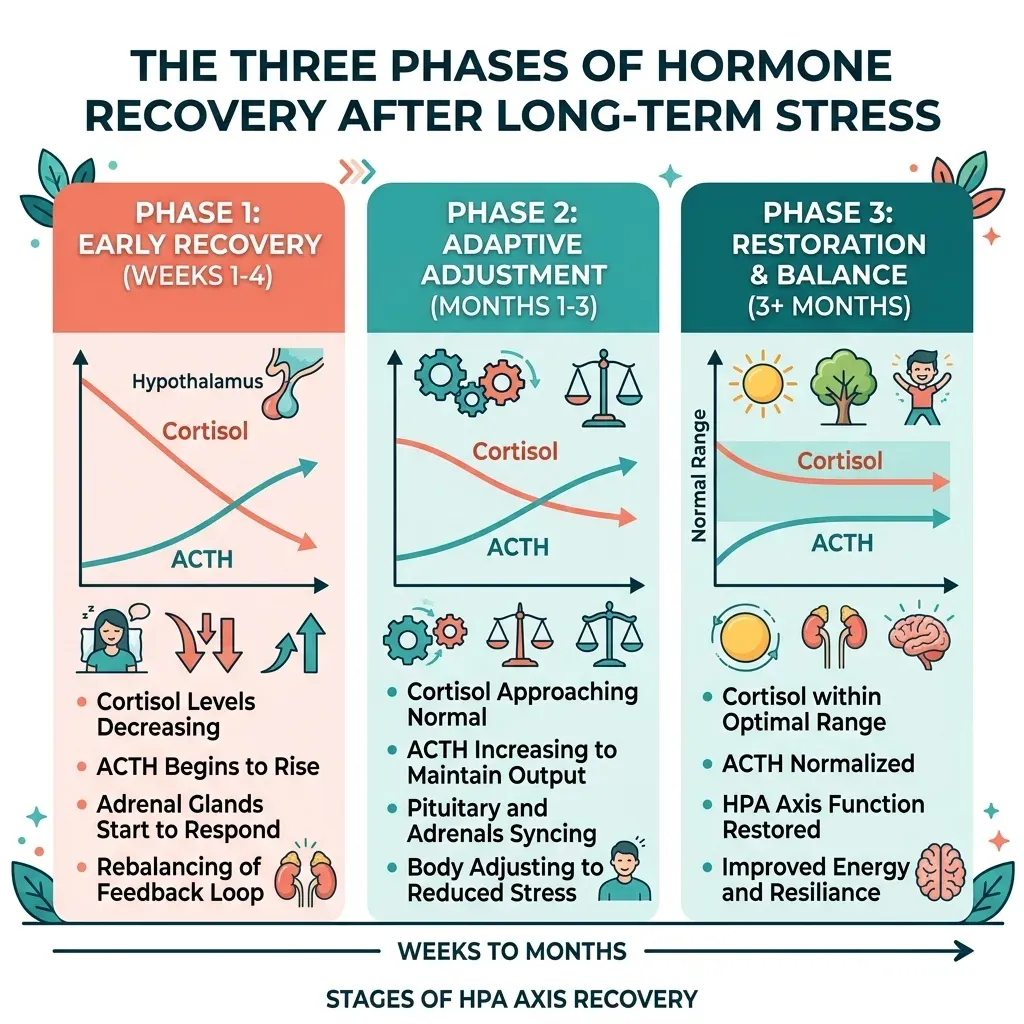
The Weizmann Institute research on gland mass dynamics fills in a crucial piece of this picture. After prolonged stress, the HPA axis doesn't snap back to normal immediately. Recovery follows three distinct phases spanning weeks to months. In early withdrawal, cortisol remains elevated while ACTH responses are blunted. In an intermediate phase lasting two to six weeks, cortisol normalizes but ACTH stays suppressed. Full recovery may not arrive for several months. The researchers also found that strong glucocorticoid receptor feedback protects against dysregulation, while chronic stress induces glucocorticoid resistance — creating what they describe as a vicious cycle where "prolonged stress makes the HPA less resilient to the next prolonged stress."
Someone can feel progressively worse over time without their adrenal glands being "tired." The problem isn't production capacity — it's signal calibration. The thermostat is miscalibrated, not the furnace.
A study on overtraining syndrome in athletes provides concrete evidence for this distinction. Cadegiani and Kater tested 51 participants using gold-standard endocrine tests and found that overtrained athletes showed blunted cortisol and ACTH responses to insulin-induced hypoglycemia — but their adrenal glands responded normally when stimulated directly with synthetic ACTH. The dysfunction was central, originating in the hypothalamus and pituitary, not the adrenal glands themselves. The overtrained athletes' responses resembled sedentary controls, suggesting they'd lost their adaptive hormonal conditioning rather than developed a new disease.
| HPA Axis Pattern | What's Happening | Associated Conditions |
|---|---|---|
| Hypercortisolism | Elevated baseline cortisol, exaggerated stress response | Acute/subacute stress, depression, anxiety disorders |
| Hypocortisolism | Reduced cortisol output, flattened daily rhythm | Chronic fatigue, burnout, PTSD, fibromyalgia |
| Blunted reactivity | Normal baseline but weak response to new stressors | Overtraining syndrome, prolonged chronic stress |
| Enhanced negative feedback | System over-suppresses cortisol after release | CFS, post-traumatic states |
Childhood adversity adds another layer. A review published in ISRN Neuroscience found that approximately 50% of chronic fatigue syndrome patients reported at least one type of childhood trauma, and that early adversity increases CFS risk by six- to eightfold. The mechanism involves epigenetic modifications — chemical tags on DNA that alter how genes are expressed without changing the genetic code itself. Specifically, childhood trauma increases methylation of the glucocorticoid receptor gene (NR3C1), reducing receptor expression in the hippocampus and permanently altering how the brain calibrates stress responses.
The Symptoms Are Real, But They Point Somewhere Else
The symptom list attributed to "adrenal fatigue" — persistent tiredness, brain fog, trouble sleeping, salt cravings, afternoon energy crashes, difficulty recovering from exercise or illness — captures something millions of people genuinely experience. Dismissing the label shouldn't mean dismissing the suffering. The question is: if not depleted adrenal glands, then what?
The Endocrine Society's position statement notes that these symptoms are "common and non-specific, meaning they can be found in many diseases." Here are some of the more frequently overlooked ones:
| Symptom | Commonly Attributed To | Conditions Actually Worth Investigating |
|---|---|---|
| Persistent fatigue | "Adrenal fatigue" | Hypothyroidism, sleep apnea, iron deficiency, depression, chronic fatigue syndrome |
| Brain fog | "Adrenal fatigue" | Sleep disorders, thyroid dysfunction, B12 deficiency, medication side effects |
| Afternoon energy crashes | "Adrenal fatigue" | Blood sugar dysregulation, poor sleep quality, circadian rhythm disruption |
| Salt/sugar cravings | "Adrenal fatigue" | Electrolyte imbalance, insulin resistance, stress eating patterns |
| Dizziness on standing | "Adrenal fatigue" | POTS, orthostatic hypotension, dehydration, medication side effects |
| Exercise intolerance | "Adrenal fatigue" | Overtraining syndrome, cardiac conditions, chronic fatigue syndrome |
Cleveland Clinic's Dr. Rao specifically flags postural orthostatic tachycardia syndrome (POTS) as "a surprisingly common condition" that gets missed when patients accept the adrenal fatigue label. POTS involves dysfunction of the autonomic nervous system — the same system that works hand-in-hand with the HPA axis — and causes fatigue, brain fog, dizziness, and exercise intolerance that overlap significantly with "adrenal fatigue" complaints. It's treatable, but only if properly diagnosed.
Thyroid conditions, particularly Hashimoto's thyroiditis, create another common overlap. The thyroid and adrenal systems interact closely, and hypothyroidism can produce fatigue, weight changes, brain fog, and cold sensitivity that mirror "adrenal fatigue" symptoms point by point. A simple TSH blood test can screen for this.
The research on flattened diurnal cortisol patterns in cancer patients adds something important to this picture. A 2024 systematic review of 17 studies found that 16 showed altered HPA axis function in cancer patients, with flattened daily cortisol curves correlating with fatigue, sleep disturbance, memory problems, and reduced well-being. These are the same symptoms attributed to "adrenal fatigue" — but they're emerging from a disturbed cortisol rhythm, not depleted glands.
Testing and Diagnosis: What Cortisol Results Actually Mean
If you've searched "adrenal fatigue testing" online, you've probably encountered offers for salivary cortisol panels, sometimes costing hundreds of dollars, that promise to reveal whether your adrenal glands are functioning properly. The gap between what these tests measure and what they can tell you is worth understanding before you spend that money.
Salivary cortisol provides a snapshot of free cortisol at the moment of collection. For diagnosing actual adrenal insufficiency, endocrinologists rely on the ACTH stimulation test — a standardized procedure where synthetic ACTH is administered and cortisol response is measured over 60 minutes. This test directly evaluates whether the adrenal glands can physically produce cortisol when stimulated. If they can (and in people labeled with "adrenal fatigue," they consistently can), the glands aren't the problem.
The 2016 systematic review was explicit about this: the "most appropriate methods to assess the HPA axis were not used to evaluate fatigue" in the studies that proponents cite. Salivary cortisol measurements are influenced by dozens of variables — collection timing, sleep-wake patterns, oral health, food intake, medication, menstrual cycle phase, recent exercise, and psychological state at the moment of spitting into a tube. Two samples from the same person taken an hour apart can look dramatically different.
There's a more fundamental issue with the testing narrative. Even when salivary cortisol patterns do show abnormalities — like a blunted cortisol awakening response — this doesn't point to "fatigued" glands. The overtraining syndrome research demonstrated that cortisol awakening response was 32.4% in overtrained athletes compared to 62.2% in healthy athletes, but direct adrenal stimulation produced identical responses across all groups. The blunting was happening upstream, in the brain's signaling to the adrenals.
When cortisol patterns look abnormal in someone with fatigue, the appropriate clinical response isn't purchasing supplements to "support" the adrenals — it's investigating what's actually driving the HPA axis disruption: undiagnosed sleep disorders, chronic psychological stress, thyroid dysfunction, autoimmune conditions, or psychiatric disorders that require their own specific treatments.
The Endocrine Society warns that taking adrenal hormone supplements without a legitimate diagnosis risks suppressing your body's natural cortisol production. This suppression can persist for months after stopping the supplements, and in extreme cases can precipitate adrenal crisis — the very emergency that actual adrenal insufficiency patients work to prevent.
Evidence-Based Approaches to Supporting Your Stress Response
Rejecting the "adrenal fatigue" label doesn't mean accepting that nothing can be done about chronic fatigue and stress-related symptoms. The research on HPA axis dysregulation points to several well-supported strategies — none of which involve adrenal supplements or cortisol replacement in people with functioning glands.
Address the underlying condition first. If chronic stress has been disrupting your sleep, energy, and cognitive function, the single most productive step is a thorough medical evaluation. This means not settling for the first practitioner who offers a label. Request thyroid panels (TSH, free T4, T3, and thyroid antibodies), complete blood count, iron studies, vitamin B12, fasting glucose, and discuss screening for sleep disorders. Rule out the diagnosable conditions that mimic "adrenal fatigue" before accepting an unvalidated one.
Protect your cortisol rhythm. Research on HPA axis function consistently shows that the daily cortisol pattern — the circadian rhythm of rising in the morning and falling at night — matters more than total cortisol output. A review in Cureus found that "distinctly flattened diurnal cortisol levels have been linked to chronic fatigue syndrome, burnout, and insomnia." Protecting this rhythm means consistent wake times, morning light exposure, limiting evening screen exposure, and avoiding late-night eating — all of which help anchor your body's cortisol clock.
Use exercise strategically. Physical activity is one of the most potent HPA axis modulators available, but the dose-response relationship matters. The overtraining syndrome research shows that exercise can shift HPA function in both directions — regular moderate training builds adaptive hormonal conditioning, while excessive training without recovery erodes it. For people feeling fatigued and stressed, moderate aerobic activity — walking, swimming, cycling at conversational pace — is likely more restorative than intense workouts.
Take stress recovery seriously. The Weizmann Institute model showed that HPA axis recovery after prolonged stress takes weeks to months, with three distinct phases. This has a practical implication: if you've been under sustained pressure (caregiving, financial strain, demanding work, relationship conflict), removing the stressor is necessary but not sufficient. Your neuroendocrine system needs time to recalibrate. Cognitive behavioral therapy has been shown to increase cortisol levels in chronic fatigue patients by helping reverse patterns induced by low activity, depression, and early-life stress.
Be cautious with adaptogens. Ashwagandha, rhodiola, and other adaptogenic herbs have some evidence for modulating cortisol levels, but the studies are typically small and short-term. They're not a substitute for addressing root causes. If you choose to try them, disclose this to your physician — some adaptogens interact with thyroid medications and can confound diagnostic testing.

Frequently Asked Questions
Is adrenal fatigue a real medical diagnosis?
No. Neither the Endocrine Society nor any major medical organization recognizes adrenal fatigue as a validated diagnosis. A 2016 systematic review of 58 studies found no consistent evidence that fatigued people have reduced adrenal function. The symptoms attributed to adrenal fatigue are real, but they stem from other identifiable conditions — not from depleted adrenal glands.
What's the difference between adrenal fatigue and adrenal insufficiency?
Adrenal insufficiency (including Addison's disease) is a medically recognized condition where the adrenal glands are genuinely damaged and cannot produce adequate hormones. It causes severe symptoms like dangerously low blood pressure, significant weight loss, and can trigger life-threatening adrenal crisis. It requires lifelong hormone replacement therapy and is diagnosed through the ACTH stimulation test. "Adrenal fatigue" is an unvalidated concept proposing a milder version of this, but testing consistently shows normal adrenal function in people given this label.
Can chronic stress actually damage my adrenal glands?
Chronic stress doesn't damage adrenal glands — it actually causes them to enlarge temporarily. The real impact of chronic stress is on the signaling system (the HPA axis) that controls the glands. Prolonged stress can dysregulate this signaling, leading to altered cortisol patterns, blunted stress responses, and symptoms like fatigue and brain fog. The dysfunction is in the brain's regulation of the system, not in the glands themselves.
Should I take cortisol tests if I suspect adrenal fatigue?
Over-the-counter salivary cortisol panels marketed for "adrenal fatigue" have significant limitations — they're highly variable and not validated for this purpose. If you're experiencing persistent fatigue, see an endocrinologist who can order appropriate testing including the ACTH stimulation test, thyroid panels, and screening for sleep disorders. These tests can identify treatable conditions that standard cortisol panels miss.
Are adrenal support supplements safe to take?
Supplements marketed for "adrenal support" range from relatively harmless vitamins and adaptogens to products containing actual hormone precursors like DHEA or adrenal glandular extracts. The Endocrine Society warns that taking adrenal hormones without a legitimate deficiency can suppress your body's natural production for months, potentially triggering the very crisis these supplements claim to prevent. Any supplement regimen should be discussed with a physician first.
Related Articles
- The Hidden Toll of Low-Level Stress: How Chronic Tension Wrecks Your Hormones and How to Fix It — A deeper look at how everyday stress reshapes your hormonal landscape and practical recovery strategies.
- How Cortisol Drives Weight Gain and What Actually Helps — The connection between chronic cortisol elevation, visceral fat accumulation, and evidence-based interventions.
- Thyroid Health and Hashimoto's: Symptoms, Diet, and Natural Support — Understanding the thyroid conditions that frequently mimic "adrenal fatigue" symptoms.
- Ashwagandha Benefits, Dosage, and Side Effects — What the research shows about this widely promoted adaptogen for stress and cortisol management.
- The Real Damage Anxiety and Burnout Do to Your Body — The biological toll of sustained anxiety and burnout on your nervous and endocrine systems.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











