What BPC-157 Is and Why Joint Repair Became a Popular Use
BPC-157 sits in an odd place: it is discussed online like a recovery shortcut, studied in labs like a repair signal, and treated by regulators like an unapproved drug. The part that makes the oral-versus-injection debate so persistent is simple. A sore knee, a stubborn tendon, or a ligament strain feels local. A capsule feels easier. A shot feels more targeted. The question is whether either route has human evidence strong enough to support the promise.
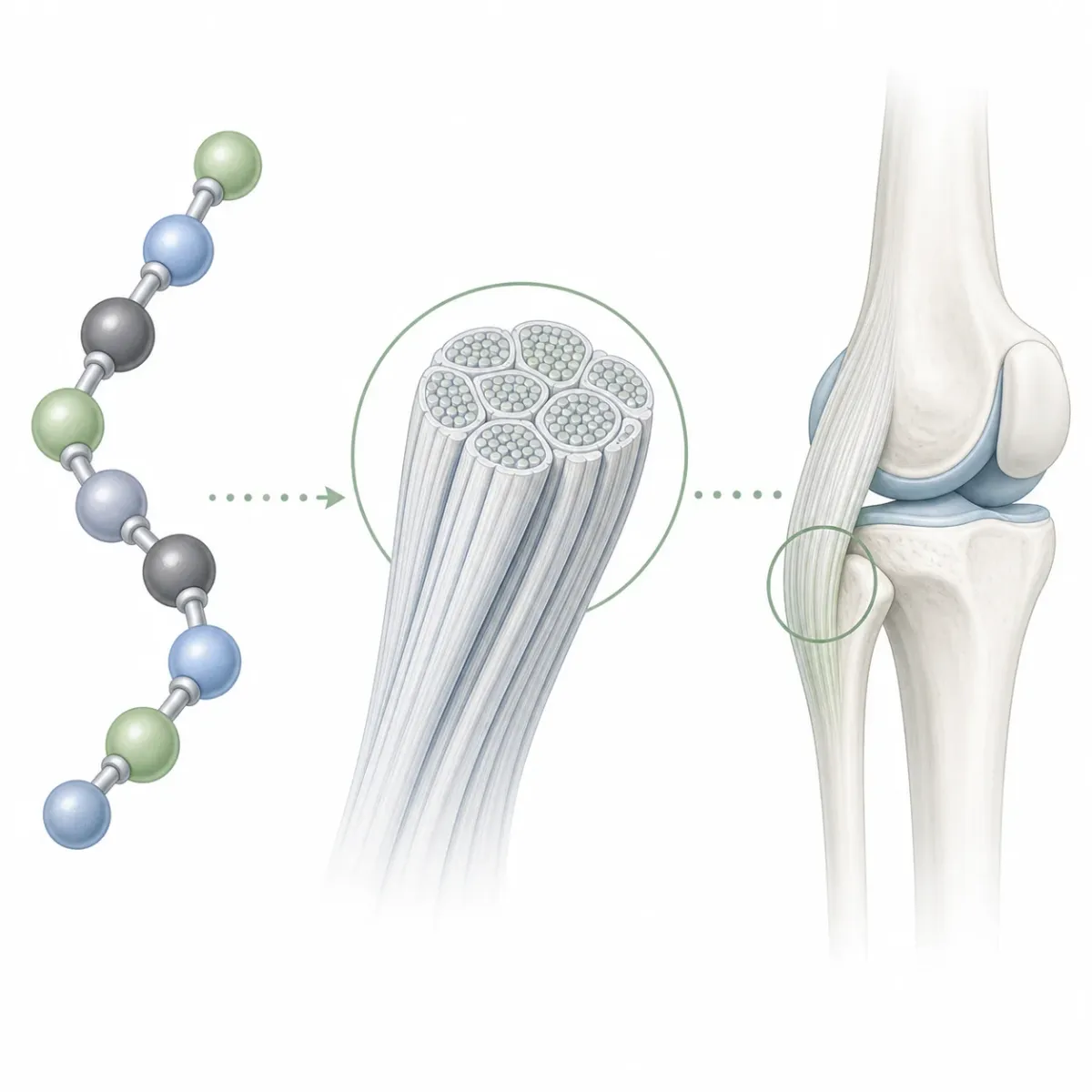
The compound itself is not a vitamin or a normal dietary supplement. BPC-157 is described as a synthetic pentadecapeptide with a 15-amino-acid chain, and the same review lists its sequence as Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val. Think of that sequence like a very short instruction strip. It is far smaller than a full protein, but still specific enough that changing the route, dose, purity, or formulation could matter.
Joint-repair interest grew because animal and cell studies kept pointing in a similar direction: tissue repair, blood-vessel signaling, tendon remodeling, and inflammation control. But the human evidence is much thinner. An orthopedic sports medicine systematic review found 36 eligible BPC-157 studies, with 35 preclinical studies and 1 clinical study. That ratio is the whole story in miniature. There is a lot of biological smoke. There is not yet much clinical fire.
This matters because "joint repair" is a heavy phrase. Pain going down after an intervention is useful, but it is not the same as rebuilding cartilage, reconnecting tendon to bone, or restoring ligament strength. For a treatment to deserve that language, researchers need to show structural or functional change, ideally against a comparison group. Most BPC-157 discussion skips that standard and jumps straight from mechanism to outcome.
The practical read: BPC-157 is interesting enough to study, but not established enough to treat oral capsules or injections as proven joint-repair therapies.
How BPC-157 Might Work in Tendons and Ligaments
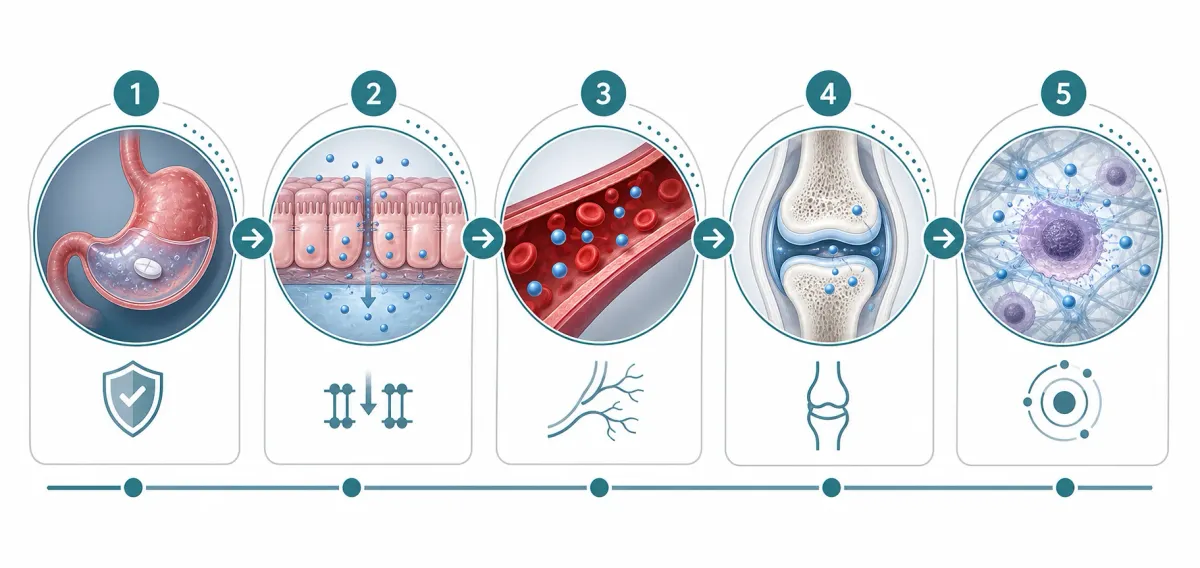
The most credible argument for BPC-157 is not that it magically rebuilds cartilage. It is that several repair pathways appear to move in a direction that could matter for soft tissue. Review authors describe nitric oxide signaling as one of the peptide's main proposed molecular targets. Nitric oxide matters because, in tissue repair, it behaves a bit like a traffic signal for blood flow, vessel tone, and inflammatory response.
Another major thread is angiogenesis, the formation of new blood vessels. The same review connects BPC-157 with VEGFR2-related pro-angiogenic signaling. For an injured tendon, better microcirculation could be useful because tendons are often poorly vascularized. Picture a construction site with too few access roads. More roads can help supplies arrive, but random road-building does not guarantee a well-built bridge.
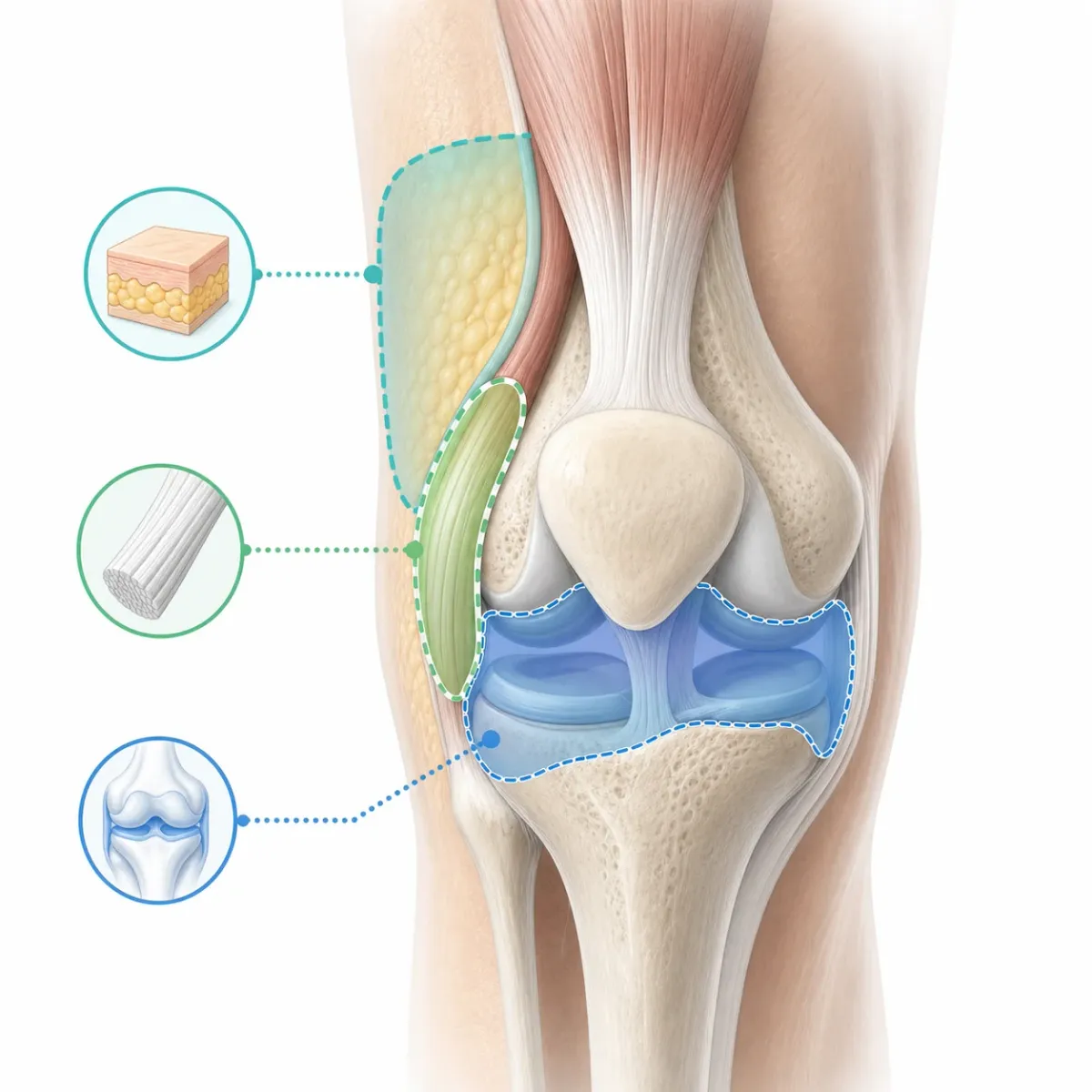
Tendon and ligament repair also depends on how fibroblasts behave. These are the cells that help lay down and organize collagen. A tendon and ligament review summarizes preclinical findings involving fibroblast activity, collagen remodeling, and FAK-paxillin signaling. That is the biochemical reason people talk about BPC-157 for tendon and ligament injuries rather than only for gut irritation.
Still, collagen remodeling is not automatically good. The body has to place new collagen in the right orientation, with the right stiffness, at the right time. Bad remodeling can leave tissue thick, painful, or poorly organized. That is why a pathway that looks helpful in a controlled injury model should be tested carefully in real patients, where age, training load, medications, inflammation, and old scar tissue all complicate the repair job.
The caution is that mechanism is not medicine. A pathway can look impressive in a dish or a rodent model and still fail when tested in people with messy, chronic injuries. The best practical takeaway is to treat mechanism claims as a reason for better trials, not as proof that a capsule or injection will repair your joint.
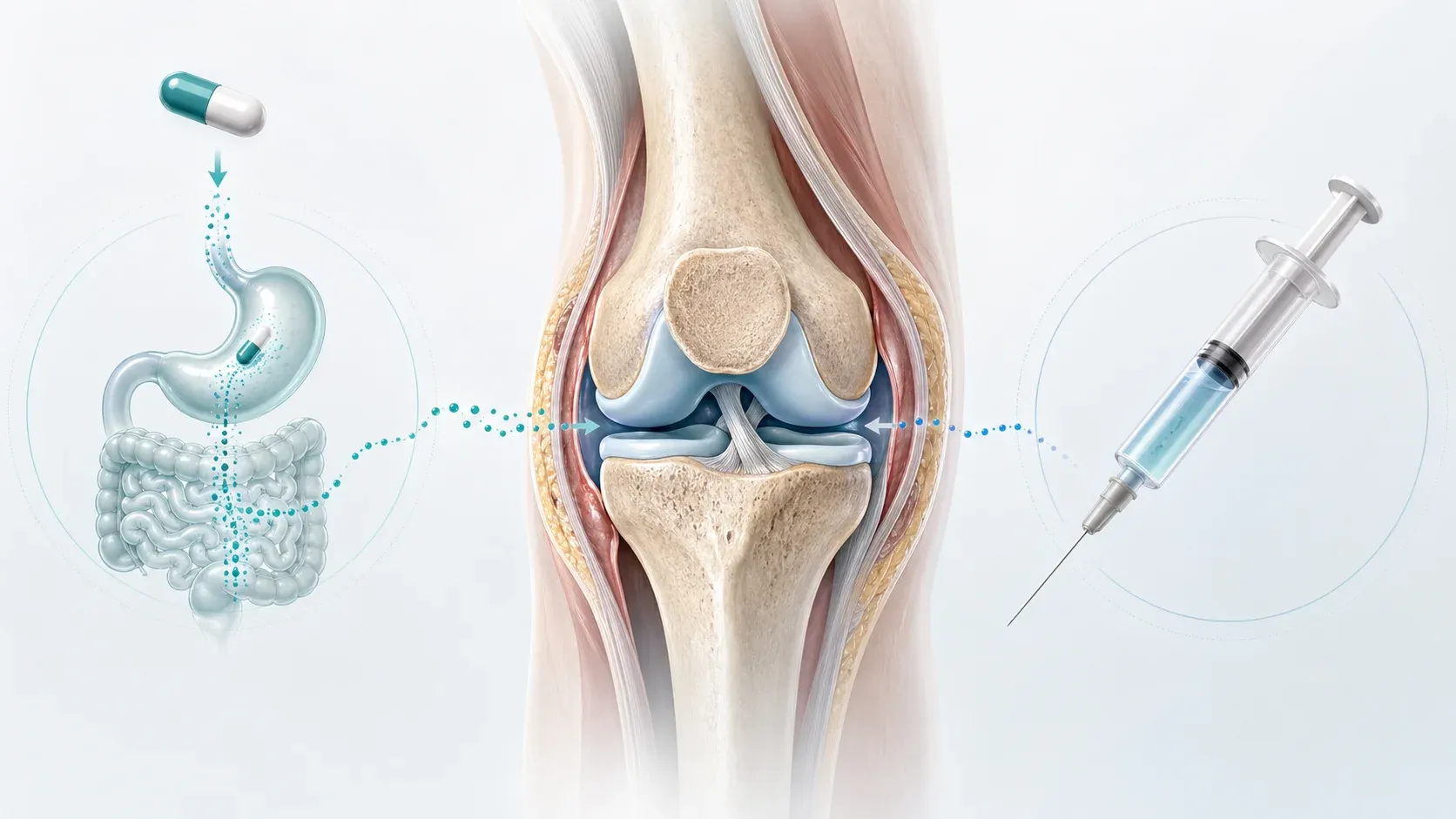
The Oral Route: Stable in the Stomach Is Not the Same as Proven in Joints
Oral BPC-157 has one unusually good talking point: stability. Many peptides are chewed up quickly in the digestive tract. BPC-157 is different enough that a Frontiers review describes it as stable in human gastric juice for more than 24 hours. That matters because a peptide cannot help anywhere if it is destroyed before absorption even begins.
But stomach stability is only the first gate. The harder question is what happens after that. Does enough of the oral compound cross into circulation? Does it survive metabolism? Does it reach an injured joint at a relevant concentration? Does it do so consistently across products? A review of local and systemic peptide therapies notes that oral and intra-articular routes each have advantages, but both face limitations in bioavailability and absorption.
That distinction gets lost in marketing. "Stable in gastric juice" often gets translated into "oral works systemically," but those are not the same claim. The first is like saying a package survived the mailroom. The second is saying it reached the correct apartment, was opened by the right person, and contained enough usable material to fix the plumbing.
| Oral claim | What it supports | What it does not prove |
|---|---|---|
| Stable in gastric juice | The peptide may survive digestion better than many peptides | That enough reaches a knee, tendon, or ligament |
| Easier than injections | Lower barrier to use and no needle injury | Greater joint-repair efficacy |
| Systemic exposure | Potential whole-body distribution | Reliable dosing at the injured site |
There is also a clinical-trial clue that helps frame the issue. ClinicalTrials.gov lists a safety and pharmacokinetics study of oral PCO-02, a BPC-157-related oral compound, but that record is not a joint-repair efficacy trial. For a reader deciding between forms, that means oral BPC-157 is plausible, convenient, and still not proven for joint repair.
The oral route also creates a product-quality problem that consumers rarely see. A capsule has to contain the expected ingredient, protect it through storage, dissolve predictably, and deliver a consistent amount. If the active material is degraded, under-dosed, mislabeled, or contaminated, the route debate becomes irrelevant. You are no longer comparing oral with injection; you are comparing unknown products with unknown exposure.
For gut-focused claims, oral delivery has a more intuitive story because the compound passes through the digestive tract. For joint repair, the story gets longer and weaker. The capsule has to become a systemic exposure, then a tissue exposure, then a meaningful repair signal. Each step adds uncertainty. That does not make oral BPC-157 useless by definition, but it does make confident joint-repair claims premature.
The Injectable Route: Local Delivery Has Better Logic, Not Better Proof
Injectable BPC-157 sounds more convincing because the route matches the problem. If the pain is in a knee, putting a compound near or inside that area feels more rational than hoping an oral dose arrives there. In drug-delivery terms, local administration is like dropping supplies at the job site instead of sending them through a regional warehouse first.
The best-known human joint data are local, not oral. A retrospective knee-pain chart review reported that 17 patients received intra-articular peptide treatment, 16 were contacted for follow-up, and 12 had received BPC-157 alone. In the BPC-157-only group, 11 of 12 patients, or 91.6%, reported significant knee-pain improvement. Those numbers explain why injections get attention.
They also show why the evidence is fragile. The same PubMed abstract says no specific tools were used to measure function, quality of life, stiffness, or activities of daily living. The published PDF adds other caveats: patients paid for treatment, objective testing was limited, and the procedure was performed without ultrasound guidance. That does not make the result meaningless, but it does make it a signal, not a verdict.
| Injection type | Why people use it | Main evidence problem |
|---|---|---|
| Subcutaneous | Slower systemic absorption without entering a joint | Little joint-specific human evidence |
| Local peri-tendon | Targets tissue near the injury | Depends heavily on anatomy, sterility, and clinical judgment |
| Intra-articular | Places material inside the joint space | Small, uncontrolled human evidence and injection-specific risks |
The practical implication is uncomfortable but clear. Injection has the better joint-specific logic and the better human signal, but it also has higher procedural risk and still lacks the trial quality needed for confidence. Local does not automatically mean proven.
It also does not automatically mean safer. A joint space is not a casual target. Sterility, needle placement, anatomy, anticoagulant use, immune status, and the exact diagnosis all matter. A poorly chosen injection can add risk without answering the biological question. This is one reason route conversations belong in a clinical setting, not in a shopping cart.
Subcutaneous use sits between those two worlds. It avoids entering the joint, but it also gives up the strongest argument for local delivery. In practice, many online protocols blur subcutaneous, intramuscular, peri-tendon, and intra-articular use as if they were interchangeable. They are not. Different tissue compartments can mean different exposure, different risks, and different clinical questions.
Oral vs. Injection: What the Evidence Actually Lets Us Say
If you want the clean answer, here it is: there is no reliable head-to-head human trial showing that oral BPC-157 is better than injected BPC-157, or that injected BPC-157 is better than oral BPC-157, for joint repair. The orthopedic systematic review found only 1 clinical study among the eligible orthopedic literature, and that study was local injection for knee pain, not a route-comparison trial.
So the route decision is not evidence versus evidence. It is convenience and plausibility on the oral side versus localized delivery and limited human signal on the injection side. That is a weaker foundation than most online discussions admit.
| Question | Oral BPC-157 | Injectable BPC-157 |
|---|---|---|
| Best argument | Gastric stability and convenience | More direct delivery to or near joint tissue |
| Best human joint evidence | Not established | Small retrospective knee-pain chart review |
| Main weakness | Bioavailability and joint exposure are uncertain | Procedural risk and weak clinical-trial quality |
| Bottom line | More convenient, less joint-specific evidence | More targeted, still unproven |
For joint repair specifically, pain relief and tissue repair are also not identical. Someone can feel better because inflammation calms down, because activity changes, because the natural healing timeline finally catches up, or because a treatment truly improved tissue structure. Without imaging, functional testing, controls, and follow-up, those explanations blur together.
That is why route arguments should be framed modestly. Oral may make more sense for people interested in systemic or gut-related hypotheses, though joint evidence is weak. Local injection may make more sense as a research route for joint questions, but it should be studied under proper clinical oversight. Neither route has earned the kind of certainty that online protocols often suggest.

What Doctors and Researchers Actually Recommend Now
Sports medicine sources are not saying BPC-157 is biologically boring. They are saying the clinical proof is not there yet. AOSSM authors note that animal models report improved healing signals but that high-quality human clinical evidence is lacking. That is the professional stance most consistent with the evidence: curiosity, caution, and no overpromising.
Regulatory status matters too. Operation Supplement Safety describes BPC-157 as an unapproved drug and lists it as prohibited. OPSS also says there is little to no reliable scientific evidence supporting its safety or effectiveness in humans. For tested athletes, that is not a footnote. It can affect eligibility, sanctions, and career risk.
Safety questions are not limited to the molecule. The product matters. The vial matters. The supplier matters. Sports medicine authors warn about purity, dosing, composition, contamination, sterility, injection-site irritation, allergic reactions, and drug interactions. An online vial labeled "research chemical" is not equivalent to an FDA-approved injectable drug manufactured under a regulated pathway.
The most useful medical conversation is not "oral or injection?" It is "what diagnosis are we treating, what proven options have been tried, what outcome are we measuring, and what risk are we accepting?" A torn meniscus, patellar tendinopathy, inflammatory arthritis, and nonspecific knee pain are different problems. A route choice cannot fix a fuzzy diagnosis.
For readers, the practical recommendation is to be more skeptical than the marketing but more nuanced than a blanket dismissal. If you are considering BPC-157, especially an injection, involve a qualified clinician, ask about legal and sport-testing implications, and do not let peptide experiments replace diagnosis, rehab, load management, sleep, nutrition, or treatments with stronger clinical evidence.
A useful litmus test is whether the plan defines success before treatment begins. "My knee feels better" is important, but it is vague. Better markers might include a pain score during a specific movement, range of motion, return-to-running tolerance, strength symmetry, imaging when appropriate, or a clinician-guided function test. If a treatment cannot be judged against a defined outcome, it is easy to mistake hope for progress.
The safest posture is not fear; it is sequence. Confirm the injury. Use the boring basics that reliably move tissue adaptation: progressive loading, adequate recovery, enough protein, sleep, and time. Then, if an experimental peptide still comes up, it can be weighed against a real baseline instead of becoming the first serious plan.

Frequently Asked Questions
Is oral BPC-157 proven to repair joints?
No. Oral BPC-157 has a plausible stability argument, but route-of-administration research still flags bioavailability and absorption as key limitations. Joint repair requires evidence that the compound reaches the injured tissue and improves meaningful outcomes, rather than merely surviving the stomach.
Are BPC-157 injections proven to work better than capsules?
No head-to-head human trial proves that. The injection route has a stronger local-delivery argument, and one small knee-pain chart review reported improvement after intra-articular BPC-157, but that study was uncontrolled and subjective.
Why do so many people report benefits if the evidence is weak?
Real improvement can happen for many reasons: natural recovery, changed training load, physical therapy, placebo response, reduced inflammation, or a true biological effect. Without controlled trials, those explanations are difficult to separate.
Is BPC-157 legal or allowed for athletes?
OPSS describes BPC-157 as prohibited and unapproved. Athletes subject to anti-doping rules should treat it as a serious compliance risk and check their governing body's current rules before using any peptide product.
What should someone do instead of guessing between oral and injection?
Start with a diagnosis. Joint pain can come from cartilage, tendon, ligament, bone, nerve, inflammatory disease, or referred pain. A clinician can match the problem to evidence-based rehab, imaging, medication, injections, or surgical options before experimental peptides enter the conversation.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











