
A $3.75 billion industry built on a protein your body already makes
Your body contains more collagen than any other protein. It forms the scaffolding of cartilage, tendons, bones, and skin. Cartilage alone is roughly 60% collagen by dry weight, which is why the supplement industry zeroed in on it as a joint-health ingredient.
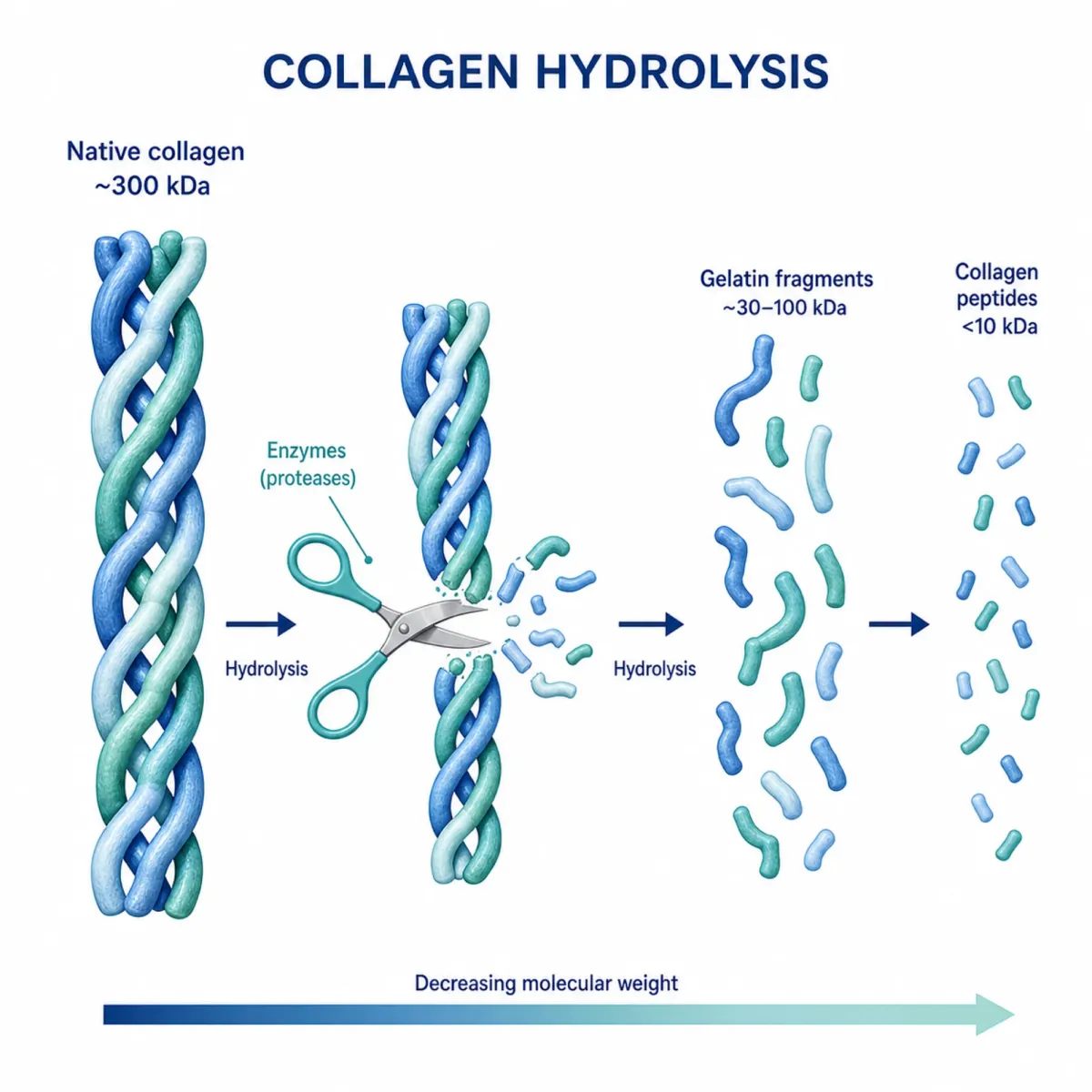
Collagen peptide powder is the hydrolyzed form of this protein. Manufacturers take animal collagen (usually from bovine hides, chicken bones, or fish scales), apply heat to break the triple-helix structure, then use enzymes to chop it into small peptide fragments. The result: low molecular weight peptides under 6 kilodaltons that dissolve in liquid, have no taste, and are marketed as easily absorbable.
Native collagen is a large, tightly wound protein your gut can barely break down. Hydrolyzed collagen peptides are already pre-digested into fragments small enough to cross the intestinal wall. These are the peptides in the tubs at your grocery store and the scoops your coworker stirs into morning coffee.
The collagen supplement market reached an estimated $3.75 billion in 2026, growing at over 9% annually. The broader collagen market spanning food, cosmetics, and biomedical applications hit $10.4 billion in 2024 and is projected to more than double by 2033. That kind of money creates pressure to sell before the science catches up. So has the science caught up for joint relief?
Do collagen peptides actually reach your joints, or just get digested like any other protein?
The most common objection to collagen supplements goes like this: your body breaks down ingested protein into amino acids, redistributes them wherever it needs protein, and collagen powder is no different from eating chicken breast. If that were the whole story, collagen supplements would be an expensive protein source with no joint-specific benefit.
Steffen Oesser's research group changed this conversation in 1999. They fed mice radioactively labeled (14C) gelatin hydrolysate and tracked where the radioactivity ended up. It accumulated in cartilage tissue. This was the first direct evidence that orally ingested collagen fragments don't just dissolve into the general amino acid pool. They survive digestion as identifiable peptides and concentrate in joint cartilage.
Think of it like putting a GPS tracker on individual Lego bricks after they've been through a washing machine. You'd expect them to come out scattered everywhere. Instead, some of them reliably end up in the same specific drawer. That's what the radiotracer showed for collagen peptides and cartilage.
Later research filled in the details. Specific dipeptides like prolyl-hydroxyproline (Pro-Hyp) and tripeptides like Pro-Hyp-Gly reach joint tissues and accumulate there. A review by Bello and Oesser confirmed that collagen hydrolysate fragments cross the intestinal wall and accumulate in cartilage, where they appear to stimulate chondrocytes (cartilage-maintaining cells) to produce new matrix components.
Nearly half of digested gelatin is absorbed from the intestine in peptide form rather than as individual amino acids. So the "it's just protein" dismissal is too simple. Collagen peptides do reach joints. Whether they arrive in quantities sufficient to produce meaningful clinical improvement is a separate question, and the one that matters more.
The evidence: moderate but real, with significant caveats
The clinical trial record for collagen peptides and joint pain is better than most supplement categories manage, but still falls short of what you'd need for strong claims.
Keith Clark's 2008 Penn State study remains one of the most cited. Clark gave 97 varsity and club athletes 10 grams of collagen hydrolysate daily for 24 weeks. Compared to placebo, the collagen group reported statistically significant reductions in joint pain when walking (p=0.007), standing (p=0.011), at rest (p=0.025), carrying objects (p=0.014), and lifting (p=0.018). Among participants with knee pain specifically, the differences were even more pronounced, with p-values ranging from 0.001 to 0.027. Clark's group noted this was the first clinical trial of that duration to show joint pain improvement in athletes from collagen supplementation.
Daniel Zdzieblik at the University of Freiburg followed up in 2017 with 139 athletes taking 5 grams daily for 12 weeks. Both groups improved (exercise modification likely contributed), but the collagen group saw 38.4% pain reduction versus 27.9% for placebo. A subsequent trial using the same protocol in 180 young adults with exercise-related knee pain found medium effect sizes: 0.453 for physician-assessed pain and 0.342 for participant-reported pain.
For osteoarthritis rather than activity-related pain, Pedro Benito-Ruiz ran a multicenter RCT with 250 knee OA patients taking 10 grams daily for 6 months. The collagen group showed significant improvement on both visual analog scales and WOMAC pain subscales. Patients with more severe cartilage deterioration benefited most.
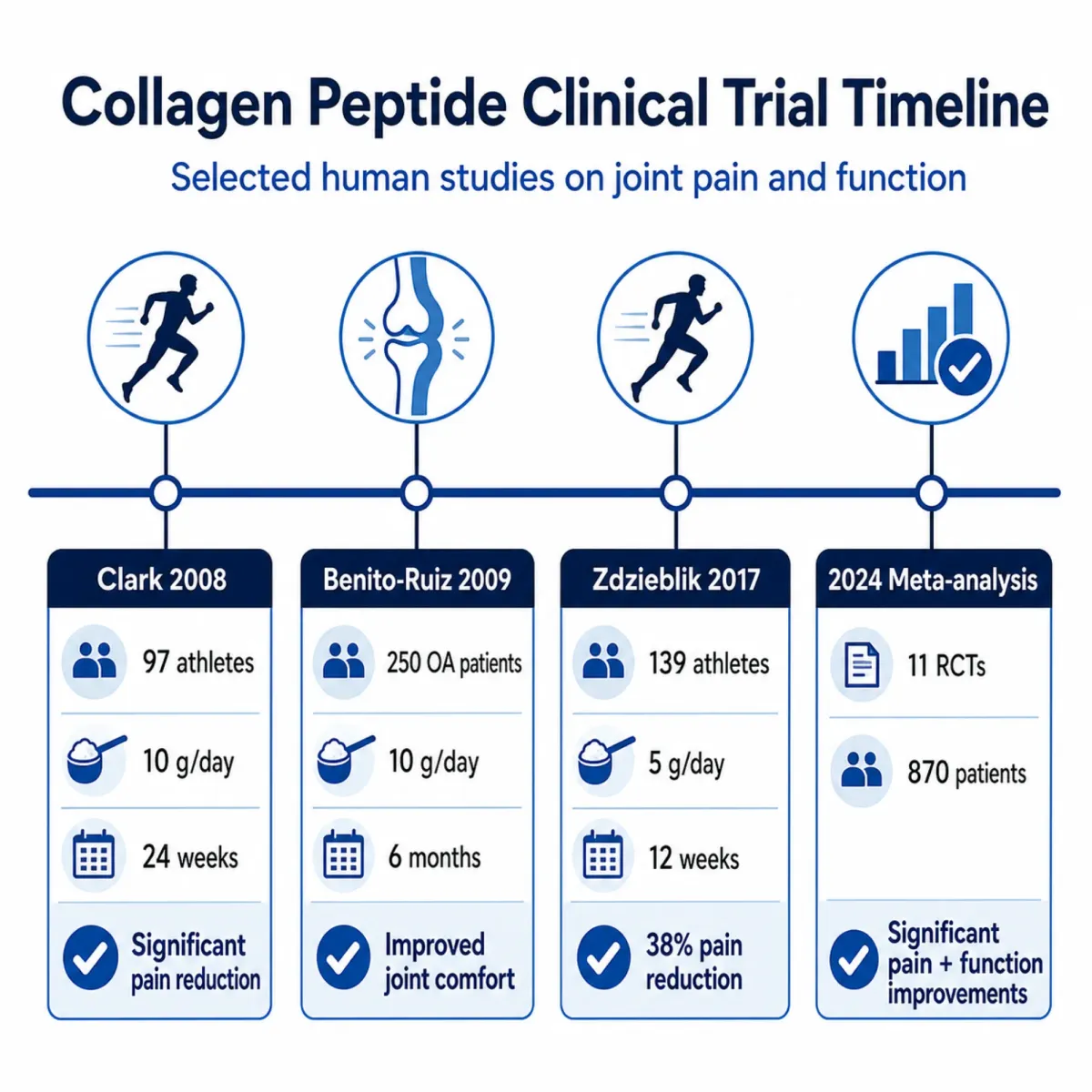
Two meta-analyses published in 2023-2024 attempted to synthesize the evidence. A 2023 analysis of 4 RCTs covering 507 knee OA patients found a standardized mean difference of -0.58 for pain (95% CI -0.98 to -0.18, p=0.004). A larger 2024 analysis of 11 RCTs with 870 participants found mean differences of -13.63 for pain and -6.46 for function, both highly significant (p=0.00001).
Those numbers sound compelling, and they are real. But look closer at the quality assessments. The 2023 meta-analysis rated all four included studies as having high risk of bias using the Cochrane ROB 2.0 tool. The 2024 analysis found heterogeneity of I-squared=88% in pain outcomes, meaning the studies varied wildly in how much benefit they detected. A systematic review of 36 RCTs concluded that "heterogeneity among studies limits the generalizability of findings."
Moderate benefit with moderate evidence quality is a fair summary. The trials consistently show collagen peptides outperform placebo for joint pain, but the effect sizes are small to medium, the studies often have methodological weaknesses, and the optimal dose remains unclear (studies used anywhere from 5 to 10 grams daily).
Two supplements called "collagen" that work through completely different biology
Walk into a supplement store and you'll find two categories of collagen products for joints, both labeled "collagen" despite having almost nothing in common mechanistically.
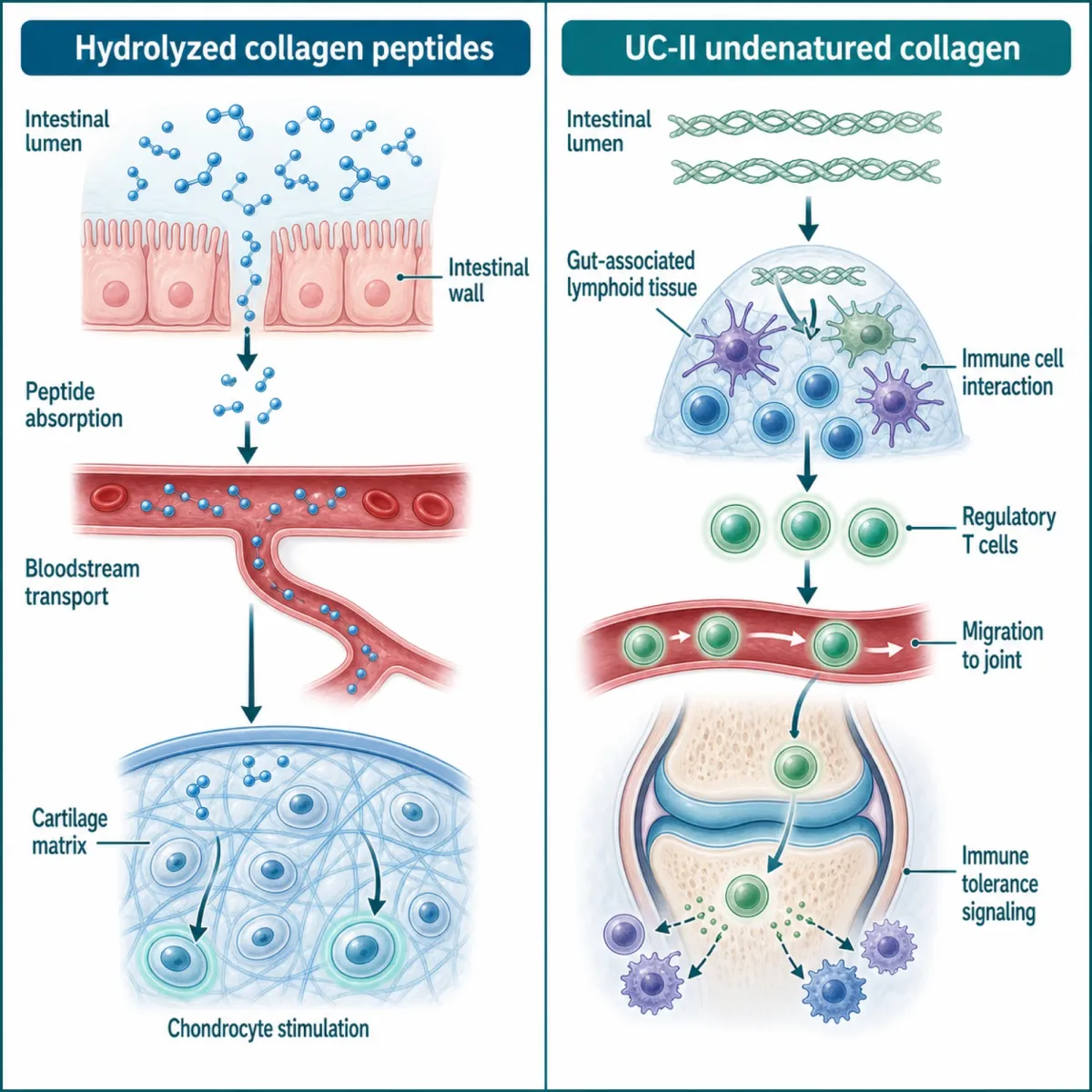
Hydrolyzed collagen (the peptide powder) provides building blocks. Your body absorbs the peptide fragments, some accumulate in cartilage, and they appear to stimulate chondrocytes to produce new extracellular matrix. The dose is 5 to 15 grams daily. It's a nutritional approach: supply the raw materials and hope the body uses them for cartilage maintenance.
UC-II (undenatured type II collagen) works through the immune system. The collagen retains its native triple-helix structure and specific antigenic epitopes. When these intact fragments encounter immune tissue in the gut, they trigger regulatory T cells through a process called oral tolerance. Those T cells then migrate to joints and suppress the inflammatory immune response that damages cartilage. The dose is just 40 milligrams daily, roughly 250 times less than hydrolyzed collagen.
The analogy: hydrolyzed collagen is like shipping lumber to a construction site. UC-II is like calling off the demolition crew. Different problems, different mechanisms.
James Lugo's 2013 study compared them directly. In 55 participants taking 40mg UC-II daily for 4 months, knee extension improved and pain-free exercise duration increased by 2.8 minutes versus 1.4 minutes for placebo. The Arthritis Foundation notes that one trial found 40mg daily of undenatured type II collagen produced significantly less pain and stiffness and better function compared to glucosamine plus chondroitin or placebo after six months.
| Feature | Hydrolyzed collagen (peptides) | UC-II (undenatured type II) |
|---|---|---|
| How it works | Supplies peptide building blocks to cartilage | Modulates immune response via oral tolerance |
| Daily dose | 5-15 grams | 40 milligrams |
| Form | Powder, capsules, liquid | Small capsules only |
| Source | Bovine, marine, porcine, chicken | Chicken sternum cartilage |
| Time to effect | 8-24 weeks in studies | 4-6 months in studies |
| Primary evidence | Pain reduction in OA and athletes | Pain reduction and function in OA |
| Evidence quality | Multiple RCTs, two meta-analyses | Fewer but well-designed RCTs |
Researchers have noted that combining the two in a single meta-analysis is inappropriate since they employ completely different biological mechanisms. If you're evaluating collagen supplements for joints, knowing which type you're considering is the first question to answer.
Harvard and Cleveland Clinic won't tell you to take it, but they won't tell you to stop either
Check what major medical institutions say about collagen supplements and a pattern emerges. Nobody dismisses them. Nobody recommends them either.
Harvard Health's assessment is representative. Dr. Toni Golen, editor of Harvard Women's Health Watch, acknowledges that collagen supplements "do offer some potential benefits" but advises skepticism. The institution's position: "the research that's been done on collagen supplements is still early, and large-scale studies need to confirm these benefits." Harvard's Nutrition Source adds a pointed observation: "most if not all of the research on collagen supplements are funded or partially funded by related industries," which creates potential bias that makes it difficult to assess how effective supplements actually are.
Cleveland Clinic is more cautious. Their collagen page emphasizes a "lack of randomized controlled trials" and notes that the FDA doesn't regulate collagen supplements, so manufacturers aren't required to prove safety or effectiveness before putting products on shelves. They call collagen peptides "possibly effective" for joint pain in knee osteoarthritis, which is the kind of carefully hedged language institutions use when the evidence points in a positive direction but isn't strong enough for a recommendation.
The Arthritis Foundation is the most positive. They reference an analysis of 41 studies concluding collagen "benefited OA and aided cartilage repair," and they publish specific dosage guidance (40mg for UC-II, 2.5-15g for hydrolyzed). Their tone is cautiously optimistic, noting that since collagen is derived from food, "even if you don't get spectacular results, it won't cause any harm."
Collagen supplements appear safe and may provide modest pain relief for osteoarthritis, but the evidence base has gaps. No major medical institution recommends collagen as a first-line joint treatment. Most suggest discussing supplementation with your doctor and prioritizing a balanced diet that supports natural collagen production.
Browse any collagen brand's website and you'll find certainty where the research offers probability. That gap tells you more about the supplement industry than any individual study.
Where the marketing outpaces the science
The collagen supplement market rewards bold claims. A company selling "joint support" in a crowded field needs differentiation, and the easiest differentiator is promising more than competitors. This creates systematic pressure to overstate.
Consider speed claims first. Many brands suggest improvement within 2-4 weeks. Clark's athlete study ran for 24 weeks. Benito-Ruiz tested over 6 months. Zdzieblik's team needed 12 weeks to see separation from placebo. If someone feels better after two weeks of collagen powder, the placebo effect is a more likely explanation than cartilage remodeling.
Then there's the magnitude problem. The actual effect sizes from meta-analyses are small to medium. The standardized mean difference for pain in the 2023 meta-analysis was -0.58. Meaningful, but not dramatic. A noticeable reduction in pain, not the elimination of it. Compare that to the before-and-after testimonials on supplement sites, where customers describe going from "unable to climb stairs" to "running marathons."
The scope of claims is equally stretched. The strongest evidence covers knee osteoarthritis and activity-related joint pain in athletes. Evidence for hip joints, shoulders, fingers, and other sites is much thinner. For rheumatoid arthritis (an autoimmune condition), it's almost nonexistent. Yet collagen powders are marketed for "total joint health" without distinguishing where the research is solid from where it's speculative.
| Marketing claim | What the research actually shows |
|---|---|
| "Rebuilds cartilage" | May stimulate chondrocyte activity; one MRI study showed increased proteoglycan content after 24 weeks at 10g daily |
| "Results in 2-4 weeks" | Clinical benefits observed at 12-24 weeks in controlled trials |
| "Clinically proven" | Multiple RCTs with positive results, but most rated high risk of bias; heterogeneity of 88% across studies |
| "Supports all joints" | Strongest evidence for knee OA and athlete knee pain specifically |
| "Better than glucosamine" | One UC-II study showed superiority; no large head-to-head comparisons for hydrolyzed collagen |
None of this means collagen supplements are worthless. A product can be genuinely helpful for moderate knee pain while simultaneously being oversold as a cure-all for joint degeneration.
Practical guidance for anyone considering collagen for joints
If the evidence interests you enough to try collagen supplementation, the research points toward specific choices that matter more than brand name or price.
For general joint comfort and activity-related pain, hydrolyzed collagen peptides (types I and III) at 5-10 grams daily have the broadest evidence base. For diagnosed osteoarthritis, both hydrolyzed collagen and UC-II have RCT support, with UC-II at 40mg daily offering a lower-volume alternative.
Commit to at least 12 weeks before evaluating results. The clinical trials showing benefit ran 12-24 weeks. If you're not willing to take a supplement daily for three months before judging it, collagen supplementation probably isn't the right approach for you.
Third-party testing matters here more than usual. The FDA does not regulate collagen supplements for efficacy. NSF International, USP, and ConsumerLab provide independent testing that verifies a product contains what the label claims. Harvard's Nutrition Source flags potential heavy metal contamination as a specific concern with collagen products.
And keep expectations grounded in the data. Collagen peptides produce small to medium reductions in joint pain. A person with moderate knee pain who improves from a 6 to a 4 on a 10-point pain scale is a realistic best case based on the trial data.
| Decision factor | What to look for |
|---|---|
| Type for joint pain | Hydrolyzed collagen (types I/III) or UC-II (type II) |
| Daily dose | 5-10g hydrolyzed or 40mg UC-II |
| Minimum trial period | 12 weeks (ideally 24) |
| Quality markers | NSF, USP, or ConsumerLab certification |
| Vitamin C | Supports collagen synthesis; some products include it |
| What to track | Pain during specific activities (stairs, walking, kneeling) |
One detail from the Benito-Ruiz trial worth noting: subjects with worse baseline cartilage deterioration and lower dietary protein intake saw the greatest benefits. If you already eat a high-protein diet, the marginal benefit from collagen peptides may be smaller than someone whose protein intake is low.
Frequently Asked Questions
How long does collagen peptide powder take to help with joint pain?
Clinical trials showing joint pain improvement used supplementation periods of 12 to 24 weeks. Keith Clark's Penn State study ran for 24 weeks at 10 grams daily before reporting significant differences. Zdzieblik's team found measurable improvements at 12 weeks with 5 grams daily. Any product claiming results in days or a couple of weeks is outpacing the published evidence.
Is collagen peptide powder the same as UC-II for joint health?
No. Hydrolyzed collagen peptide powder provides amino acid building blocks absorbed at doses of 5-15 grams daily. UC-II works through immune modulation (oral tolerance) at just 40 milligrams daily. They use different biological pathways, different doses, and should not be compared directly. Some researchers consider combining them in the same meta-analysis inappropriate given their mechanistic differences.
Do collagen supplements have side effects?
The clinical trial record shows a safety profile comparable to placebo, with occasional gastrointestinal discomfort, headaches, or mild digestive changes reported. Harvard's Nutrition Source notes that available research has not shown negative side effects. The bigger safety concern is product quality, since supplements are not FDA-regulated for efficacy and may contain unlisted ingredients or contaminants.
Can I get the same joint benefits from bone broth instead of collagen powder?
Bone broth contains some collagen, but the concentration varies depending on preparation and is generally much lower than supplement doses. The clinical trials used standardized 5-10 gram doses of hydrolyzed peptides processed for bioavailability. Bone broth hasn't been studied in the same controlled way for joint outcomes.
Should I take collagen powder with vitamin C?
Vitamin C is a required cofactor for collagen synthesis. One study found that vitamin C-enriched gelatin at 15 grams increased collagen synthesis markers by 153% from baseline when taken 60 minutes before exercise. Whether adding vitamin C to a collagen supplement meaningfully improves joint outcomes hasn't been tested in isolation, but ensuring adequate vitamin C intake while supplementing collagen is biologically reasonable.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











