
The short version: Senolytic compounds like fisetin and quercetin can selectively destroy senescent "zombie" cells that accumulate with age and drive chronic disease. Animal studies are striking — fisetin extended mouse lifespan even when given late in life. Early human trials of dasatinib plus quercetin have reduced senescent cell burden in people with kidney disease. But the supplements on pharmacy shelves are unregulated, often underdosed, and may interact with medications. Researchers who discovered these drugs say most people should wait for clinical trial data before self-prescribing.
What Happens When Cells Refuse to Die?
Your body replaces billions of cells every day. Most damaged cells either repair themselves or trigger apoptosis — a controlled self-destruct sequence that clears them without causing collateral damage. But some damaged cells do neither. They stop dividing permanently yet refuse to die. These are senescent cells, and researchers have started calling them "zombie cells" because they linger in tissues, metabolically active but functionally useless.
Senescent cells aren't always harmful. During fetal development, they help sculpt fingers and organs. After a wound, they recruit immune cells to the injury site. And when a cell's DNA sustains damage that could turn cancerous, senescence acts as a tumor suppression mechanism — a hard brake on replication that prevents malignant growth.
The problem is accumulation. In young, healthy tissue, the immune system clears senescent cells efficiently. Natural killer cells and macrophages identify them and destroy them. But as we age, two things happen simultaneously: senescent cells form faster (from chronic stress, DNA damage, metabolic dysfunction), and the immune system loses its ability to remove them. The result is a growing population of zombie cells that the body can't get rid of.
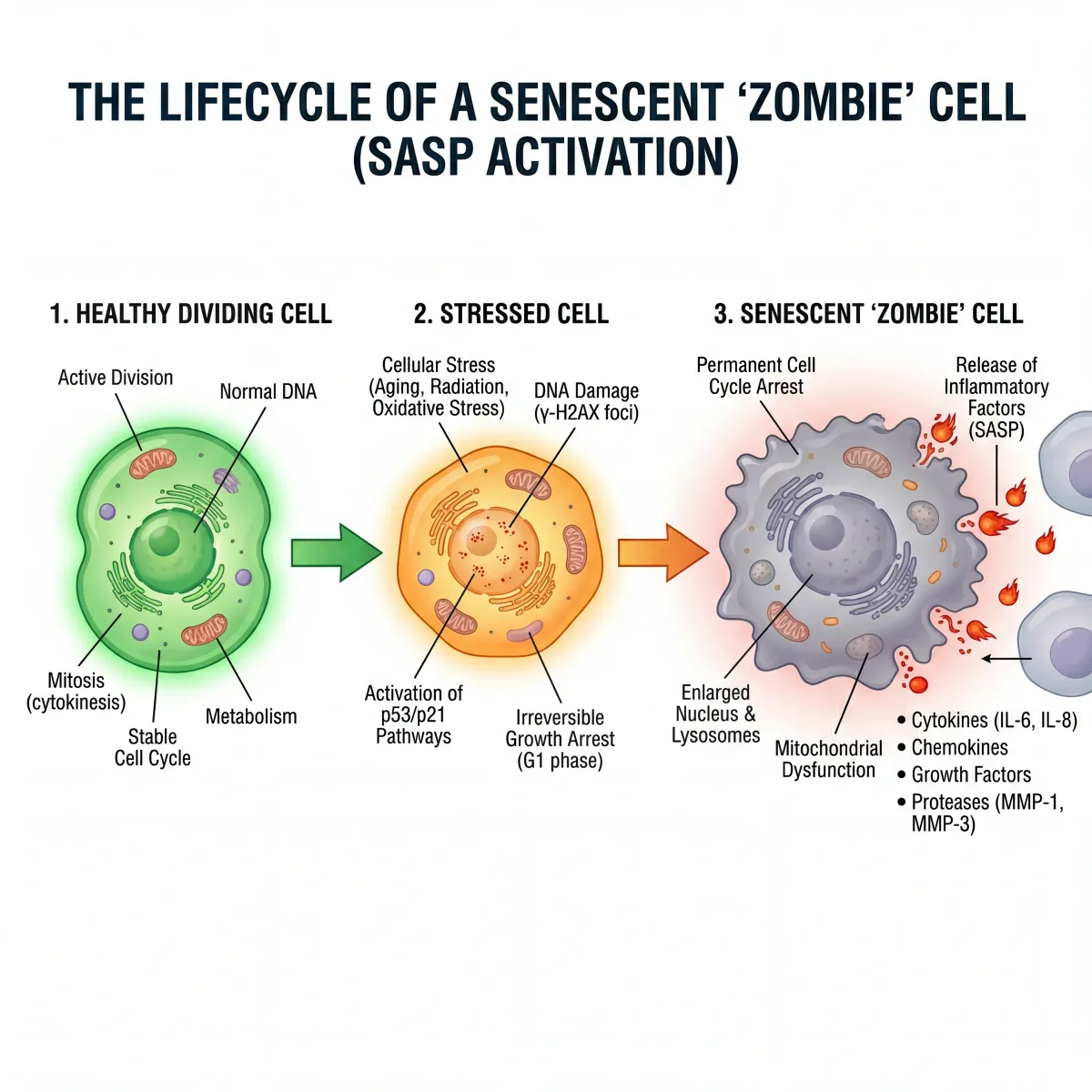
The damage comes from what senescent cells secrete. They pump out pro-inflammatory cytokines, chemokines, and tissue-degrading enzymes — a mix collectively called the senescence-associated secretory phenotype, or SASP. IL-6, TNF-alpha, MMP-3, and dozens of other factors damage surrounding healthy tissue and spread senescence to neighboring cells through paracrine signaling. One senescent cell can corrupt the cells around it.
Transplanting a small number of senescent cells into young mice is enough to cause physical dysfunction and accelerate aging. Multiple labs have replicated this result. The disease list is long: chronic inflammation, cardiovascular disease, type 2 diabetes, osteoporosis (2 million fractures and $19 billion in annual costs in the U.S. alone), osteoarthritis, pulmonary fibrosis, kidney disease, neurodegeneration.
| Feature | Normal Cell | Senescent "Zombie" Cell |
|---|---|---|
| Division | Active replication | Permanently arrested |
| Metabolic activity | Normal | Elevated |
| Apoptosis response | Functional | Resistant to programmed death |
| Immune clearance | Normal turnover | Evades NK cells via HLA-E and PD-L1 |
| Secretory profile | Standard signaling | SASP: pro-inflammatory cytokines, MMPs, chemokines |
| Effect on neighbors | Neutral | Spreads senescence through paracrine signaling |
How Senolytic Compounds Force Aging Cells Out
Senescent cells resist apoptosis for a specific reason: they upregulate pro-survival pathways that normal cells don't need. James Kirkland's team at Mayo Clinic mapped these pathways using expression profiling and RNA interference, identifying what they called Senescent Cell Anti-Apoptotic Pathways, or SCAPs. These include the BCL-2/BCL-XL family (which blocks mitochondrial apoptosis), PI3K/AKT signaling, p53/p21/serpine networks, and dependence receptor/tyrosine kinase pathways.
Senolytic drugs work by temporarily disabling these pro-survival defenses. Once the defenses drop, the cell's own SASP — which is constantly bombarding it with pro-apoptotic signals — finishes the job. The zombie cell self-destructs. Non-senescent cells, which don't depend on these upregulated pathways, remain unaffected at the same drug concentrations.
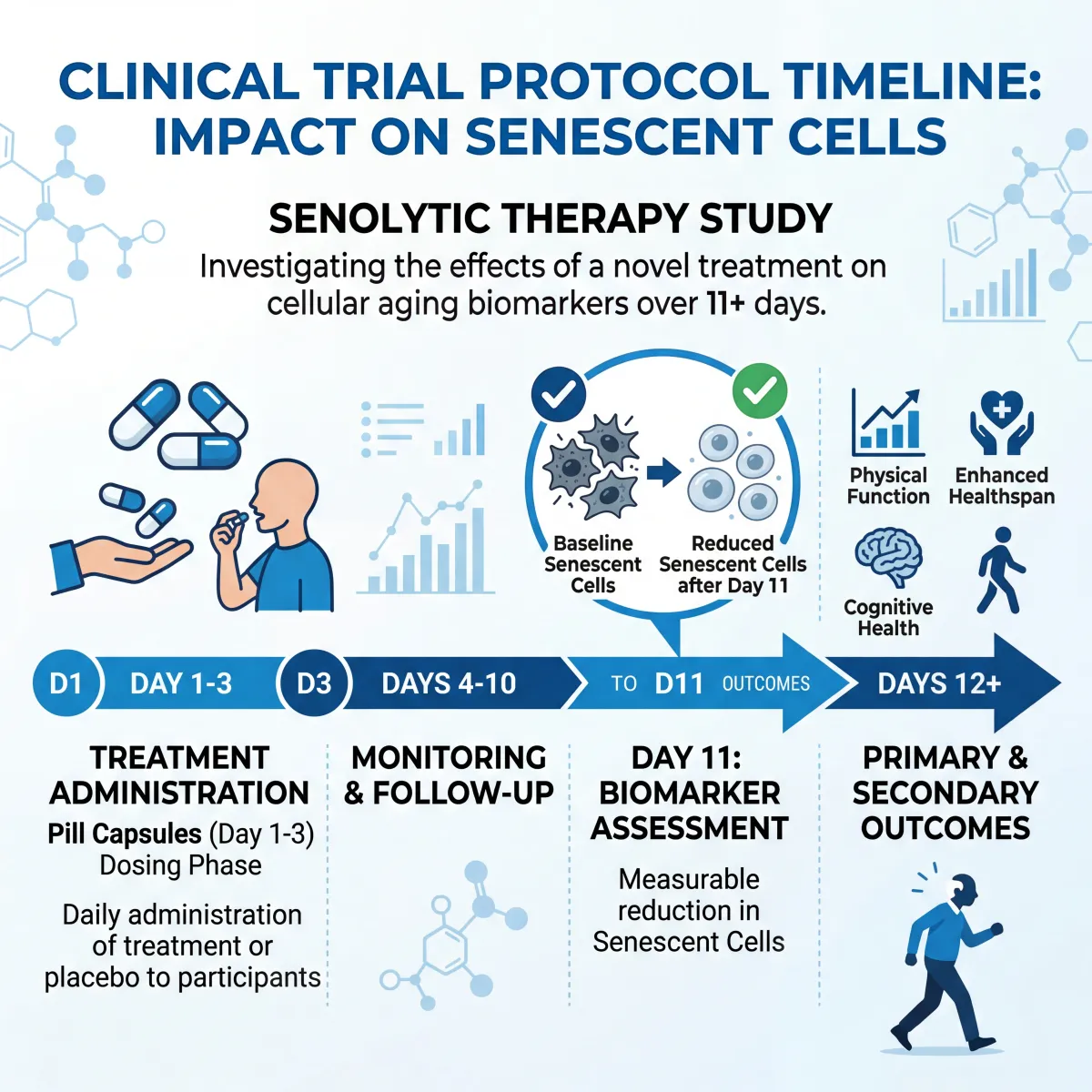
This is the "hit-and-run" mechanism that makes senolytics fundamentally different from conventional drugs. You don't need continuous dosing. A brief exposure — sometimes as short as three days — is enough to trigger apoptosis in senescent cells. The drugs clear the body within hours, but the senescent cells are already gone. In Mayo Clinic's first human trial, effects on senescent cell reduction persisted for at least 11 days after the drug combination had completely cleared participants' systems.
Different senolytic agents target different survival pathways, which means they work on different cell types. Dasatinib (a tyrosine kinase inhibitor originally developed for leukemia) kills senescent preadipocytes. Quercetin (a plant flavonoid) kills senescent endothelial cells. Combining them broadens the range. Fisetin, a related flavonoid, appears to hit multiple pathways simultaneously and shows the broadest activity profile of any single natural compound tested so far.
Fisetin: From Strawberry Pigment to Longevity Compound
Fisetin is a flavonoid polyphenol found in small amounts across many fruits and vegetables. The highest natural concentration occurs in strawberries at 160 micrograms per gram, with lower amounts in apples, persimmons, grapes, onions, and cucumbers. Average dietary intake from food alone is roughly 0.4 mg per day — orders of magnitude below the doses used in senolytic research.
In 2018, a landmark study tested 10 different flavonoid polyphenols for senolytic activity. Fisetin came out on top. When administered to old mice — beginning at the equivalent of roughly 75 human years — fisetin reduced senescence markers in multiple tissues, restored tissue homeostasis, reduced age-related pathology, and extended both median and maximum lifespan. That it worked even when started late in life — not just preventively — strengthened the case for human trials.
Fisetin's mechanism involves the PI3K/AKT and BCL-2 survival pathways. It selectively induces apoptosis in senescent human endothelial cells (HUVECs), confirmed by caspase-3/7 activation at concentrations as low as 0.5 micromolar. It does not kill senescent fibroblasts or preadipocytes at the same concentrations, which means fisetin — like all senolytics — is cell-type specific.
| Property | Fisetin | Quercetin |
|---|---|---|
| Chemical class | Flavonol (3,3',4',7-tetrahydroxyflavone) | Flavonol (3,3',4',5,7-pentahydroxyflavone) |
| Richest food source | Strawberries (160 μg/g) | Capers, red onions, kale |
| Senolytic target cells | Endothelial cells (HUVECs) | Endothelial cells (HUVECs) |
| Survival pathways targeted | PI3K/AKT, BCL-2 | PI3K/AKT, BCL-2, serpine |
| Mouse lifespan extension | Yes (median and maximum) | Yes (in combination with dasatinib) |
| Plasma half-life (mice) | ~3 hours | ~2 hours |
| Known drug interactions | May potentiate warfarin (glucuronidation) | Cytochrome P450 interactions |
Fisetin also has anti-inflammatory and neuroprotective activity outside of senolysis. It promotes apoptosis in breast cancer MCF-7 cells without affecting non-tumorigenic cells. Because it's hydrophobic, fisetin penetrates cell membranes and accumulates inside cells — which partly explains why it's potent despite a plasma half-life of only about three hours in mice.
The NIH funded a multicenter, placebo-controlled clinical trial (AFFIRM-LITE) testing fisetin in skilled nursing facility residents with COVID-19, based on the rationale that senescent cell burden increases COVID-19 severity because SASP factors overlap with the cytokine storm that drives critical illness. That trial reflects growing institutional confidence in fisetin's safety profile, even in frail elderly populations.
Quercetin and the Dasatinib Combination Protocol
Quercetin was among the first compounds identified as senolytic, discovered through Kirkland's hypothesis-driven screen of drugs targeting senescent cell anti-apoptotic pathways. Alone, quercetin kills senescent endothelial cells. Dasatinib, alone, kills senescent preadipocytes (fat cell progenitors). Combined, they cover a wider range of senescent cell types and in some cases act synergistically — meaning the combination is more effective than the sum of each drug alone.
The combination has been tested in animal models of idiopathic pulmonary fibrosis, where it improved lung function. In aged mice, it improved cardiac ejection fraction and vascular reactivity after a single three-day treatment course. It reduced osteoporosis, decreased frailty markers, preserved intervertebral disc integrity, and lowered liver steatosis in high-fat diet models.
A mouse study in Nature Communications tracked D+Q's effects on age-dependent intervertebral disc degeneration. Mice treated from age 6 or 14 months showed lower degeneration scores, reduced SASP markers (IL-6, MMP13), preserved extracellular matrix, and less cell death in the disc. But mice that started at 18 months — when degeneration was already established — saw no benefit. Timing matters, and starting earlier appears to be the difference between prevention and futility.
What Clinical Trials Actually Show
The first human trial of D+Q involved nine participants with diabetic kidney disease. Each received a combination dose of dasatinib and quercetin for three days. Analysis of blood, skin biopsies, and adipose tissue confirmed that senescent cells were reduced across multiple tissues, with effects persisting at least 11 days after the drugs cleared. The study was small and primarily assessed safety and feasibility, but it was the first direct evidence that senolytic drugs could reduce senescent cell burden in living humans.
Subsequent trials have expanded into other conditions. In patients with idiopathic pulmonary fibrosis, nine doses of oral D+Q over three weeks improved six-minute walk distance, walking speed, and chair-rise ability. The STAMINA trial tested D+Q in older adults with mild cognitive impairment and found the protocol was safe and feasible, with 99% medication compliance and no serious adverse events related to the study drugs.
An epigenetic study complicates the picture. Nineteen participants took D+Q for six months, with DNA methylation measured at baseline, three months, and six months. First-generation epigenetic clocks showed an unexpected increase in age acceleration at three months, though this partially reversed by six months. Second and third-generation clocks (PhenoAge, GrimAge, DunedinPACE) showed no significant changes. When fisetin was added to the protocol in a follow-up study — 50 mg dasatinib, 500 mg quercetin, 500 mg fisetin — the epigenetic age acceleration seen with D+Q alone was no longer statistically significant, suggesting fisetin may buffer the epigenetic effects.
| Trial | Participants | Protocol | Key Finding |
|---|---|---|---|
| Hickson et al. (EBioMedicine, 2019) | 9 (diabetic kidney disease) | D+Q, 3-day course | First proof senescent cells reduced in human tissue |
| IPF pilot (Mayo Clinic) | 14 (pulmonary fibrosis) | D+Q, 9 doses over 3 weeks | Improved walk distance and physical performance |
| Lee et al. (Aging, 2024) | 19 (healthy volunteers) | DQ 6 months, then DQF 6 months | Adding fisetin mitigated epigenetic aging signals |
| STAMINA (Lancet EBioMedicine, 2025) | 12 (mild cognitive impairment) | D+Q, intermittent over ~14 weeks | Safe and feasible; 99% compliance; no serious AEs |
| AFFIRM-LITE (ongoing) | Nursing facility residents | Fisetin, placebo-controlled | Testing fisetin for COVID-19 outcomes |
Dosing, Timing, and Why Self-Prescribing Is Risky
Clinical trials have used specific dosing protocols that bear no resemblance to what's sold over the counter. The D+Q combination in human trials typically uses dasatinib at pharmaceutical-grade doses (a prescription leukemia drug) combined with quercetin. The epigenetic study used 50 mg dasatinib plus 500 mg quercetin, with 500 mg fisetin added in the second phase. These are intermittent protocols — a few days on, then weeks or months off — based on the hit-and-run principle that senescent cell death persists long after the drug clears.
What you'll find on supplement shelves is different. Over-the-counter senolytic supplements typically contain only quercetin and/or fisetin, since dasatinib is a prescription pharmaceutical. According to Nicolas Musi, Vice Chair of Translational Research at Cedars-Sinai, senolytic supplements are typically sold at much lower doses than needed to be effective. Since these supplements aren't regulated by the FDA, their ingredients, quality, and compound amounts can't be verified — especially products bought online.
James Kirkland, the researcher who discovered senolytics, has been unusually direct for a scientist: "People have to be very, very concerned about what they buy. Don't take advice over the internet and pay exorbitant prices for things that may or may not work." He advises most people to avoid senolytics "until and unless we have really rigorous, reproducible scientific data that pharmaceutical regulators and the medical community accept."

Fisetin is metabolized through glucuronidation, which means it could potentiate the effects of warfarin and other drugs metabolized through the same pathway. Research on D+Q's effects on vascular smooth muscle cell chromatin found that the combination affects both young and senescent cells — senescent cells showed some "rejuvenation" of chromatin structure, but young cells showed temporary senescence-like changes. Those changes reversed after 24 hours, but the finding underscores that senolytics are not surgically precise instruments.
Then there's immunity. Senescent cells include senescent T cells and NK cells. Eliminating them might improve primary immune responses in the short term, but researchers have raised concerns that immunological memory — the basis of vaccine protection and long-term immunity — could be negatively impacted by indiscriminate senescent cell clearance. Certain memory T cells share surface markers with senescent cells, and whether current senolytic compounds can distinguish between the two is an open question.
Senescent cells also serve beneficial roles in wound healing and tissue repair, and their SASP recruits immune cells to sites of injury. Eliminating too many at the wrong time could impair healing. Researchers have found extremely varied responses to how senolytic drugs are absorbed across different ethnic groups, adding another layer of unpredictability to self-dosing.
Frequently Asked Questions
Can eating strawberries and onions provide enough fisetin and quercetin to work as senolytics?
No. The average dietary intake of fisetin is approximately 0.4 mg per day. Senolytic research uses doses hundreds of times higher — 500 mg or more in clinical studies. Strawberries contain the highest natural fisetin concentration at 160 micrograms per gram, but you'd need to eat roughly 3 kilograms of strawberries daily to approach research doses. The same math applies to quercetin from onions and kale. Dietary flavonoids have other health benefits, but achieving senolytic-level tissue concentrations through food alone isn't feasible.
Are senolytic supplements safe to take without a doctor's guidance?
Researchers who developed these compounds recommend against it. Over-the-counter supplements aren't regulated by the FDA, so you can't verify their ingredients, purity, or dose accuracy. Senolytic supplements can interact with medications — fisetin may potentiate warfarin, and quercetin affects cytochrome P450 enzymes that metabolize many common drugs. Individual responses also vary significantly. Both Kirkland and Musi at Cedars-Sinai advise consulting a physician before taking any senolytic supplement.
How often should senolytics be taken based on the research?
Clinical protocols use intermittent dosing, not daily supplementation. The hit-and-run mechanism means senescent cells die even after the drug leaves the body. In human trials, D+Q has been given as short courses (2-3 consecutive days) separated by weeks or months. One animal study used weekly injections. This intermittent approach is deliberate — it reduces the opportunity for side effects while still clearing the senescent cell burden. Taking senolytics daily is not supported by the current research and may increase risk without additional benefit.
What is the difference between senolytic and senomorphic approaches?
Senolytics kill senescent cells outright by disabling their anti-apoptotic defenses. Senomorphics suppress the harmful effects of senescent cells — particularly the SASP — without destroying them. A JAK1/2 inhibitor, for example, can block SASP production and reduce local inflammation without triggering cell death. Both approaches have shown benefits in animal models of age-related disease. The advantage of senomorphics is that they preserve any beneficial functions of senescent cells (like tumor suppression); the disadvantage is that they require continuous dosing since the cells remain alive.
Are there natural ways to reduce senescent cell accumulation besides supplements?
Exercise is the strongest non-pharmacological intervention. Physical activity enhances immune surveillance — particularly NK cell and macrophage function — which helps the body clear senescent cells naturally. Caloric restriction and intermittent fasting activate autophagy pathways that may reduce senescent cell burden. Some approved medications like metformin also appear to have geroprotective effects. Nicolas Musi at Cedars-Sinai recommends exercise as the most accessible longevity intervention while clinical trial data on senolytics matures.
Related Articles
- Autophagy: How to Trigger It Through Fasting, Exercise, and Diet — Autophagy and senescence clearance are complementary cellular maintenance systems that decline with age.
- Telomere Length: Can You Actually Slow Cellular Aging? — Telomere shortening is one of the primary triggers of cellular senescence.
- Biological Age Testing: How to Measure and Improve Your Pace of Aging — Epigenetic clocks are now being used to measure whether senolytic interventions actually reverse biological aging.
- Spermidine: The Longevity Compound in Wheat Germ That Triggers Autophagy — Another natural compound being studied for its anti-aging properties through different mechanisms.
- Chronic Inflammation and Anti-Inflammatory Living — The SASP from senescent cells is a major driver of the chronic low-grade inflammation linked to aging.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











