
The first time you notice it is around 42. The alarm goes off, the room is quiet, your body is technically rested, and the first hour still feels like wading through cold porridge. Coffee helps. The shower helps. By 10 a.m. you're functional. But the version of you that used to roll out of bed already moving forward has gone somewhere, and no amount of supplements seems to call him back.
That somewhere has a name. Endocrinologists call it the somatopause. Sermorelin, a peptide that mimics the body's own growth-hormone-releasing hormone, is one of the most researched tools for nudging that biology back. This guide is for men over 40 who care less about the bodybuilding angle and more about morning energy and deep sleep — and want to know what the evidence actually says before filling a prescription.
Why Men 40+ Lose Morning Energy
Growth hormone is not a bodybuilding hormone — that marketing reframe is why most men dismiss it. In actual physiology, GH and the IGF-1 it triggers in the liver are the night-shift maintenance crew that repairs muscle, recycles damaged cells, regulates fat metabolism, and keeps mitochondria producing ATP at a young-adult clip. When that crew shows up half-staffed, the visible damage is slow: a little more belly, a little less recovery, more cold porridge before 10 a.m.
The slow part is the problem. A 2013 review in Best Practice & Research Clinical Endocrinology & Metabolism reports GH production declines roughly 14% per decade after early adulthood. A pubertal boy produces 1.0 to 1.5 mg of GH per day; an elderly man may produce as little as 50 micrograms. By 40, clinicians estimate 30 to 40 percent of peak output is gone; by 60, production lands at 15 to 25 percent of youthful levels.
The same review found that in men 60 and older, 35 percent meet clinical criteria for GH deficiency, and 85 percent of healthy men aged 59 to 98 carry IGF-1 levels below the 2.5th percentile of younger men. That is most of the room at any over-60 cardiology appointment.
Somatopause does not arrive alone. Testosterone declines at 1 to 2 percent per year after age 30. The two declines reinforce each other: GH supports Leydig-cell function and lowers sex-hormone-binding globulin, while testosterone makes the pituitary more responsive to GH-releasing signals. When both fall together, the symptom cluster — fatigue, abdominal fat that ignores diet, slower recovery, mental fog, irritability — gets filed as lifestyle. Lifestyle is part of it. The hormonal floor is doing more work than men realize.
The intervention isn't broken; the substrate it was designed for has changed.
How Sermorelin Restores GH Pulsatility
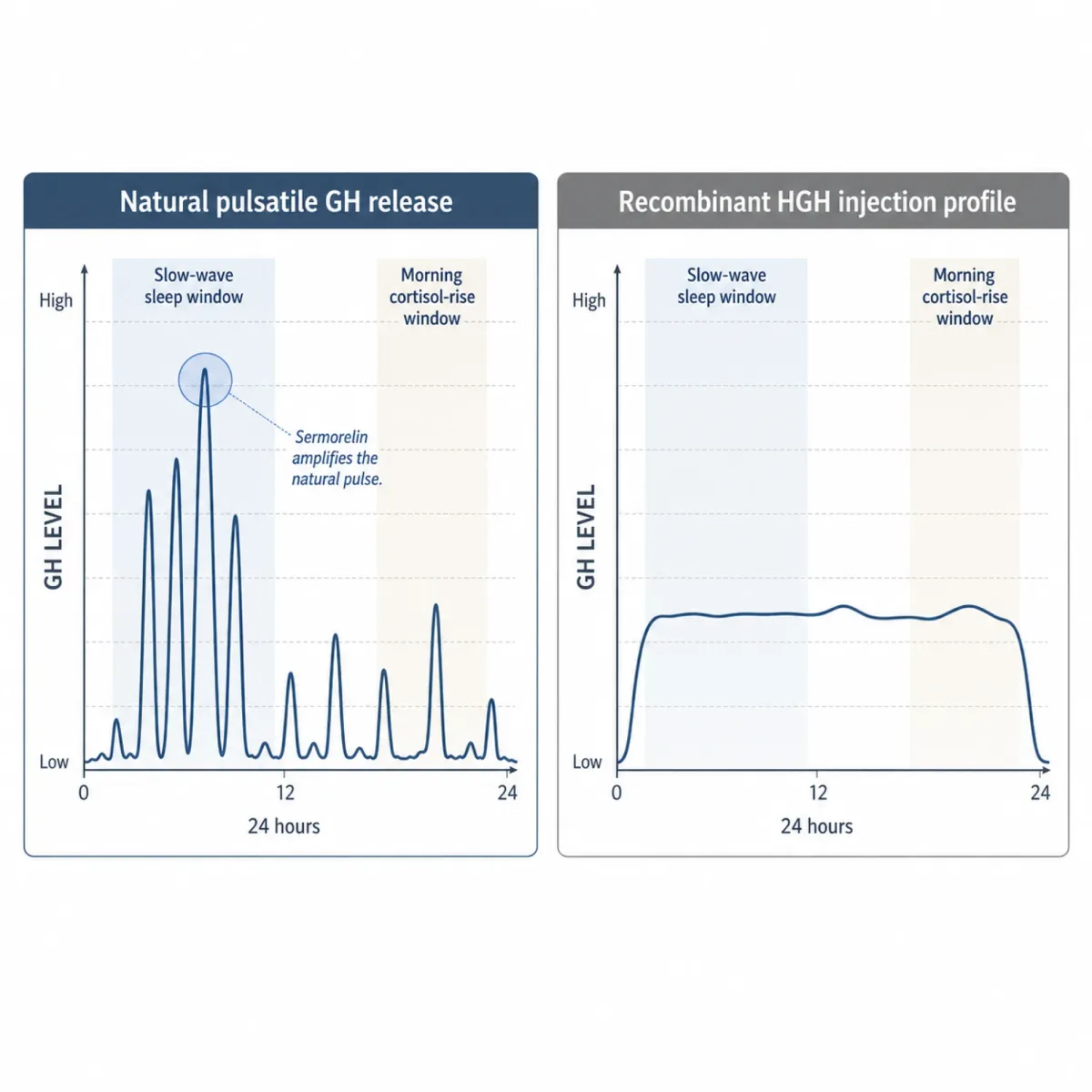
Picture the pituitary as a thermostat rather than a faucet. The hypothalamus releases GHRH in pulses, mostly at night; the somatotroph cells fire a burst of stored GH; somatostatin from the same brain neighborhood then calls everything back down. The system is built for episodes of high signal followed by quiet, not continuous infusion.
Sermorelin is a synthetic peptide containing the first 29 amino acids of natural human GHRH — the bioactive sequence the receptor actually reads. Injected subcutaneously, it binds GHRH receptors on somatotroph cells and triggers the same cAMP-PKA cascade that drives calcium influx and GH vesicle release. The pituitary does what it normally does, with a stronger upstream nudge.
The pulsatile pattern is not cosmetic. A 2025 clinical review in Frontiers in Aging traces how GH signaling through JAK-STAT behaves differently when receptors see pulses versus continuous exposure. Pulses favor lipolysis, lean-tissue anabolism, and intact insulin sensitivity. Continuous elevation — what follows a recombinant HGH injection — pushes the system toward insulin resistance, fluid retention, and joint discomfort. The 2013 ScienceDirect review describes GHRH agonists as restoring “normal GH pulsatility and amplitude”, the structural reason this class is positioned as the gentler tool.
The other quiet feature: the body's own brake stays attached. As GH and IGF-1 rise, somatostatin secretion increases and dampens further pituitary release. Direct rhGH bypasses the brake; sermorelin doesn't. For a 47-year-old looking at multi-year therapy, that built-in ceiling is worth more than the early scale-weight numbers.
For a deeper comparison, see our earlier piece on sermorelin vs. HGH injections for anti-aging. Same destination on the GH axis, very different on-ramps.
Morning Energy and Deep Sleep
If a man on sermorelin notices anything in the first month, it will almost always be sleep. That isn't marketing — it's a consequence of where the day's largest GH pulse fires.
A landmark review by Eve Van Cauter and colleagues at the University of Chicago, published in the Journal of Clinical Endocrinology & Metabolism, established that approximately 70 percent of daily GH secretion in men occurs during sleep, with the most significant pulse arriving within minutes of the first slow-wave-sleep episode. The amount of GH released correlates directly with time in deep, stage-3 NREM sleep. As that depth erodes with age, the nightly hormone bath shrinks with it.
The relationship is bidirectional. Ferenc Obal and James Krueger, in Sleep Medicine Reviews (2004), demonstrated that GHRH itself is sleep-promoting — it activates sleep-regulatory neurons in the preoptic hypothalamus and increases NREM duration and slow-wave activity independent of its GH-releasing role. GHRH helps you fall into deep sleep; deep sleep triggers GH; the GH supports cellular repair. When GHRH activity drops with age, both ends of the loop suffer at once.
Two studies nailed the timing question. Steiger and colleagues found that pulsatile GHRH given in the first half of the night significantly increased both GH and slow-wave sleep in healthy young men, while the same compound in the early morning produced no sleep effect because cortisol-driven wakefulness overrides it. Marshall and colleagues, in a 1996 comparison of episodic versus continuous GHRH infusion, showed pulsatile dosing produced significantly greater stage-4 slow-wave sleep than continuous infusion. A bedtime sermorelin injection looks structurally a lot like the natural GHRH pulse the body is trying to generate.
The morning-energy effect comes from the same physiology. GH drives mitochondrial biogenesis, glucose metabolism, and fatty-acid oxidation — the machinery of cellular ATP. When GH falls, cells get less efficient at converting nutrients into usable energy, the substrate behind what men describe as “the battery no longer fully charges.” When deeper sleep returns, mitochondria do their overnight repair properly, and the next morning is the first place that shows. Most patients report this within the first one to two weeks.
If sleep doesn't change by week three, the dose, the timing, or the pituitary's responsiveness deserves a second look before continuing.

Nightly Dosing and Why Timing Matters
Sermorelin is a once-daily subcutaneous injection. The mundane version of that fact misses what matters: when you inject controls most of the result.
Standard adult dosing, per 503B compounding-pharmacy literature from Empower, is 0.2 to 0.3 mg of sermorelin acetate subcutaneously once daily at bedtime. Most clinicians working with men 40+ start at 200 to 300 micrograms nightly and titrate up after four to six weeks based on IGF-1 labs. The IGF-1 target is upper-normal — roughly 200 to 300 ng/mL, the range of a healthy man in his late twenties.
Three details determine whether the injection actually does its job.
Timing. Inject 30 to 60 minutes before sleep, synchronized to where the body's first slow-wave-sleep episode would naturally start. Inject at 9 p.m. if you reliably fall asleep at 10. Move that window earlier and you miss the first SWS pulse you're trying to amplify; push it past sleep onset and the pharmacokinetic peak fires when you're already in lighter sleep.
Empty stomach. No food for two to three hours before. Elevated glucose and the insulin response that follows it directly suppress the pituitary's GH response to GHRH. Eat pasta at 9, inject at 10, and you've spent a real prescription on a blunted pulse.
Site. Subcutaneous fatty tissue — abdomen, outer thigh, or back of the upper arm — rotated nightly. Healthline's clinical writeup describes the standard technique: pinch a fold, insert at 90 degrees with a 29- or 30-gauge insulin syringe, depress slowly, withdraw straight.
Long-term protocols typically introduce cycling after the first three to six months — five days on/two off, four weeks on/one off, or three months on/one off — to prevent GHRH-receptor desensitization. Whether cycling is necessary or merely cautious is genuinely unresolved; clinicians don't all agree.
The 3 to 6 Month Timeline
Set expectations in months, not weeks. Failure modes show up as the timeline staying flat past an expected milestone. Compiled from clinic-reported observations of men over 40:
| Timeframe | What men typically notice | Underlying physiology |
|---|---|---|
| Weeks 1 to 4 | Improved sleep depth, more morning energy, less post-workout soreness | Nocturnal GH pulsatility normalizes; SWS time increases; mitochondria recover |
| Weeks 4 to 8 | Measurable strength gains, early waist-circumference reduction, faster recovery | IGF-1 reaches young-adult range; mTOR signaling restores muscle protein synthesis |
| Weeks 8 to 16 | Visible reduction in abdominal fat, body-comp testing shows 3 to 5% fat loss | Hormone-sensitive lipase mobilizes visceral fat; insulin sensitivity improves |
| Months 4 to 6 | Total fat loss of 4 to 8%, lean muscle gains of 3 to 6 lb | Full GH-axis optimization; cardiovascular and lipid markers begin shifting |
| Months 6 to 12 | Stabilization at a new baseline, sustained energy, gradual continued improvement | Long-term tissue remodeling; cycling protocol typically introduced |
Those numbers come from aggregated patient reports from sermorelin telehealth practices, not randomized trials. Independent confirmation that the magnitudes are reasonable comes from the 2013 ScienceDirect review, which found that controlled studies of GH supplementation in older men show roughly 2 kg lean-mass gain with similar reduction in fat mass.
One useful proof-of-concept anchor: a 1996 Thorner study cited by Healthline reported daily sermorelin injections increased growth rate in 74 percent of children with GH deficiency after six months. That was a pediatric trial — but it established that GHRH(1-29) reliably stimulates the pituitary GH axis. The men's-health applications are downstream of that biology.
The honest disclosure: randomized trials of sermorelin in healthy men over 40, with energy and sleep as primary endpoints, do not exist at the scale that exists for GLP-1 drugs. Eric Topol has been pointed about this: there are no large randomized human trials demonstrating sermorelin's anti-aging benefits. What exists is consistent clinic-level observation tied to defensible mechanism — a different category of evidence from a Phase III.
Safety, Side Effects, and Regulatory Status
The most common side effects are exactly what you would predict for a subcutaneous peptide. Healthline and aggregated practice data agree on the short list: injection-site reactions in roughly 15 to 20 percent of users, brief facial flushing for 5 to 15 minutes after injection, mild headaches in the first one to two weeks, and transient fluid retention or joint stiffness as GH levels rise. Most resolve as the body adjusts. Serious adverse events are rare, in part because the somatostatin brake prevents the supraphysiological GH spikes that direct rhGH injection can produce.
The regulatory picture is more interesting. Sermorelin was originally FDA-approved in 1997 under the brand name Geref for pediatric growth-hormone deficiency. The manufacturer Serono ceased commercial production around 2006, and the FDA officially listed sermorelin as discontinued in 2008. The agency was unusually explicit: the discontinuation was a business decision, not withdrawal for safety or effectiveness reasons.
Today, sermorelin is available only through FDA-registered compounding pharmacies operating under Section 503A or 503B authority. Frier Levitt's 2025 regulatory analysis notes that sermorelin is one of the few peptides allowed in this channel because it appears in Category I of the FDA interim 503A Bulks List, alongside NAD+. Most other GH-axis peptides — CJC-1295, ipamorelin, BPC-157, AOD-9604 — do not meet that criterion and exist in legal grey territory marketed as “research chemicals.” Sermorelin is genuinely different here.
Compounded does not mean equivalent to FDA-approved. Compounded drugs are not FDA-approved as products; the agency does not test individual batches. The real-world consequence shows up in recall notices like Olympia Pharmacy's nationwide recall of seven compounded products including sermorelin, after lots were found out-of-specification. The FDA has separately placed related compounds, including growth hormone releasing peptide-2 (GHRP-2), in Category 2 over immunogenicity concerns. Sermorelin's identical-to-natural-GHRH sequence is the structural reason it has not landed there.
Three more things worth surfacing. Sermorelin is on the World Anti-Doping Agency prohibited list — if you compete in a sanctioned sport, hard stop. There are no large randomized trials on long-term cancer risk in healthy adults; the theoretical concern with any GH-axis intervention is that elevated IGF-1 can support proliferation of tumor cells if a clinically silent malignancy is already present. And men with active malignancy, uncontrolled diabetes, untreated retinopathy, or untreated hypothyroidism are typically excluded until those conditions are managed.
Who Should Skip Sermorelin
Some men should not take sermorelin. Some should not take it yet. The categories are different.
The not-at-all list is short and absolute: active or recently treated malignancy, untreated severe sleep apnea, active diabetic retinopathy, uncontrolled type 2 diabetes, untreated hypothyroidism. Anyone competing in a tested sport is also a hard stop because of the WADA listing.
The not-yet list is longer. If a man over 40 is sleeping six hours a night, sedentary, drinking five nights a week, and 25 pounds heavier than he was at 30, sermorelin will help around the edges but won't move the needle the way the marketing implies. GH secretion responds powerfully to inputs men have neglected. Resistance training at 70 to 85 percent of one-rep max produces an endogenous GH spike. High-intensity intervals of 20 to 30 seconds at maximum effort do too. Overnight fasting of 12 to 16 hours pushes the pituitary toward larger nighttime pulses by lowering the insulin signal that competes with GHRH. Consistent 7 to 9 hours of sleep with a cool dark room compounds all of it. A man who has not yet bought himself those gains has cheaper room to grow before he reaches for a prescription.
For men who do start, monitoring is consistent across clinical sources: IGF-1 every three to six months, fasting glucose and insulin, comprehensive metabolic panel, lipid panel, complete blood count (especially with concurrent TRT), and PSA. A DEXA scan or bioimpedance reading at baseline and every six to twelve months gives you the body-composition trend.
One last note. Roughly 40 percent of men experience some degree of erectile dysfunction by age 40, rising to about 70 percent by 70. Sermorelin is not an ED drug. Improvements men report come downstream of better sleep, lower visceral fat, and improved endothelial function — not direct sexual pharmacology. If sexual function is the primary complaint, that conversation belongs with a urologist before a sermorelin intake form.
Frequently Asked Questions
How fast will I feel different on sermorelin?
Most men over 40 notice improved sleep depth and morning energy within the first one to two weeks. Strength and recovery changes typically arrive between weeks four and eight; visible body-composition change emerges from weeks eight to sixteen. If three weeks pass with no sleep change, that's a signal to revisit dose, timing, or the empty-stomach rule before continuing.
Can sermorelin replace testosterone replacement therapy?
No. Sermorelin works on the growth-hormone axis and TRT works on the androgen axis. In men with borderline-low testosterone, sermorelin's improvement in deep sleep and reduction in visceral fat can nudge endogenous testosterone modestly upward, but that is not a substitute for actual TRT in clinically deficient men. Men needing both typically run them together with appropriate monitoring.
Why does the timing of the injection matter so much?
The pituitary's response to GHRH is gated by the cortisol-driven wakefulness signal that runs the morning, and by the insulin response to anything you've eaten in the prior two to three hours. A bedtime injection on an empty stomach lands the GHRH pulse in the same window when the pituitary is most responsive and lifestyle inhibitors are at their lowest. An injection three hours late, after a carb-heavy dinner, can produce a measurably blunted GH pulse despite the same dose.
Is the compounded supply trustworthy?
It depends on the pharmacy. The FDA does not verify potency, sterility, or purity of compounded products on a per-batch basis, and recalls do happen — Olympia Pharmacy issued a nationwide recall of out-of-specification compounded sermorelin in a recent example. Working with a reputable 503B outsourcing facility or an established 503A pharmacy that publishes its USP 797/795 compliance reduces, though does not eliminate, the channel-specific risk.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











