
The Stack Everyone Talks About Is Not Really Public
Search for Bryan Johnson and peptides, and the internet quickly starts behaving as if there is a secret injectable recipe sitting behind the Blueprint logo. BPC-157, TB-500, GHK-Cu, Epitalon, growth-hormone secretagogues: the names travel together in biohacking threads until they sound like one tidy protocol.
The public evidence is much narrower. In the public Blueprint material reviewed for this guide, the clearly disclosed peptide-related items are oral collagen peptides, topical hair and scalp peptides, Follistatin gene therapy, and a Cerebrolysin trial, not a published consumer stack of BPC-157, TB-500, or Epitalon injections. That distinction matters because copying a public diet habit is one thing; guessing at a private drug protocol is another.
Bryan Johnson's most copyable peptide lesson is not "buy the stack." It is "separate documented protocol from online fan fiction before spending money."
Blueprint's public skin guidance says to consume 20 to 30 grams of collagen peptides daily and pair them with vitamin C. Its public hair section describes a water-based peptide serum and shampoo, with the serum containing eight biomimetic peptides: EGF, Thymosin-beta4, SCF, hGH, VEGF, PDGF, Follistatin, and Copper Tripeptide-1. Those are real disclosures, but they are mostly topical or nutritional.
The advanced interventions are also not normal shopping-list items. Johnson's protocol says he received Follistatin gene therapy in October 2023. The same page says he trialed daily 5 mL intramuscular Cerebrolysin injections for three months and measured no effect. That last detail should slow everyone down. Even an extreme testing program can try something expensive and fail to find a useful biomarker signal.
| Claim People Make Online | What the Public Sources Actually Show | Budget Takeaway |
|---|---|---|
| Bryan has a clear injectable peptide stack. | Public Blueprint material shows collagen, topical hair peptides, and a few advanced therapies. | Do not buy injectables based on association. |
| More peptides means a better longevity protocol. | One disclosed Cerebrolysin trial found no measured effect. | Measurement beats novelty. |
| The normal-budget version is a cheaper gray-market vial. | Independent safety and anti-doping sources warn that the gray market is risky. | Cheap can be the expensive mistake. |
What Blueprint Actually Discloses
The most concrete "peptide stack" in the public Blueprint ecosystem is ordinary-looking compared with the injectable lore. The collagen product page lists a 30-day supply at $45, or $42.75 on subscription. The supplement facts list 20 g of collagen peptides Types I and III from bovine hide per serving, plus standardized chicken cartilage with 10 mg active Type II collagen.
That does not make it magic. Collagen peptides are more like building-material shipments than architectural blueprints. They may supply amino-acid fragments and bioactive peptides, but they still depend on the body's repair priorities, training stimulus, total protein intake, sleep, and time.
The haircare product is a different category. Blueprint's haircare stack page lists a one-time purchase price of $178, or $169.10 by subscription, and describes 11 advanced peptides including sh-polypeptide-86 and copper tripeptide-1. That is topical cosmetic territory, not the same risk category as injecting research-use compounds from a vial.
For readers trying to decode the protocol, the useful distinction is route. Oral collagen is food-adjacent. Topical peptides are cosmetic-adjacent. Gene therapy and injected neurotrophic mixtures are clinic-supervised experimental territory. Internet peptide stacks often collapse those categories into one word, "peptides," which is like calling a vitamin gummy, a prescription injection, and a lab reagent the same thing because they all fit in a drawer.
| Public Blueprint Item | Route | Published Price or Dose | How to Think About It |
|---|---|---|---|
| Collagen peptides | Oral | 20 to 30 g daily in the protocol; product serving lists 20 g | Potentially copyable if it fits diet and budget. |
| Hair peptide serum and shampoo | Topical | $178 one-time haircare stack | Cosmetic category, not comparable to injections. |
| Follistatin gene therapy | Medical intervention | Public protocol notes October 2023 | Not a normal-budget consumer protocol. |
| Cerebrolysin trial | Intramuscular injection | 5 mL daily for three months | Publicly reported as no measured effect. |
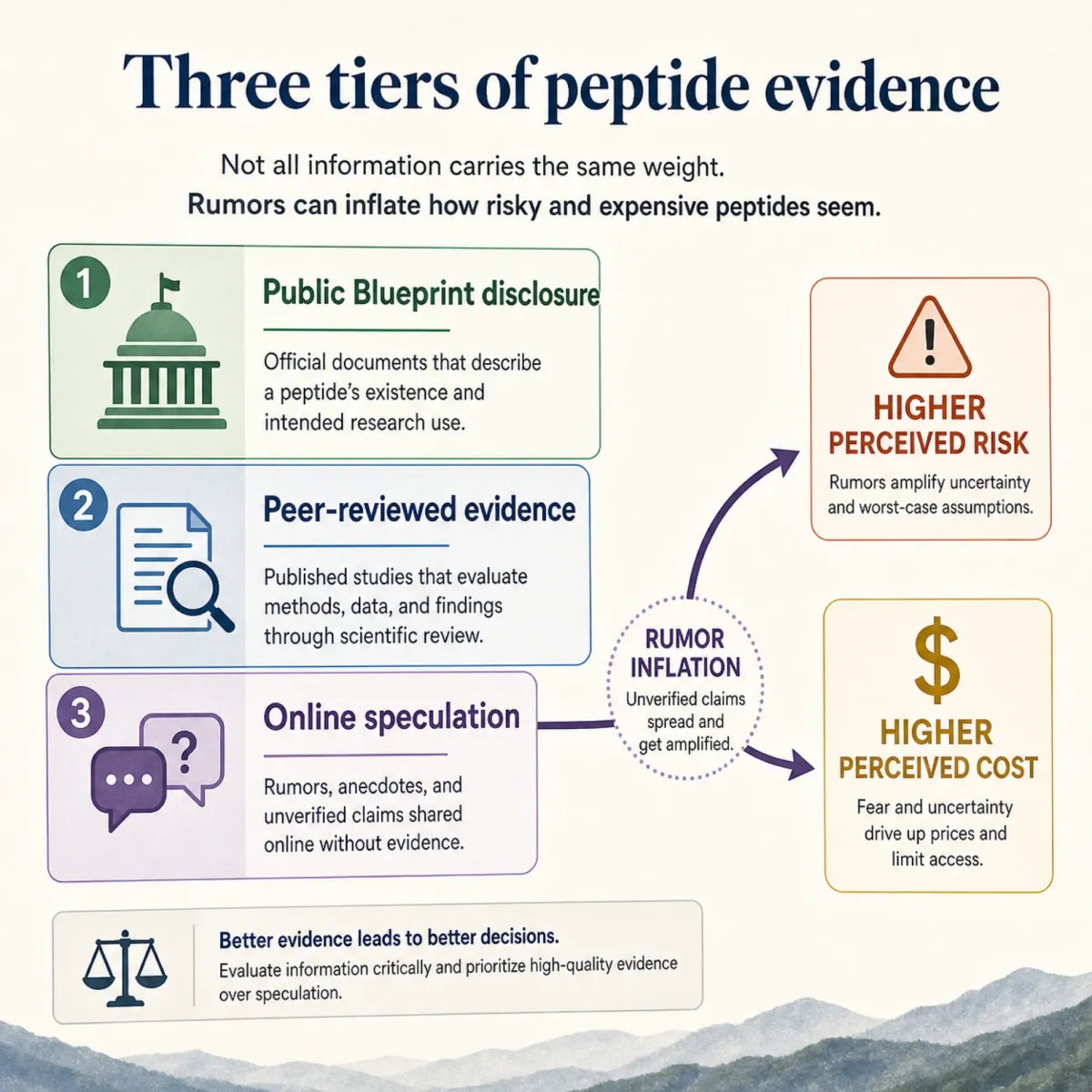
Why Peptide Rumors Stick to Longevity Influencers
Peptide rumors stick because the word sounds scientific, compact, and futuristic. Jonathan Jarry at McGill University's Office for Science and Society writes that the online peptide boom is confusing by design: some peptides are injected, some are oral, some influence growth hormone, and some do not. He describes the fad as a market where experimental drugs are promoted by fitness influencers even when the evidence and legal status are muddy.
The strongest skeptical point is not that every peptide is useless. Insulin and oxytocin are peptides, and medicine uses peptide drugs. The problem is the jump from "peptides exist in biology" to "a research vial from the internet will repair my tendon, reverse aging, and burn fat." McGill notes that many of the trendy compounds were studied mainly in rodents, small volunteer groups, or surrogate biomarkers rather than hard outcomes like improved strength or weight loss.
The same McGill review identifies BPC-157 plus TB-500 as the internet-nicknamed Wolverine Stack. That nickname does a lot of marketing work. It turns uncertainty into a superhero story. But a nickname is not a clinical endpoint.
There are also regulatory and sport consequences. McGill reports FDA concerns that compounds such as BPC-157, GHK, GHRP-6, and ipamorelin in compounded medication may pose immune-reaction risks. WADA's prohibited list places BPC-157 under S0 non-approved substances prohibited at all times. If you compete in tested sport, "I bought it for recovery" is not a loophole.
The practical implication is blunt: if a claim depends on the sentence "Bryan Johnson probably uses this," treat it as unsupported until a public source says so. The lower the evidence, the higher the burden should be before you inject anything.
The Budget Reality Check
For a normal budget, the most defensible peptide conversation starts with collagen because it has human data and does not require needles. In a double-blind, placebo-controlled trial, E. Proksch and colleagues randomized 69 women aged 35 to 55 to 2.5 g or 5.0 g of collagen hydrolysate or placebo once daily for 8 weeks. At the end of the study, the collagen groups showed statistically significant improvement in skin elasticity compared with placebo.
That result is interesting, but it does not prove that everyone needs the same dose Bryan Johnson uses. Blueprint's public protocol talks about 20 to 30 g daily, while the Proksch skin-elasticity trial used 2.5 g and 5.0 g daily. Those are different products, outcomes, and contexts. Think of the collagen literature like a dimmer switch, not a scoreboard: more grams are not automatically more benefit for every person.
A joint-health review in PMC adds another layer: native and hydrolyzed collagen are the most studied collagen types for joint health, and hydrolyzed collagen may contain bioactive peptides that reach joint tissues and exert chondroprotective effects. That is a reasonable basis for curiosity, not a license to ignore boring fundamentals.
The budget math is simple. A $45 collagen tub is a decision many households can at least evaluate. A $178 haircare stack is a cosmetic splurge. A self-directed injectable protocol from an unregulated seller is not a budget hack; it is a quality-control gamble with health consequences.
There is also a softer cost that biohacking forums rarely price: attention. A person who buys several experimental peptides at once loses the ability to know what helped, what did nothing, and what caused side effects. That is the opposite of the Blueprint spirit. Johnson's public Cerebrolysin note is valuable precisely because it admits an unglamorous result: a carefully tracked intervention produced no measured effect. For mortals, that is the pattern worth copying. Change fewer variables, define the outcome first, and be willing to stop when the signal is not there.
A conservative collagen trial, for example, can be framed around a practical goal such as protein convenience, skin dryness, nail brittleness, or joint comfort. It should not be framed as "Bryan takes this, so it must be the longevity lever." The evidence for collagen is strongest when you keep the claim modest. The Proksch trial measured skin physiology, and the joint review discusses collagen forms and mechanisms. Neither paper proves that a normal-budget person should spend their rent money trying to mimic a celebrity protocol.
What Is Worth Copying on a Normal Budget
The best part of Blueprint for ordinary people is not the expensive edge. It is the insistence on measurement, consistency, and basics before theatrics. A normal-budget version should feel almost disappointing: train, sleep, eat enough protein, correct obvious deficiencies with a clinician, and use supplements only when they solve a defined problem.
Strength training deserves first place because it attacks the same aging anxieties that peptide marketing exploits. The National Institute on Aging says NIA-supported researchers have studied strength training for more than 40 years and identified benefits including maintaining muscle mass, improving mobility, and increasing healthy years of life. NIA also notes that age-related muscle loss and strength decline, called sarcopenia, can be substantially slowed by maintaining an active lifestyle.
Vitamin D is another example of a boring metric that beats a dramatic purchase. NIH's Office of Dietary Supplements says serum 25(OH)D is the main indicator of vitamin D status, and 50 nmol/L, or 20 ng/mL, is sufficient for most people. That is not a peptide claim; it is a reminder to test what can be tested before chasing what cannot.
Omega-3s fit the same pattern. NIH ODS says EPA and DHA are present in fish, fish oils, and krill oils, while ALA is found in plant oils such as flaxseed, soybean, and canola. If your diet already handles this, great. If not, you can address it without pretending to run a private longevity lab.
This is where a normal-budget plan becomes more honest than the glamorous one. You do not need a shelf full of compounds to learn whether your baseline habits are weak. If training is irregular, recovery is poor, protein is low, or sleep is chaotic, the next peptide will mostly decorate the problem. The body is not a dashboard where every warning light needs a separate supplement. It is more like a house with a few overloaded circuits: fix the wiring before buying specialty bulbs.
That does not mean supplements are useless. It means they should be recruited for a job. Collagen can be a protein-adjacent convenience. Vitamin D can be a lab-guided correction. Omega-3 intake can be a diet-quality decision. A topical hair product can be a cosmetic experiment. Each one should have a reason to exist before it has a subscription.
| Priority | Budget Move | Why It Beats Peptide FOMO |
|---|---|---|
| First | Progressive strength training | Targets muscle, mobility, and aging resilience directly. |
| Second | Protein and collagen only if diet goals support it | Low drama, measurable intake, no needles. |
| Third | Lab-guided vitamin D or omega-3 decisions | Corrects a real gap instead of buying an identity. |
| Last | Prescription peptides only for a specific medical reason | Requires clinician oversight, not influencer certainty. |

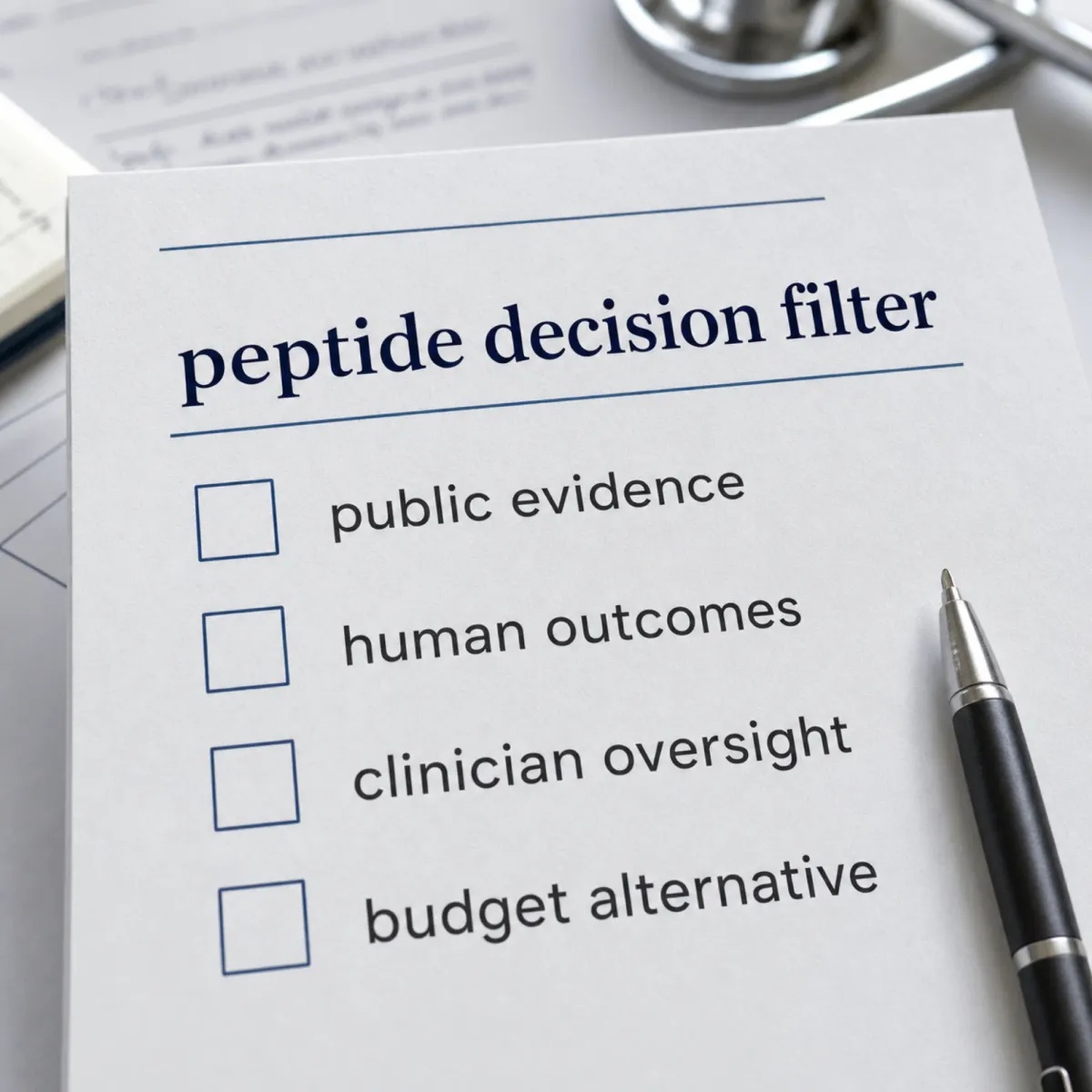
A Safer Decision Filter Before You Buy Anything
If you still want to evaluate a peptide, use a filter that removes glamour. First, ask whether the claim is publicly documented or merely attached to a famous person's name. Second, ask whether the human evidence measures an outcome you actually care about. Third, ask whether the product route changes the risk. A topical cosmetic peptide, oral collagen, and injected research-use peptide do not belong in the same mental bucket.
Then ask the budget question honestly: what would have to be true for this to beat the cheaper alternative? For collagen, that might mean clearer skin or easier joint comfort after a defined trial period. For a topical hair product, it might mean fewer broken strands or better scalp tolerance. For a gray-market injectable vial, the answer should usually be "nothing," because the quality-control and medical-risk problems are larger than the promised savings.
One useful rule is to downgrade any claim by one full notch when the evidence comes from a seller, an affiliate review, a private clinic page, or a forum thread. A seller can still be accurate, but the incentive is different. A clinic can still be careful, but it is not the same thing as an independent trial. A forum can surface real experiences, but it cannot test purity, diagnose a condition, or separate placebo from recovery that would have happened anyway.
Another rule is to separate "can be biologically active" from "should be bought by you." Many peptide discussions blur that line. A compound can do something in a cell dish, in a rodent model, or under specialist supervision and still be a poor choice for a healthy person with no diagnosis. Budget advice gets safer when it stops asking, "Could this work somehow?" and starts asking, "Is this the next best dollar for my actual risk profile?"
McGill's review is useful here because it punctures the main sales story. It reports that these compounds are often sold for research use only while clearly meant for human consumption. That is a red flag, not a discount code.
A normal-budget reader does not need to become anti-peptide. Peptides are part of real medicine and biology. The better stance is stricter: documented public protocol over rumor, human outcomes over rodent excitement, clinician oversight over self-experimentation, and basic health behaviors before expensive novelty.
Frequently Asked Questions
Does Bryan Johnson publicly use BPC-157 or TB-500?
Not in the public Blueprint sources reviewed for this guide. The public material discloses oral collagen peptides, topical hair/scalp peptides, Follistatin gene therapy, and a Cerebrolysin trial, while BPC-157 and TB-500 appear in broader internet peptide discussions rather than as a documented Blueprint consumer stack.
Is collagen a peptide?
Hydrolyzed collagen contains smaller collagen peptides. The practical difference is route and risk: oral collagen behaves like a nutritional supplement, while injectable research peptides carry very different safety, sterility, legal, and medical questions.
What is the cheapest part of Blueprint worth copying?
The cheapest copy is not a product. It is the habit of tracking basics: consistent training, sleep, diet quality, and lab-guided deficiency correction. If you choose collagen, judge it like any other supplement: defined goal, defined time window, and no expectation that it replaces training or medical care.
Are research-use peptides safe if the vendor has good reviews?
Good reviews do not solve sterility, purity, dosing, degradation, or medical-fit problems. McGill's review notes that many trendy peptides are sold as research-use products while clearly aimed at human use, which is exactly why normal-budget buyers should be cautious.
Should athletes avoid peptide stacks?
Yes, unless a qualified medical and anti-doping professional clears a specific therapy. WADA lists BPC-157 under non-approved substances prohibited at all times, and growth-hormone-related peptides can create anti-doping risk even when the claimed benefit is uncertain.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











