
A Group of Muscles You Use Every Day Without Thinking About
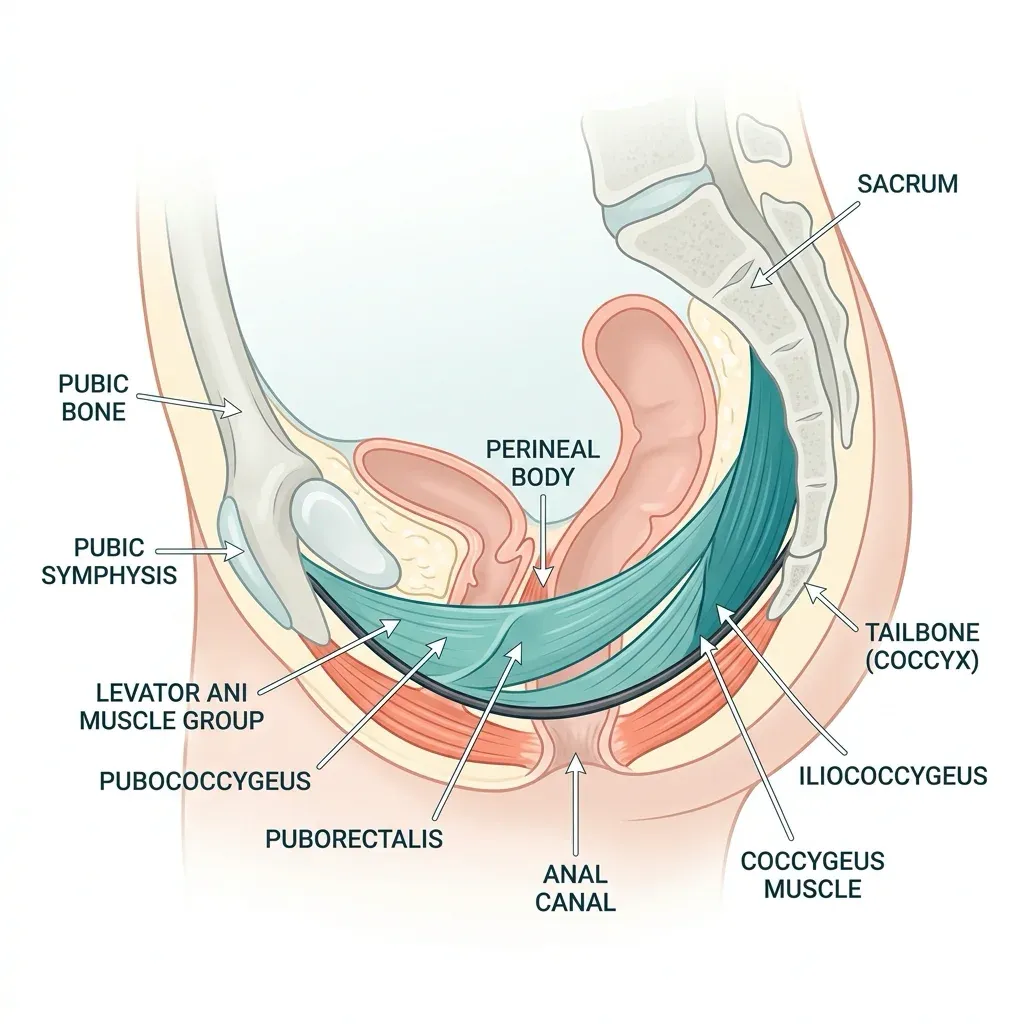
Somewhere between your hip bones sits a sling of muscle that most people never consider until something goes wrong. This muscular layer — the pelvic floor — stretches from the pubic bone at the front to the tailbone at the back, and it does far more than its reputation suggests.
The pelvic floor consists of the levator ani group (puborectalis, pubococcygeus, and iliococcygeus) and the coccygeus muscle, all innervated by sacral nerves at the S3, S4, and S5 levels. Together they form what researchers describe as a hammock-like structure that supports the bladder, uterus or prostate, and rectum. But support is only part of the job. These muscles also control the release of urine, stool, and gas. They stabilize the pelvis during movement. And they play a direct, measurable role in sexual function, breathing mechanics, and spinal stability.
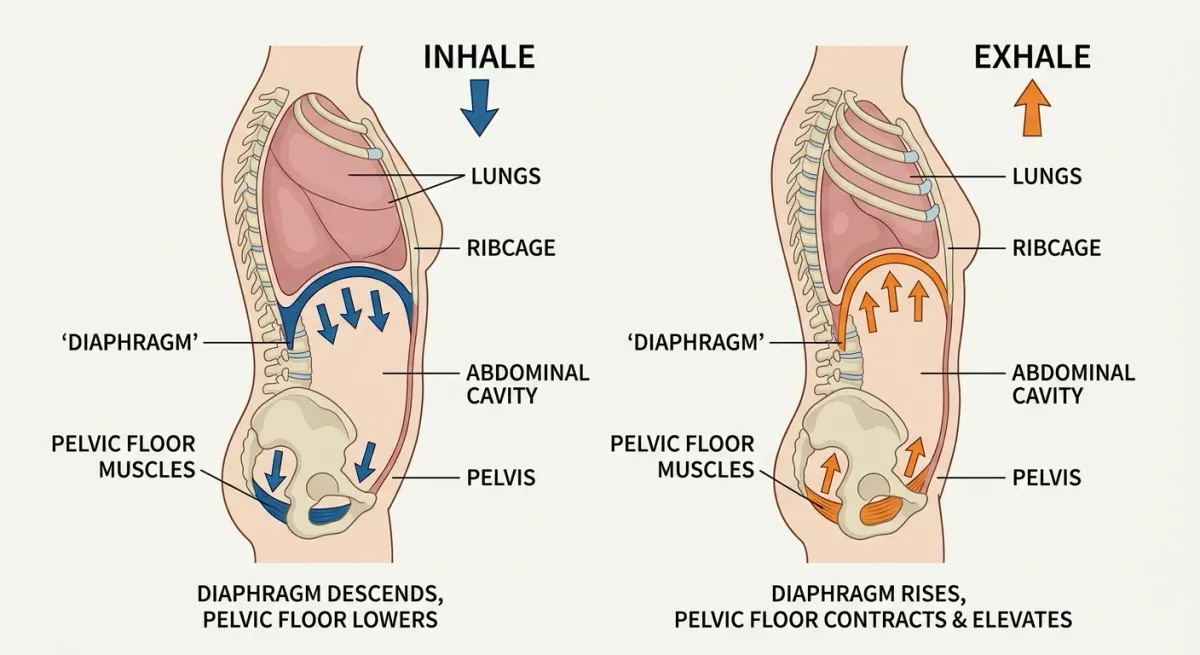
When you cough, the pelvic floor contracts reflexively to prevent leakage. When you lift something heavy, it co-activates with your deep abdominal muscles to manage intra-abdominal pressure. When you breathe, it moves in coordination with the diaphragm — descending during inhalation, rising during exhalation. A 2022 study using dynamic MRI confirmed that these muscles physiologically act as expiratory muscles working in synergy with the abdominal wall.
Quick fact: Pelvic floor disorders affect more than 28 million Americans, and nearly one in four women will experience symptoms at some point in their lives.
The pelvic floor also contributes directly to trunk stability. Research has demonstrated that pelvic floor muscles provide feedforward activation in response to trunk perturbation — firing before your conscious brain registers a shift in balance. This means pelvic floor weakness can ripple outward into problems you might never trace back to these muscles.
Half of Women Over 50 Will Deal With This — Here's What to Watch For
Pelvic floor dysfunction is not a single condition. It is an umbrella term for problems that arise when these muscles become too weak, too tight, or poorly coordinated. The three main categories are urinary incontinence, fecal incontinence, and pelvic organ prolapse — and they overlap more often than most people realize.
According to StatPearls clinical data, urinary incontinence alone affects 25 to 45 percent of women, with prevalence climbing above 40 percent in women over 70. Pelvic organ prolapse — where the bladder, uterus, or rectum drops from its normal position — affects more than half of women over 50, and carries a lifetime surgical risk of about 19 percent in Western populations.
| Symptom | What It May Indicate | How Common |
|---|---|---|
| Leaking urine when coughing, sneezing, or exercising | Stress urinary incontinence | Affects 25-45% of women |
| Sudden, urgent need to urinate | Urge incontinence | Increases with age |
| Pelvic heaviness or a "falling out" sensation | Pelvic organ prolapse | Over 50% of women 50+ |
| Chronic constipation or straining | Obstructive defecation / hypertonic PF | Roughly half of chronic constipation cases |
| Unexplained low back pain | Pelvic floor coordination failure | Linked to LBP in women |
| Pain during intercourse | Hypertonic (too-tight) pelvic floor | Variable |
What catches many people off guard is that dysfunction does not always mean weakness. A pelvic floor that is chronically tense — a hypertonic pelvic floor — can produce many of the same symptoms as a weak one. The Cleveland Clinic notes that pelvic floor dysfunction describes an inability to properly relax and coordinate these muscles, not just an inability to contract them. This distinction matters enormously when choosing exercises and treatments, because the standard advice to simply "squeeze harder" can make hypertonic conditions worse.
Left untreated, symptoms typically persist or worsen over time. But the encouraging finding across multiple studies is that most cases can be treated without surgery when caught early. Biofeedback training alone is effective for more than 75 percent of patients, and structured pelvic floor physical therapy produces measurable improvement in the majority of cases.
Arnold Kegel Published His Paper in 1948 — the Field Has Moved On
Kegel exercises remain the most recognized pelvic floor intervention on the planet. Arnold Kegel described them in 1948, and the basic concept has not changed: squeeze the muscles you would use to stop urinating, hold, release, repeat. The National Institute of Diabetes and Digestive and Kidney Diseases still recommends them as a starting point, and for good reason — they work for many people with stress incontinence.
But here is the problem. Research consistently shows that around 30 percent of women cannot properly contract their pelvic floor muscles even after receiving verbal instructions. Brief verbal instruction, the kind you get in a 10-minute doctor's appointment, often is not enough for beginners to learn the technique correctly. Some women bear down instead of lifting, which worsens the very issue they are trying to fix.
| Factor | Kegels Alone | Comprehensive Pelvic Floor Training |
|---|---|---|
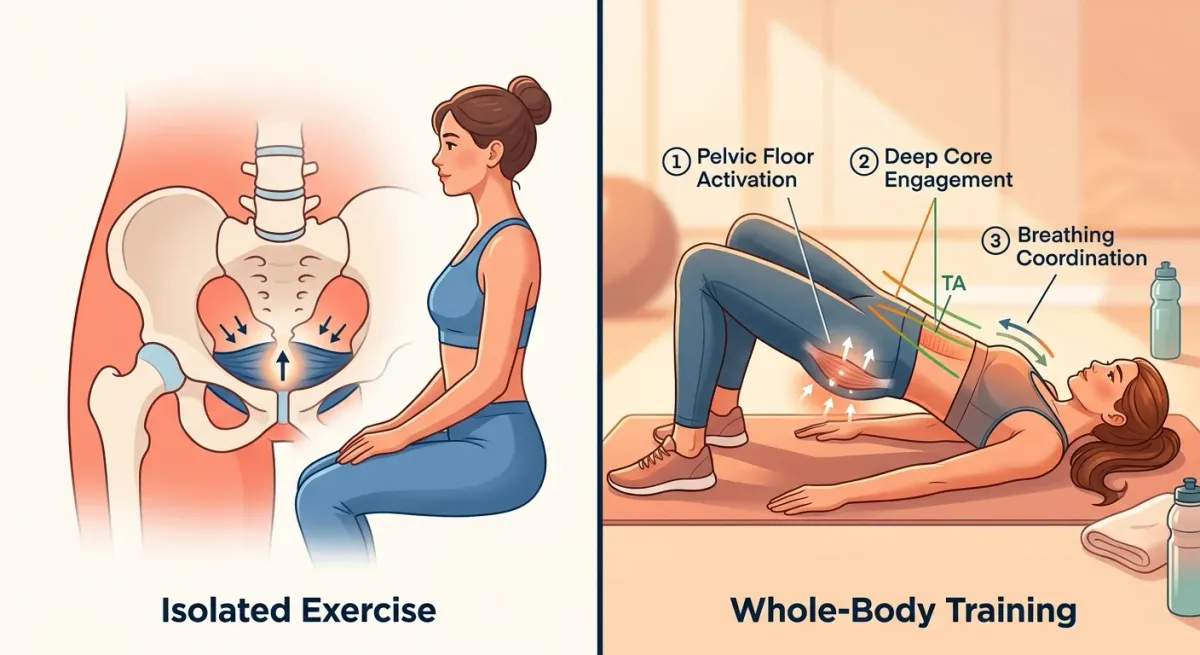
| Muscles targeted | Isolated PFM contraction | PFM + deep core + diaphragm coordination |
| Addresses hypertonic PF | No — may worsen tension | Yes — includes relaxation and lengthening |
| Breathing integration | Not typically included | Central component |
| Back pain benefit | Minimal evidence | Statistically significant pain reduction |
| Supervised outcomes | Often unsupervised | Supervised programs show superior results |
| Who benefits most | Mild stress incontinence | Incontinence, prolapse, pain, LBP, athletes |
Kegels also focus exclusively on contraction. They do not teach relaxation, lengthening, or coordination with breathing — all of which matter for a fully functional pelvic floor. A person with a hypertonic pelvic floor who does aggressive Kegel protocols may end up with more pain and more dysfunction, not less. This is why pelvic health specialists increasingly emphasize a broader training approach that treats these muscles as part of an integrated system rather than an isolated squeeze.
Kegels done in isolation also miss the pelvic floor's role in trunk stability. A 2022 randomized trial found that women with chronic low back pain who combined pelvic floor exercises with core stabilization saw significantly greater reductions in pain and disability than those doing stabilization alone — pain scores of 2.02 versus 2.84 on a 10-point scale. The pelvic floor functions as part of the muscular stability system surrounding the spine, and training it in isolation misses that role entirely.
Six Movements That Train the Whole System
The clinical evidence points toward a training approach that integrates the pelvic floor with the deep core, the diaphragm, and functional movement patterns. Here is what that looks like in practice, drawn from protocols used in the research studies reviewed for this guide.
1. Diaphragmatic breathing with pelvic floor awareness. Lie on your back with knees bent. Breathe in through your nose, letting your belly expand. As you exhale slowly through pursed lips, gently lift your pelvic floor as if stopping the flow of urine. The key is synchronization: the pelvic floor naturally rises during exhalation, so you are working with your body's built-in coordination rather than against it. Start with 5 minutes daily.
2. The bridge with pelvic floor engagement. From the same lying position, exhale and engage your pelvic floor as you lift your hips off the ground. Hold the bridge for 5 seconds at the top, maintaining steady breathing. Lower on an inhale. This trains the pelvic floor alongside the glutes and deep core in a functional pattern. Work up to 3 sets of 10.
3. Deep squat holds. Stand with feet slightly wider than hip-width. Lower into a deep squat (as low as comfortable), holding for 20 to 30 seconds. This position lengthens the pelvic floor muscles, which is particularly important for anyone with hypertonic symptoms. Focus on relaxing the pelvic floor during the hold rather than clenching. If you struggle with stress-related muscle tension, this exercise can serve double duty.
4. Bird-dog with exhale engagement. On hands and knees, extend opposite arm and leg while exhaling and drawing your pelvic floor upward. Hold 5 seconds. Return and switch sides. This challenges trunk stability while requiring real-time pelvic floor coordination — far more demanding than an isolated squeeze.
5. Standing hip hinge with coordinated breath. Stand with soft knees. Hinge at the hips as if reaching for the floor, inhaling on the way down (pelvic floor relaxes and lengthens). Exhale as you return to standing, pelvic floor lifting. This mimics real-life lifting mechanics and trains the muscles you will actually use when picking up groceries or a child.
6. Progressive Kegel protocol (for those who need it). The clinical standard from published trials recommends 3 sets of 8 to 12 contractions, each held for 8 to 10 seconds, performed 3 times daily for 15 to 20 weeks. Progress from lying to sitting to standing as strength improves. But this is one tool in the box, not the entire program.
Important: If you are doing these exercises correctly, your stomach, thighs, and buttocks should stay relatively relaxed. Tightening everything at once puts additional downward pressure on the bladder and can make leakage worse.
| Exercise | Primary Benefit | Best For | Sets / Duration |
|---|---|---|---|
| Diaphragmatic breathing + PF awareness | Coordination, relaxation | Hypertonic PF, beginners | 5 min daily |
| Bridge with PF engagement | Strength + core integration | Weak PF, post-pregnancy | 3 × 10 reps |
| Deep squat holds | Lengthening, relaxation | Hypertonic PF, tension-related pain | 3 × 20-30 sec |
| Bird-dog with exhale engagement | Stability, coordination | LBP, athletes | 3 × 8 per side |
| Standing hip hinge | Functional lifting pattern | All populations | 3 × 10 reps |
| Progressive Kegel protocol | Isolated PFM strength | Stress incontinence | 3 × 8-12, 3x/day |

One in Four Women — and More Men Than You'd Expect
Pelvic floor dysfunction is often framed as a women's health issue, and the numbers do reflect a gender skew. Columbia Surgery reports that nearly one quarter of all women face pelvic floor disorders, with prevalence rising steeply by decade: 10 percent of women aged 20 to 39, 27 percent of those 40 to 59, 37 percent in the 60 to 79 bracket, and nearly 50 percent of women over 80.
But men are not immune. Post-prostatectomy urinary incontinence affects between 1 and 60 percent of male patients depending on surgical technique, and a 2022 study of Norwegian powerlifters found that 9.3 percent of male athletes reported urinary incontinence, while 61.8 percent reported some degree of anal incontinence. Among female athletes in the same study, 50 percent had urinary incontinence and 80 percent had anal incontinence — numbers that should reframe the conversation around high-intensity training and pelvic health.
Athletes, paradoxically, face elevated risk. A 2024 systematic review in Sports Health found that female athletes are nearly three times more likely to experience urinary incontinence than sedentary women. Prevalence ranges from roughly 11 percent in low-impact sports like cycling to 80 percent in high-impact activities like trampoline gymnastics. The likely mechanism: repeated high intra-abdominal pressure during jumping, lifting, and impact activities stresses the pelvic floor, especially when combined with breath-holding.
The primary risk factors across all populations include:
- Pregnancy and vaginal delivery — the single largest risk factor for women
- Obesity — excess weight increases chronic downward pressure on pelvic organs
- Chronic constipation and straining — repeated bearing down weakens pelvic muscles
- Age — muscle mass and connective tissue integrity decline over time
- High-impact exercise with poor breathing mechanics
- Prior pelvic surgery — including prostatectomy, hysterectomy, and prolapse repair
Perhaps the most concerning finding from the weightlifter study: 43 percent of the women and 74 percent of the men did not know why pelvic floor training matters. The knowledge gap is substantial even among people whose activities put them at the highest risk. If you are doing regular cardiovascular or strength training, pelvic floor health deserves a place in your routine.
Your Diaphragm and Your Pelvic Floor Are Doing a Coordinated Dance
The relationship between breathing and pelvic floor function has become one of the more productive areas of recent research.
The pelvic floor and the thoracic diaphragm operate as a functional unit. During inhalation, the diaphragm contracts downward while the pelvic floor descends to accommodate the shift in abdominal pressure. During exhalation, both rise together. A 2015 study in the Journal of Physical Therapy Science measured this directly: pelvic floor contraction significantly increased maximum voluntary ventilation (p<0.05), confirming that the pelvic floor participates actively in respiratory mechanics. The researchers concluded that breathing is measurably more effective during pelvic floor contraction.
A 2022 paper in Healthcare used dynamic MRI to show what happens when you hold your breath during exertion — a habit common in weightlifting. During breath-holding, high intra-abdominal pressure pushes against the relaxed pelvic floor. The MRI showed it being slightly pushed downward despite the subject's effort to engage it. When the same exertion was performed during active exhalation, the pelvic floor and diaphragm moved upward together — protected.
The practical application: exhale during the effort phase of any exercise. This is the opposite of what many people instinctively do. When lifting weights, exhale as you push or pull. When doing a sit-up, exhale on the way up. When picking up a heavy box, breathe out as you stand. This simple adjustment coordinates pelvic floor protection with exertion rather than leaving the muscles vulnerable.
Stress enters the picture too. The Cleveland Clinic lists stress and anxiety as contributing causes of pelvic floor dysfunction — and the mechanism is physical. Chronic stress produces shallow, chest-dominant breathing that disrupts diaphragm-pelvic floor coordination. The muscles may become chronically tense in response to sustained anxiety and stress responses, which is why pelvic health therapists increasingly incorporate relaxation techniques and diaphragmatic breathing into treatment.
The research on gut-brain communication suggests that pelvic and abdominal tension may be both a symptom and a perpetuator of stress-related digestive issues — another reason to explore the breathing-pelvic floor connection with a qualified practitioner if chronic stress is part of your picture.
Frequently Asked Questions
How long does it take to see results from pelvic floor training?
Most people notice initial improvement within 3 to 6 weeks of consistent daily practice. However, the clinical protocols used in published studies run for 15 to 20 weeks to achieve more substantial strengthening effects. A minimum of 8 weeks is needed before muscles show measurable gains in endurance and contractile force. Consistency matters more than intensity — brief daily sessions outperform sporadic longer workouts.
Can men benefit from pelvic floor exercises?
Yes. Men have pelvic floor muscles with the same basic structure and function. Pelvic floor training is a standard recommendation after prostate surgery, where incontinence rates range from 1 to 60 percent depending on the procedure. Research on male weightlifters found that 9.3 percent experienced urinary incontinence during training, yet the overwhelming majority had never been taught pelvic floor exercises.
Should I stop doing Kegels entirely?
No. Kegels remain an effective, evidence-based intervention for stress urinary incontinence, and a 2025 meta-analysis found a 92 percent probability of benefit for postmenopausal women with incontinence. The point is not to abandon Kegels but to recognize them as one component of a broader approach. If you have symptoms of a hypertonic (overly tight) pelvic floor — pain during intercourse, difficulty emptying your bladder, chronic pelvic tension — Kegels alone may not be appropriate, and a pelvic health specialist can help determine the right balance.
Do high-impact sports damage the pelvic floor permanently?
Not necessarily. While athletes face higher incontinence rates — up to 80 percent in trampoline gymnastics — targeted pelvic floor training significantly reduces urine leakage in athletic populations. The key risk factor is improper breathing mechanics during exertion, not the exercise itself. Exhaling during effort and including pelvic floor work in athletic conditioning can substantially reduce risk.
When should I see a pelvic health specialist instead of exercising on my own?
Seek professional evaluation if symptoms persist beyond a few weeks, worsen with exercise, include pain during intercourse, or follow pelvic surgery or childbirth. Supervised pelvic floor training consistently produces better outcomes than self-directed programs — about 30 percent of women perform the exercises incorrectly without guidance. A specialist can determine whether your pelvic floor is hypertonic versus weak, which changes the treatment approach entirely.
Related Articles
- How Cortisol Drives Weight Gain and What Actually Helps — Chronic stress affects pelvic floor tension through the same cortisol pathways that drive abdominal weight gain.
- 7 Signs You May Have Anxiety (and What Your Body Is Really Telling You) — Anxiety-driven muscle tension can include the pelvic floor, contributing to hypertonic dysfunction.
- Zone 2 Cardio for Fat Burning and Longevity — Low-intensity exercise that supports pelvic floor health without the high-impact strain of intense training.
- Postpartum Depression vs. Baby Blues: Evidence-Based Guide to Recovery — Childbirth is the leading risk factor for pelvic floor dysfunction, and postpartum recovery involves both mental and physical rehabilitation.
- Gut-Brain Axis: How Your Microbiome Affects Mood and Cognition — The gut-brain connection intersects with pelvic floor function through shared neural pathways and abdominal tension patterns.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











