
Why the First Weeks After Birth Feel So Overwhelming
Something strange happens after the elation of delivery fades. Within 48 to 72 hours, many new mothers find themselves crying over nothing, snapping at partners, or lying awake even though exhaustion has settled into their bones. If that sounds familiar, you are not alone — and you are probably experiencing what clinicians call the "baby blues," a condition so common that a 2023 narrative review in the Journal of Personalized Medicine estimated its global prevalence at roughly 39 percent of all postpartum individuals.
But here is where things get complicated. Approximately one in seven mothers will go on to develop postpartum depression (PPD), a condition that shares early symptoms with the baby blues yet follows a different trajectory entirely. The two overlap in timing, look similar on the surface, and are easily confused — which is why an estimated 80 percent of PPD cases remain undiagnosed and untreated, according to a systematic review published in Cureus.
Knowing where baby blues end and postpartum depression begins is not an academic exercise. It is a clinical one with real consequences for both mothers and their children. This guide walks through the evidence on how to tell the difference, what drives each condition at a biological level, and which treatments actually work.
Baby Blues vs. Postpartum Depression: A Clinical Comparison
The terms "baby blues" and "postpartum depression" get used interchangeably in casual conversation, which creates a dangerous ambiguity. They are not the same condition. One resolves on its own. The other can persist for years without intervention.
| Feature | Baby Blues | Postpartum Depression |
|---|---|---|
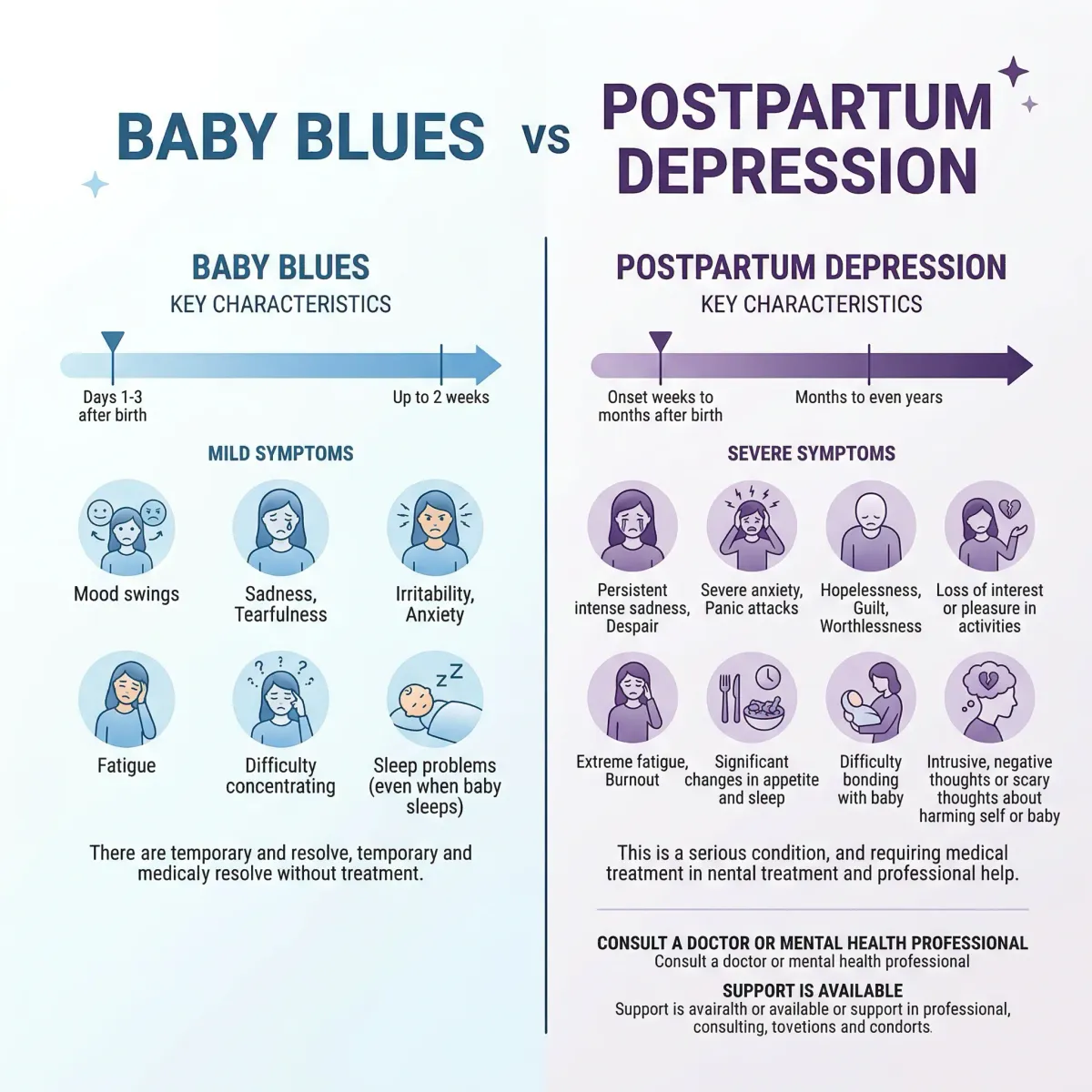
| Prevalence | 39-75% of postpartum individuals | 10-18% of postpartum individuals |
| Onset | Days 2-3 after delivery | Typically 4-8 weeks postpartum (can occur up to 1 year) |
| Duration | Resolves by day 10-14 | Months to years without treatment |
| Functional impact | Mild — can still care for infant | Significant — daily tasks become difficult |
| Suicidal thoughts | Not present | May be present |
| Treatment needed | Social support, rest, reassurance | Psychotherapy and/or medication |
| DSM-5 classification | No formal diagnosis | Major depressive episode with peripartum onset |
Key distinction: Baby blues are self-limiting. The tearfulness, mood swings, and irritability peak around the third to fifth postpartum day and fade before the end of the second week. If symptoms persist beyond 14 days, intensify rather than fade, or include thoughts of harming yourself or your baby, that is no longer baby blues — it is a medical condition that requires professional evaluation.
The baby blues lack a formal place in the DSM-5 or ICD-10 because they represent a transient adjustment rather than a psychiatric disorder. Postpartum depression, by contrast, meets the full clinical criteria for a major depressive episode — at least five persistent symptoms over a two-week period, including depressed mood or loss of interest in activities that once brought satisfaction.
What the baby blues and PPD share is a starting point: the hormonal free-fall that follows delivery. Where they diverge is in whether the brain's mood-regulation systems recover from that free-fall or get stuck in a depressive pattern. Understanding the biology behind that divergence is critical for knowing when to wait and when to act.
What Drives Postpartum Mood Changes at a Biological Level
Pregnancy is a hormonal construction project. Over nine months, estrogen and progesterone levels climb to roughly ten times their pre-pregnancy concentrations. After delivery, those levels collapse — returning to baseline within about three days, according to Cleveland Clinic. That plunge is among the fastest hormonal shifts the human body ever experiences, and it directly destabilizes multiple mood-regulation pathways.
The story goes deeper than just estrogen and progesterone. Research highlighted in the 2023 Journal of Personalized Medicine review points to several interconnected biological mechanisms:
| Biological System | What Happens After Delivery | Mood Consequence |
|---|---|---|
| Allopregnanolone (a progesterone derivative) | Sharp decline post-delivery | Reduced calming effect on GABA-A receptors, producing a withdrawal-like state |
| HPA axis (cortisol regulation) | Placental CRH drops suddenly; ACTH secretion spikes | Stress response dysregulation |
| Serotonin / Tryptophan | Tryptophan fails to rise in affected mothers as it does in unaffected mothers | Impaired serotonin synthesis, lower mood |
| Thyroid function | FT3 and FT4 fluctuations; possible thyroiditis | Fatigue, depression-mimicking symptoms |
The allopregnanolone connection deserves particular attention because it led directly to new treatments. Allopregnanolone is a neurosteroid that normally enhances GABA-A receptor activity — the same receptor system targeted by anti-anxiety medications like benzodiazepines. When allopregnanolone drops sharply after delivery, the resulting GABA-A underactivity can produce something functionally similar to a withdrawal syndrome. This mechanism explains why some mothers experience acute mood collapse while others — whose GABA systems adapt more quickly to the hormonal shift — experience only mild, self-correcting baby blues.
The relationship between cortisol and mood instability adds another layer. The HPA axis, which governs the body's stress response, is profoundly altered during pregnancy because the placenta itself produces cortisol-releasing hormone (CRH). When the placenta is delivered, that CRH supply vanishes overnight, leaving the maternal HPA axis temporarily unable to calibrate its stress response. In most women, this recalibration happens within a few weeks. In those who develop PPD, the recovery stalls.
Risk Factors That Increase Vulnerability
Not every new mother faces the same odds of developing postpartum depression. A 2022 meta-analysis across 33 studies and 133,313 participants quantified several key risk factors, and the numbers make clear which ones carry the most weight.
| Risk Factor | Odds Ratio | Clinical Significance |
|---|---|---|
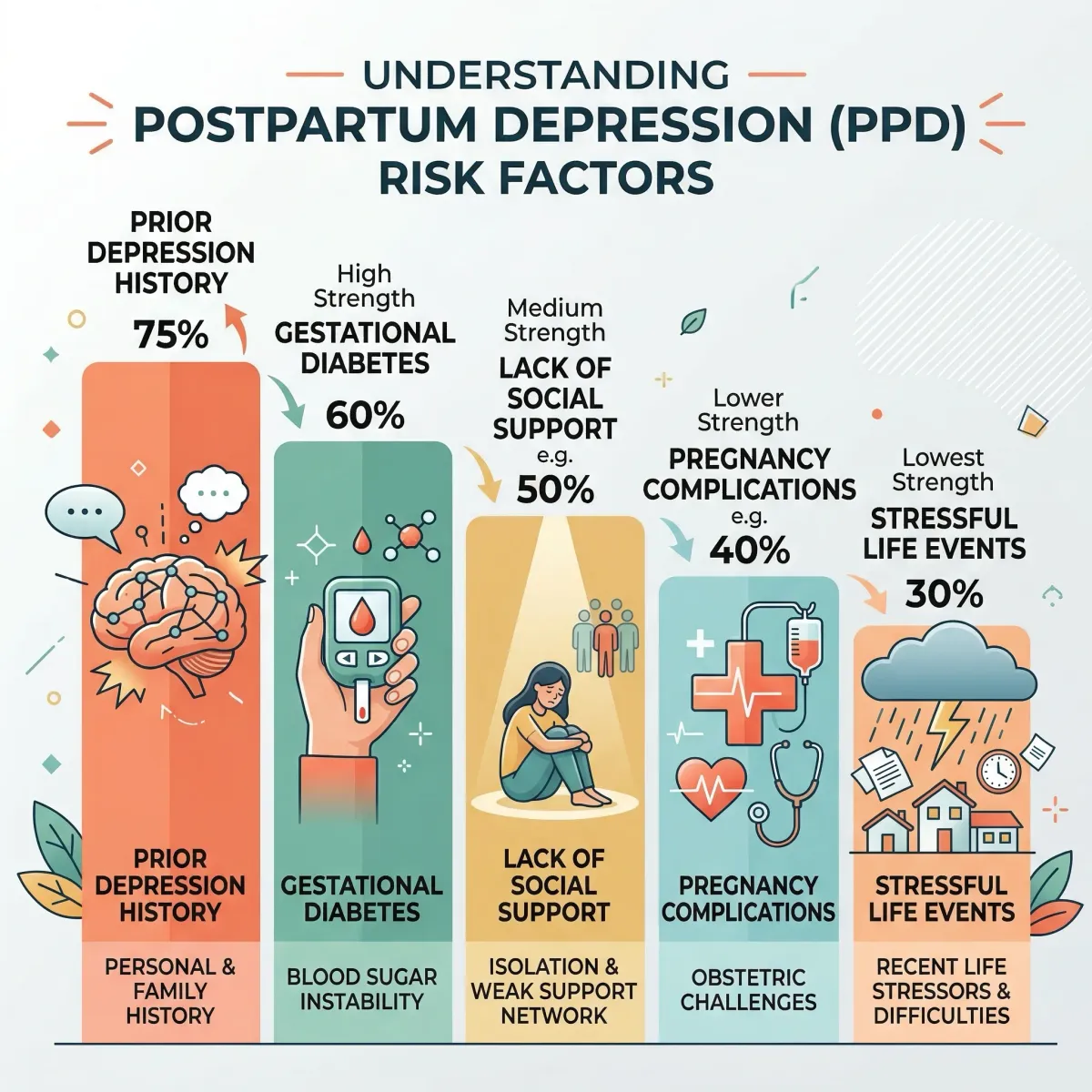
| History of depression during a previous pregnancy | 4.82 | Nearly 5x the risk — the single strongest predictor |
| Personal history of depression (non-pregnancy) | 3.09 | Prior mood disorders triple the likelihood |
| Gestational diabetes | 2.71 | Inflammatory pathways may mediate this connection |
| Depression during current pregnancy | 2.40 | Prenatal depressive symptoms strongly predict postpartum continuation |
| Lack of social/spousal support | Strong association | Consistently ranks among the most potent modifiable risk factors |
Several things stand out in the data. First, previous depression — particularly during a prior pregnancy — is by far the strongest single predictor. Women with that history face an approximately 40 percent chance of recurrence in subsequent pregnancies, according to the Cureus systematic review. Second, gestational diabetes appears as a risk factor that most people would not intuitively connect to depression, but the inflammatory cascade associated with insulin resistance may directly affect mood-regulating neurotransmitter systems.
The modifiable risk factors matter most in practical terms. Social support is among the strongest protective factors identified across multiple studies, and its absence is among the most consistent predictors of PPD. This is not limited to emotional support — practical help with infant care, household tasks, and sleep logistics makes a measurable difference. The Cureus review noted that spousal support specifically "helps lessen the strain on new mothers, thus mitigating the risk of PPD."
Health disparities also shape who gets screened and treated. CDC data from the Pregnancy Risk Assessment Monitoring System found postpartum depressive symptom rates exceeding 20 percent among women under 20, American Indian/Alaska Native women, and those who experienced intimate partner violence. And a 2024 analysis in the Journal of Clinical Medicine found PPD rates of 18 to 22 percent among women of color compared to 11 percent among white women — a gap that reflects both biological risk and systemic barriers to care.
Women recovering from iron deficiency face an additional compounding factor, since low ferritin levels during and after pregnancy can amplify fatigue and cognitive fog in ways that overlap with and worsen depressive symptoms.
Screening Tools and When to Seek Help
Given that an estimated 80 percent of PPD cases go undiagnosed, screening is not a formality — it is the bottleneck between illness and treatment. Yet CDC surveillance data shows that one in five women in the United States still does not receive prenatal depression screening, and one in eight is not screened after delivery.
The two most widely validated screening instruments are:
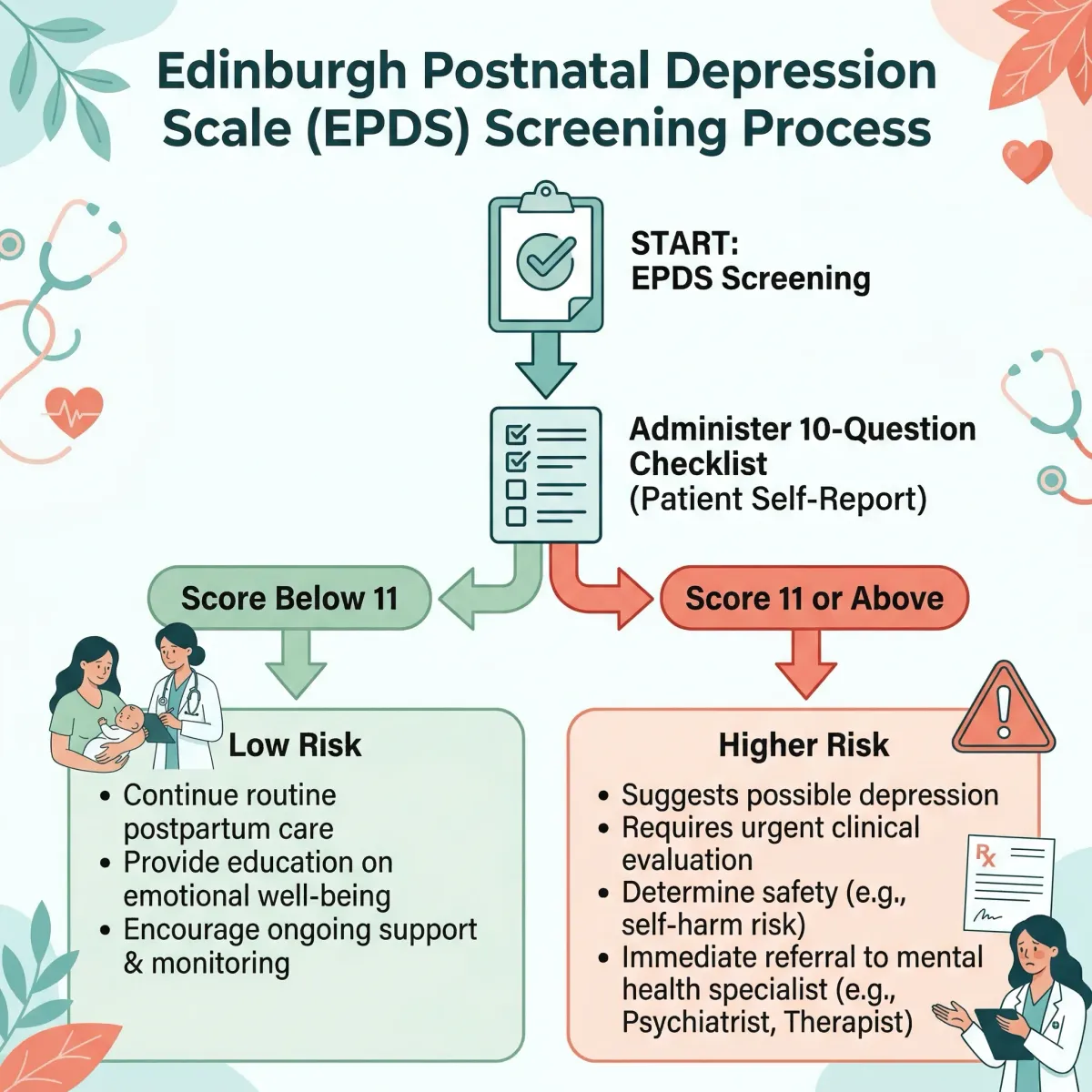
Edinburgh Postnatal Depression Scale (EPDS): A 10-item self-report questionnaire that takes under five minutes to complete. It is the most commonly used screening tool worldwide, available in over 60 languages. A meta-analysis of 58 validation studies found that a cutoff score of 11 (out of 30) provides the best balance of sensitivity and specificity for detecting clinical depression. The shorter EPDS-3 version — just the three anxiety-focused items — achieved 95 percent sensitivity and actually identified 16 percent more depressed mothers than the full scale.
Patient Health Questionnaire (PHQ-9 / PHQ-2): The PHQ-9 maps directly to DSM-5 major depression criteria, making it useful for both screening and severity assessment. The ultra-brief PHQ-2 version (two questions about depressed mood and loss of interest) is endorsed by both the American Academy of Pediatrics and ACOG for initial screening, though research shows it misses a meaningful number of women with clinical depression.
When to seek help immediately: Do not wait for a scheduled postpartum visit if you experience persistent sadness lasting more than two weeks, inability to care for yourself or your baby, thoughts of harming yourself or your infant, or severe anxiety symptoms that interfere with daily functioning. The National Maternal Mental Health Hotline (1-833-852-6262) provides free, confidential support around the clock.
Professional organizations including ACOG, the American Academy of Pediatrics, and the American Academy of Family Medicine now recommend universal screening during pregnancy and at postpartum visits. The evidence supporting this is straightforward: research consistently demonstrates that screening followed by clinical care leads to lower rates of depression and higher rates of treatment and remission.
Evidence-Based Treatment Options
Postpartum depression treatment has expanded considerably in recent years. The right approach depends on severity, breastfeeding status, and individual preference. What the evidence makes clear is that untreated PPD carries real risks for both mother and child.
Psychotherapy (mild to moderate PPD): Two forms of talk therapy have the strongest evidence base. Cognitive behavioral therapy (CBT) helps mothers identify and restructure thought patterns that fuel depressive spirals — catastrophizing about parenting ability, for example, or interpreting normal infant behavior as evidence of personal failure. Interpersonal therapy (IPT) focuses on the relationship disruptions and role transitions that come with new parenthood. Both approaches typically show results within 8 to 12 sessions. A 2025 scoping review of 49 prevention studies found that psychoeducational and mindfulness-based interventions also consistently reduce PPD risk, particularly when they incorporate family involvement.
SSRIs (moderate to severe PPD): Selective serotonin reuptake inhibitors remain the first-line pharmacological treatment, with sertraline and escitalopram most commonly prescribed. Sertraline carries particularly strong safety data for breastfeeding mothers, with minimal transfer into breast milk. Antidepressants typically require three to eight weeks to reach full therapeutic effect, and current guidelines recommend continuing treatment for at least six to twelve months after symptoms resolve to reduce relapse risk.
Newer targeted medications: Two drugs designed specifically for postpartum depression have changed the treatment picture considerably. Brexanolone, FDA-approved in March 2019, is a synthetic form of allopregnanolone — the same neurosteroid that plummets after delivery. Administered as a 60-hour IV infusion in a healthcare facility, it works by directly restoring GABA-A receptor activity. Zuranolone, approved in August 2023, works through a similar GABA mechanism but is taken orally for just 14 days. The American College of Obstetricians and Gynecologists describes zuranolone as the first oral medication approved specifically for postpartum depression.
The connection between gut health and mood regulation has also drawn attention in postpartum research. The gut-brain axis — the bidirectional communication pathway between intestinal microbiota and the central nervous system — undergoes significant shifts during pregnancy and the postpartum period. While this area is still under investigation, it underscores why whole-person approaches to recovery matter alongside targeted pharmacological treatment.
Recovery Timeline and What Partners Can Do
Recovery from postpartum depression is not a linear process, and timelines vary based on severity, treatment type, and individual biology. But the data offer a general framework.
| Treatment Approach | Expected Timeline to Improvement | Notes |
|---|---|---|
| Psychotherapy alone (CBT/IPT) | 4-8 weeks for noticeable improvement | 8-12 sessions typical course; most effective for mild-moderate PPD |
| SSRIs | 3-8 weeks for therapeutic effect | 6-12 months continuation recommended after remission |
| Zuranolone | Days (rapid onset) | 14-day oral course; some experience improvement within first week |
| Brexanolone | Within 60 hours (duration of infusion) | Requires inpatient administration; reserved for moderate-severe cases |
| Combined therapy + medication | 3-6 months for full recovery | Often the most effective approach for moderate-severe PPD |
The Cleveland Clinic notes that with professional help, nearly all individuals who experience postpartum depression can overcome their symptoms, with treatment typically spanning three to six months. However, without treatment the picture changes substantially: StatPearls data shows that approximately 25 percent of individuals with untreated perinatal depression continue experiencing symptoms for three years after giving birth, and roughly 30 percent remain depressed beyond one year.

What partners can do: Partner involvement is not a nice-to-have — it is one of the strongest modifiable factors in PPD outcomes. Research consistently shows that spousal support is directly associated with reduced PPD severity and faster recovery. Practical steps include:
- Take over specific nighttime feedings or infant care shifts so the mother can sleep in uninterrupted blocks (sleep deprivation is both a symptom and an aggravating factor)
- Attend at least one therapy session or medical appointment to understand the treatment plan and how to support it
- Learn the warning signs — if she says she is fine but has stopped eating, sleeping, or engaging with the baby, take that seriously
- Manage the household logistics that pile up: meals, laundry, visitors. Reducing decision fatigue matters more than most people realize
- Recognize that PPD is a medical condition, not a character flaw or a sign that something is wrong with the relationship
Hormonal transitions at any stage of life can affect mood and cognitive function. The postpartum period is one of the most acute hormonal shifts the body goes through, and treating it as a purely psychological event misses the biological reality.
Frequently Asked Questions
Can the baby blues turn into postpartum depression?
Yes. The baby blues are an established risk factor for developing postpartum depression. While most women's symptoms resolve within two weeks, those whose mood does not improve — or who notice symptoms intensifying rather than fading — should be evaluated promptly. The transition is not inevitable, but baby blues that persist beyond 14 days warrant clinical attention rather than a wait-and-see approach.
Is postpartum depression only caused by hormones?
Hormonal shifts are the trigger, but PPD is multifactorial. The rapid decline in estrogen, progesterone, and allopregnanolone after delivery creates the biological vulnerability, but whether depression develops also depends on genetic predisposition, personal psychiatric history, social support, sleep quality, and life stressors. Some women experience dramatic hormonal changes with no depressive symptoms, while others with smaller hormonal shifts develop significant depression — the difference lies in how multiple risk factors interact.
Can fathers or non-birthing partners get postpartum depression?
Yes. Research documents postpartum depression in fathers at rates of roughly 8 to 10 percent, driven by sleep deprivation, relationship stress, role adjustment, and in some cases hormonal changes (testosterone levels can drop in new fathers). Paternal PPD often co-occurs with maternal PPD, and screening both parents improves outcomes for the entire family.
Is it safe to take antidepressants while breastfeeding?
Several antidepressants — particularly sertraline — have extensive safety data showing minimal transfer into breast milk and no documented adverse effects on nursing infants. The decision involves weighing the small medication exposure against the well-documented risks of untreated maternal depression on infant development, including disrupted bonding, feeding difficulties, and developmental delays. This is a conversation to have with a prescribing physician, not a decision to make alone.
How long does postpartum depression last without treatment?
Without intervention, PPD can persist for years. Research from StatPearls indicates that approximately 25 percent of untreated individuals still have depressive symptoms three years after giving birth. A separate review found that about 30 percent of affected mothers remain depressed beyond one year postpartum. With appropriate treatment — therapy, medication, or both — most women recover within three to six months.
Related Articles
- How Cortisol Drives Weight Gain and What Actually Helps — Understanding the stress hormone connection that underlies postpartum mood changes.
- Iron Deficiency in Women: Symptoms, Testing, and Recovery — Postpartum iron depletion compounds fatigue and cognitive fog during recovery.
- 7 Signs You May Have Anxiety (and What Your Body Is Really Telling You) — Recognizing anxiety symptoms that often accompany or mimic postpartum depression.
- Gut-Brain Axis: How Your Microbiome Affects Mood and Cognition — The gut-brain connection that shifts during pregnancy and may influence postpartum mental health.
- Hormone Replacement Therapy (HRT) — Benefits, Risks, and Modern Evidence — How hormonal transitions at any life stage affect mood and cognitive function.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











