
An Estimated Two Million People Die from Liver Disease Every Year
That statistic from a 2024 Hepatology Forum review puts the scale of liver disease in perspective. Your liver handles over 500 biochemical processes, from filtering blood to manufacturing bile acids to converting stored glycogen into usable energy. It metabolizes every medication you take, processes every glass of wine, and neutralizes environmental toxins you absorb through food, air, and water.
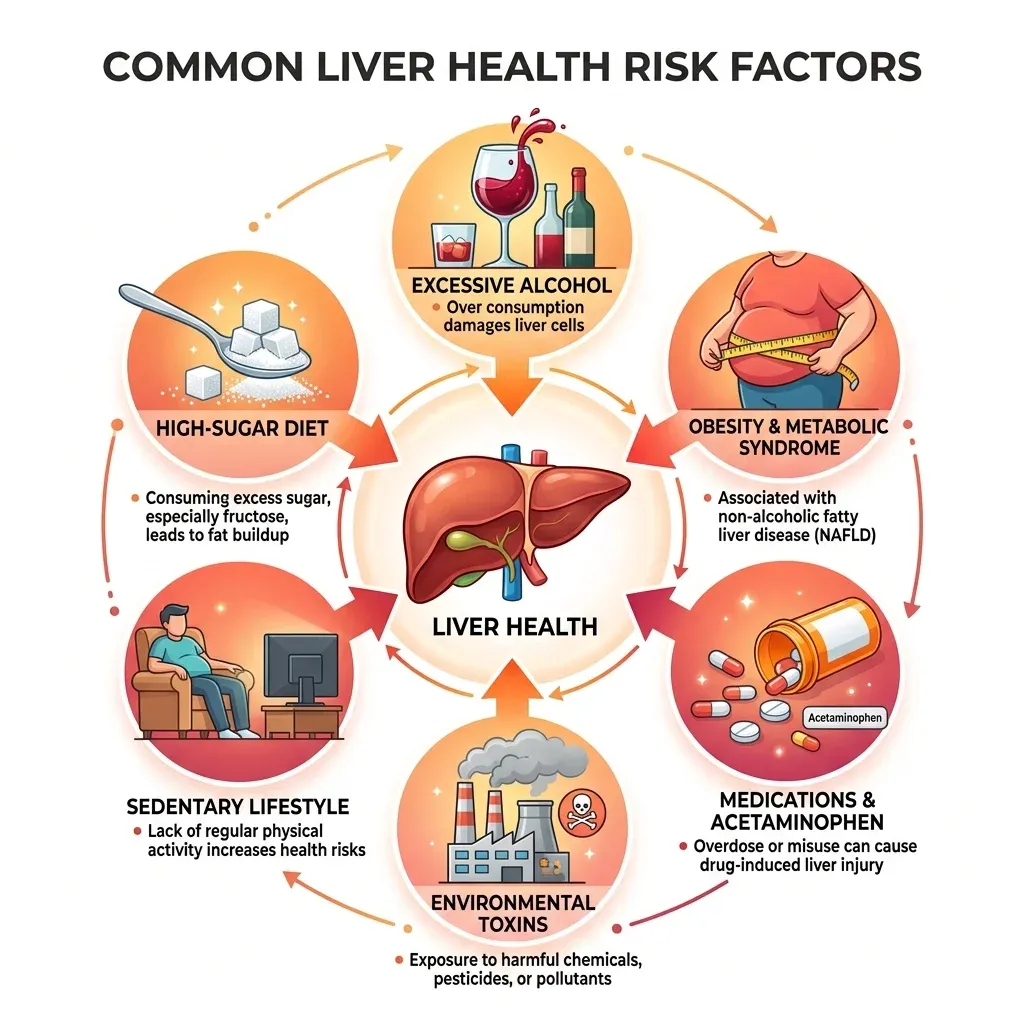
Yet most people never give their liver a second thought until blood work comes back with elevated enzymes. Non-alcoholic fatty liver disease alone now affects between 20 and 30 percent of adults in Western countries, a figure that climbs to 90 percent in obese populations. The progression from fatty deposits to inflammation to fibrosis to cirrhosis can happen quietly over years, without obvious symptoms until significant damage has accumulated.
The supplement industry has responded to rising liver disease rates with shelves of "liver detox" and "liver cleanse" products. Most of these rely on marketing rather than evidence. But buried within the noise are a handful of compounds with genuine clinical data behind them. Milk thistle and N-acetylcysteine (NAC) stand out as the most thoroughly studied, and a few other supplements have earned attention from researchers working on liver protection.
This guide examines what the clinical evidence actually supports, where the gaps remain, and how to distinguish supplements backed by randomized trials from those riding on tradition alone.
Milk Thistle Has Been Studied Since the 1960s, and the Data Are Promising but Complicated
Milk thistle (Silybum marianum) produces a group of flavonolignans collectively called silymarin. The most biologically active component, silybin, accounts for 50 to 70 percent of the total extract. It is the single most researched plant compound for liver disease, a distinction even the Cleveland Clinic acknowledges.
Silymarin works through three distinct mechanisms. First, it functions as an antioxidant that scavenges free radicals generated by the metabolism of ethanol, acetaminophen, and other hepatotoxins. Second, it downregulates inflammatory pathways including COX-2 and NF-kB signaling while increasing the anti-inflammatory cytokine IL-10. Third, it acts as an antifibrotic agent by blocking platelet-derived growth factor signaling, which prevents the stellate cells in your liver from transforming into the scar-tissue-producing myofibroblasts that drive fibrosis.
Quick fact: The European Medicines Agency has approved intravenous silibinin (the concentrated form of silybin) as an antidote for Amanita phalloides mushroom poisoning, one of the deadliest forms of acute liver failure.
What the Clinical Trials Show
The landmark trial most cited in silymarin research was conducted by Ferenci and colleagues, who gave 140 mg of silymarin three times daily to patients with liver cirrhosis. After following participants for four years, the survival rate was 58 percent in the silymarin group compared with 39 percent in the placebo group (p=0.036). Patients with alcoholic cirrhosis responded more strongly than those with other forms of the disease.
More recent data comes from a meta-analysis of eight randomized trials involving 587 patients with non-alcoholic fatty liver disease (NAFLD). Across these trials, silymarin supplementation reduced alanine aminotransferase (ALT) levels by an average of 9.16 U/L and aspartate aminotransferase (AST) by 6.57 U/L, both statistically significant findings.
In a 2022 double-blind trial of 52 obese patients with NAFLD awaiting bariatric surgery, those taking 560 mg of silymarin daily saw their rate of severe steatosis (Grade III on ultrasound) drop from 44.5 percent to 11.2 percent in just eight weeks. The placebo group showed modest improvement, but the difference between groups was significant (p=0.004).
| Trial / Review | Population | Silymarin Dose | Duration | Key Finding |
|---|---|---|---|---|
| Ferenci et al. (cirrhosis) | 170 cirrhotic patients | 140 mg TID | 41 months | 4-yr survival: 58% vs 39% |
| Meta-analysis, 8 RCTs (NAFLD) | 587 patients | Varied | 8-24 weeks | ALT -9.16 U/L, AST -6.57 U/L |
| Mirhashemi et al. 2022 (bariatric) | 52 obese NAFLD patients | 560 mg/day | 8 weeks | Grade III steatosis: 44.5% to 11.2% |
| Anushiravani et al. (NAFLD) | 150 patients, 5 arms | 140 mg/day | 3 months | Lower transaminases vs metformin |
The Bioavailability Problem
The primary limitation of milk thistle is absorption. Silymarin's oral bioavailability sits at only 20 to 50 percent, and the flavolignans are rapidly absorbed and eliminated. This explains why many clinical trials use higher doses than what appears on most supplement labels, and why researchers have developed phosphatidylcholine complexes (phytosomes) to improve delivery. If you are considering milk thistle supplementation, the formulation matters as much as the milligram count.
Typical research doses range from 420 to 600 mg of silymarin daily, split into two or three doses. Safety data supports doses up to 700 mg three times daily for 24 weeks without serious adverse events. Side effects, when they occur, tend to be mild gastrointestinal symptoms like bloating or loose stools.
Every Hospital in the Country Stocks NAC for a Reason
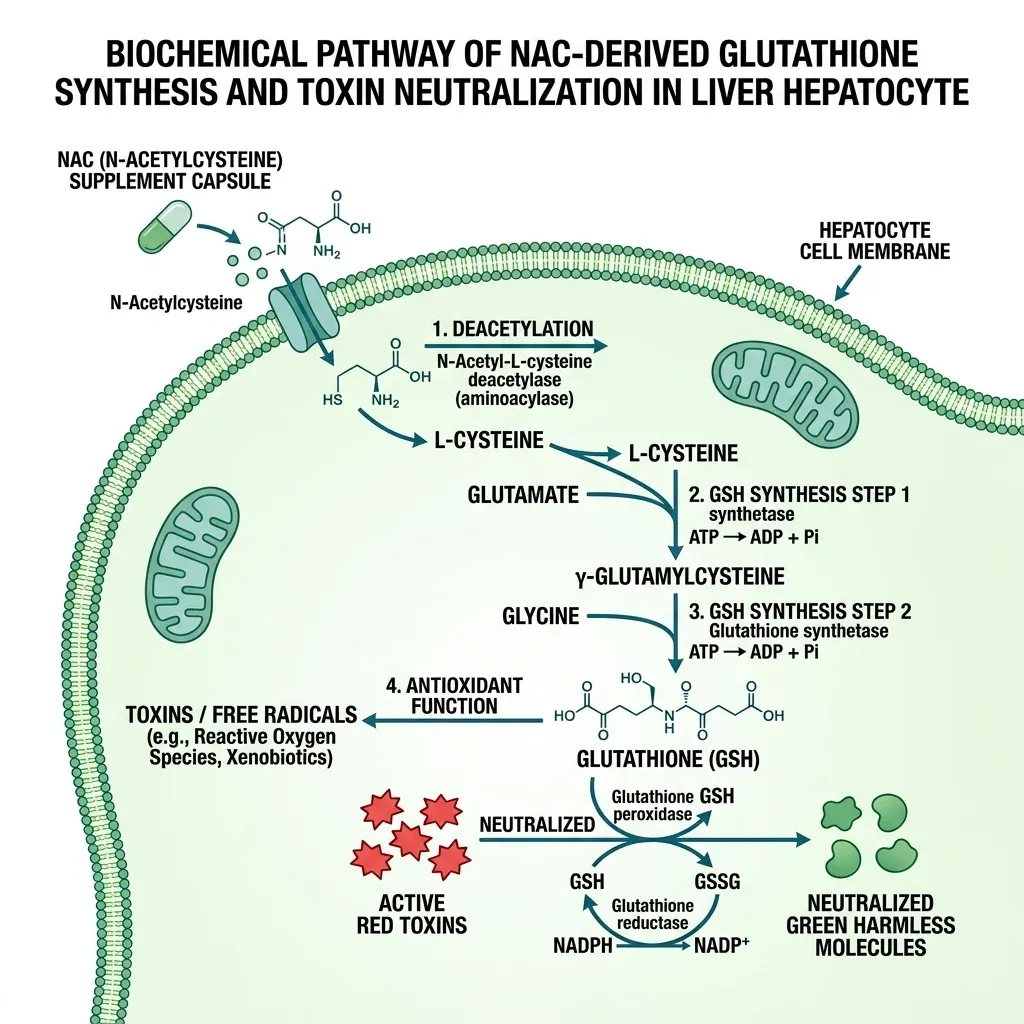
N-acetylcysteine earned its medical credentials in the most dramatic way possible. It is the standard antidote for acetaminophen overdose, the leading cause of acute liver failure in the United States. When administered within 10 hours of an overdose, NAC effectively prevents serious liver injury by replenishing glutathione, the master antioxidant that gets depleted when the liver is overwhelmed by the toxic acetaminophen metabolite NAPQI.
That emergency use case illustrates the core mechanism behind NAC's liver benefits. NAC is a precursor to L-cysteine, which your body uses to manufacture glutathione. Glutathione participates directly in Phase II liver detoxification, conjugating with toxins and reactive oxygen species to make them water-soluble and excretable. When glutathione stores drop, whether from chronic alcohol use, poor nutrition, illness, or simply aging, your liver's capacity to handle oxidative stress diminishes.
Beyond the ER: NAC for Chronic Liver Conditions
The research on NAC extends well beyond emergency medicine. A randomized trial at Tabriz University gave 600 mg of NAC twice daily to patients with NAFLD and tracked their liver enzymes for three months. ALT levels dropped from 77.0 to 51.7 U/L (p=0.014), and spleen size decreased from 121.3 to 116.2 mm (p=0.018), suggesting reduced fatty infiltration and portal hypertension.
For more advanced liver disease, a six-month RCT in cirrhotic patients found that 600 mg daily NAC significantly improved Child-Pugh scores (from 7.4 to 5.8) and MELD scores (median 12 to 9.5, p=0.009). The researchers noted that NAC also blocks transforming growth factor-beta (TGF-beta) signaling in fibrogenic cells, making it a direct anti-fibrotic agent in addition to its antioxidant role. A meta-analysis of 22 clinical trials covering 1,714 patients found that NAC outperformed both ursodeoxycholic acid and silibinin for ALT reduction in patients with hepatitis B.
Where NAC's evidence gets murkier is in non-acetaminophen acute liver failure. A 2022 review in the Saudi Journal of Gastroenterology noted that medical guidelines actually disagree on this: the European Association for the Study of the Liver (EASL) recommends NAC as standard care for early-stage liver failure regardless of cause, while the American Gastroenterological Association (AGA) limits its recommendation to clinical trials only. The most cited RCT (Lee et al., 173 patients) found no significant difference in overall three-week survival but did show improved transplant-free survival (40% vs 27%, p=0.043), particularly in patients with early-stage encephalopathy.
| NAC Application | Evidence Level | Typical Dose | Key Outcome |
|---|---|---|---|
| Acetaminophen overdose | Gold standard (all guidelines agree) | IV protocol or oral 70 mg/kg | Prevents liver failure if given within 10 hours |
| NAFLD | Moderate (multiple RCTs) | 600 mg BID | Reduced ALT, spleen size |
| Cirrhosis | Moderate (RCT + meta-analyses) | 600 mg daily | Improved Child-Pugh and MELD scores |
| Non-acetaminophen ALF | Uncertain (guidelines disagree) | Varies | Possible transplant-free survival benefit |
Three Other Supplements That Have Earned Serious Attention
Milk thistle and NAC dominate the liver supplement research landscape, but they are not the only compounds with credible evidence. Three others merit discussion based on their distinct mechanisms and growing clinical data.
TUDCA (Tauroursodeoxycholic Acid)
TUDCA is the taurine conjugate of ursodeoxycholic acid, a bile acid that occurs naturally in small amounts in human bile. It has been FDA-approved for cholestatic liver diseases based on its ability to protect hepatocytes and promote bile flow. What makes TUDCA distinctive is its mechanism: rather than working primarily as an antioxidant, it inhibits apoptosis (programmed cell death) by stabilizing the mitochondrial membrane, reducing endoplasmic reticulum stress, and preventing the accumulation of misfolded proteins. Chinese medicine has used bear bile, which is naturally rich in TUDCA, for over 3,000 years. Modern synthesis has made supplemental TUDCA widely available without the ethical issues of bear farming.
TUDCA's effects extend well past the liver. Research demonstrates it crosses the blood-brain barrier and shows neuroprotective effects in models of Alzheimer's, Parkinson's, and Huntington's disease. It increased insulin sensitivity by 30 percent in animal models. For liver health specifically, its choleretic and anti-apoptotic properties make it particularly relevant for people dealing with bile flow issues or cholestatic conditions.
Berberine
Berberine is an alkaloid found in goldenseal, barberry, and Oregon grape. Its relevance to liver health comes from a body of research showing it addresses several of the metabolic factors that drive NAFLD: insulin resistance, elevated cholesterol, and inflammation. A review of six clinical studies found that 1,000 to 1,500 mg daily significantly reduced ALT, LDL cholesterol, and postprandial glucose in patients with fatty liver disease. Combination therapy with conventional treatments further reduced triglycerides. If you are interested in berberine's cardiovascular effects as well, we have written more about berberine's role as a natural cholesterol fighter.
Curcumin
The active compound in turmeric has been studied across nine randomized trials for liver disease. The pooled data shows curcumin supplementation reduced ALT, AST, LDL cholesterol, fasting blood sugar, and markers of insulin resistance in NAFLD patients over two to three months. Like silymarin, curcumin faces a significant bioavailability problem: standard curcumin is poorly absorbed, and most clinical benefits appear only with enhanced formulations using piperine or phospholipid complexes. Curcumin's anti-inflammatory effect works partly through COX-2 inhibition, overlapping with but not duplicating silymarin's mechanism.
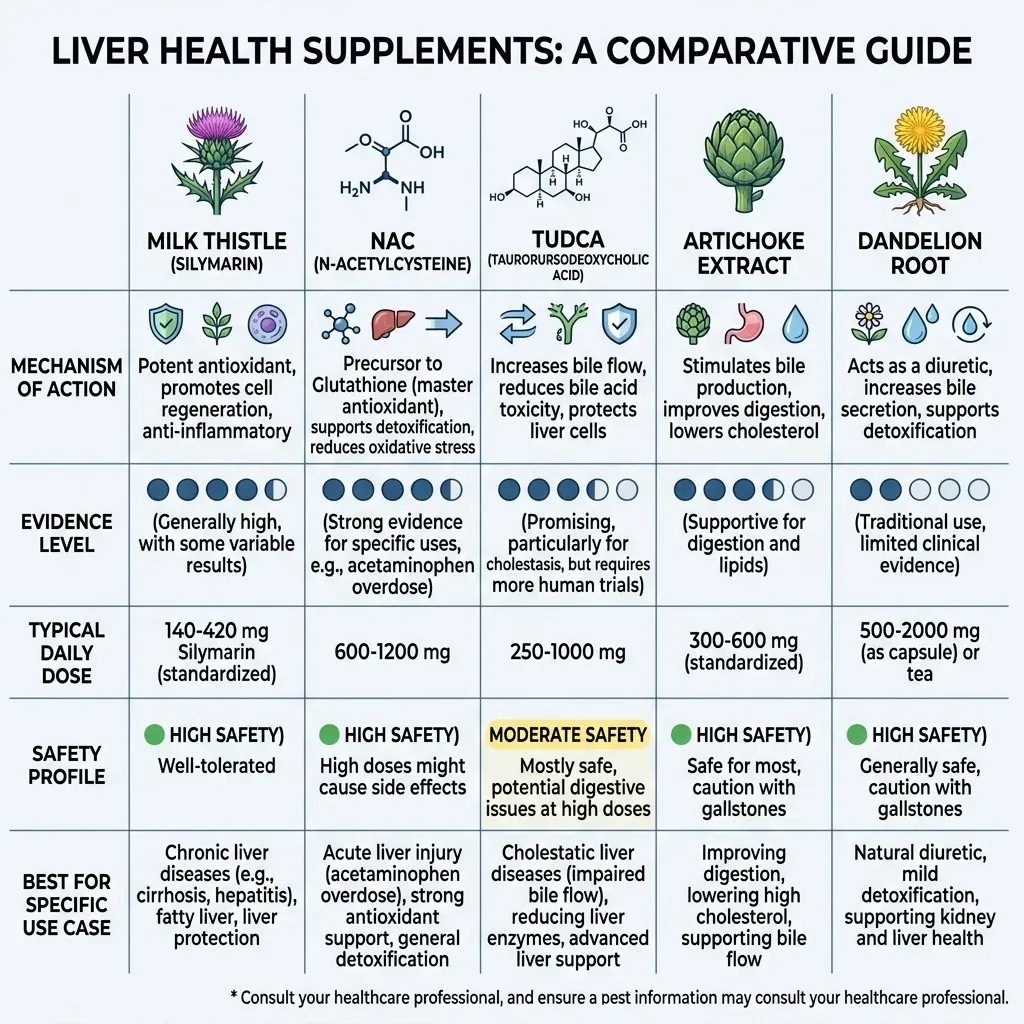
| Supplement | Primary Mechanism | Strongest Evidence For | Dose Range | Bioavailability Issue? |
|---|---|---|---|---|
| Milk Thistle (Silymarin) | Antioxidant + antifibrotic | NAFLD, cirrhosis survival | 420-600 mg/day | Yes (20-50%) |
| NAC | Glutathione precursor | Acetaminophen toxicity, NAFLD | 600-1200 mg/day | No |
| TUDCA | Anti-apoptotic, ER stress reduction | Cholestatic liver disease | 250-1500 mg/day | No |
| Berberine | Metabolic regulation | NAFLD (via insulin/lipid control) | 1000-1500 mg/day | Moderate |
| Curcumin | Anti-inflammatory | NAFLD enzyme reduction | 500-1500 mg/day | Yes (needs enhancement) |
Your Liver Does Not Need a Juice Cleanse to "Detox"
The word "detox" has become so warped by marketing that it barely communicates anything useful. Scroll through supplement ads and you will find activated charcoal drinks, dandelion root tinctures, and 14-day cleanse programs all promising to "flush toxins" from your liver. What your liver actually does is both simpler and more interesting than any of these products suggest.
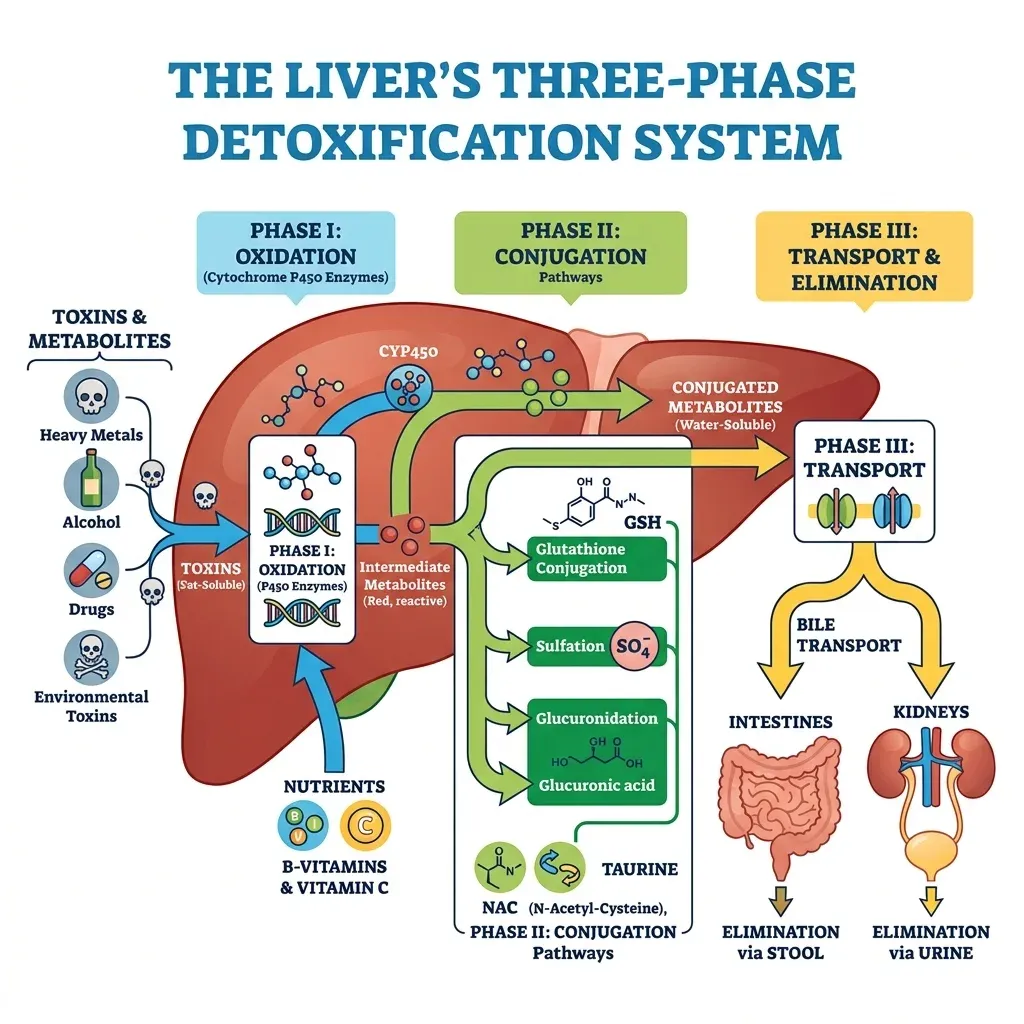
Your liver runs a continuous, sophisticated detoxification operation built around three enzymatic phases:
Phase I (Functionalization): Cytochrome P450 enzymes chemically modify toxins, drugs, and hormones, often making them temporarily more reactive. This is the step where acetaminophen gets converted into NAPQI, the toxic metabolite that NAC neutralizes.
Phase II (Conjugation): Transferase enzymes attach water-soluble molecules (glutathione, sulfate, glucuronic acid, glycine) to the Phase I products, rendering them excretable. This is where glutathione, the molecule NAC replenishes, does its heaviest work.
Phase III (Transport): Membrane transport proteins move the conjugated waste products into bile or blood for elimination through the intestines or kidneys.
When supplement marketers talk about "supporting detoxification," the only scientifically meaningful interpretation is ensuring your liver has adequate substrates and cofactors for these three phases. NAC contributes cysteine for glutathione synthesis. Silymarin enhances glutathione levels while simultaneously protecting hepatocytes from oxidative damage generated during Phase I. These are specific, measurable biochemical effects, not vague "toxin flushing."
The bottom line: A healthy liver detoxifies itself continuously. What evidence-based supplements do is support the biochemical machinery that makes this possible, particularly when that machinery is under strain from metabolic disease, alcohol, medications, or environmental exposures.
The relationship between your liver and your gut deserves mention here. The liver receives blood directly from the intestinal tract via the portal vein, meaning it serves as a first-pass filter for everything absorbed through your gut lining. When intestinal permeability increases, as happens with poor diet, chronic stress, or dysbiosis, the liver faces a heavier toxic burden. This is one reason researchers have grown interested in the gut-brain axis and the parallel liver-gut axis. Supporting gut health through polyphenol-rich foods may reduce the upstream load your liver must handle.
Some People Stand to Gain More Than Others
Liver support supplements are not equally useful for everyone. The research points to several populations that show the most consistent benefits:
People with NAFLD or early steatosis: Both silymarin and NAC have their strongest evidence in this population. The 2020 narrative review in Advances in Therapy specifically recommended starting silymarin "as early as possible in patients with fatty liver disease when the regenerative potential of the liver is still high." Waiting until cirrhosis has developed means working with a liver that has less capacity to respond.
Regular alcohol consumers: Ethanol metabolism generates acetaldehyde and free radicals that deplete hepatic glutathione. Both NAC (which replenishes glutathione directly) and silymarin (which enhances glutathione while blocking lipoperoxidation) address this mechanism. The Ferenci cirrhosis trial showed stronger results in patients with alcoholic cirrhosis than other forms.
People taking hepatotoxic medications: Acetaminophen is the obvious example, but statins, certain antibiotics, anti-tuberculosis drugs, and some chemotherapy agents also stress the liver. A meta-analysis of five trials covering 1,198 patients found silymarin significantly reduced the risk of anti-tuberculosis drug-induced liver injury. If you take medications metabolized by the liver, discussing supportive supplementation with your prescriber is worth the conversation.
Aging adults: Glutathione production naturally declines with age. NAC supplementation addresses this directly. Age-related declines in liver function compound with accumulated oxidative damage, metabolic changes, and the increased medication burden most older adults carry. Our discussion of NAD+ and NMN for cellular repair covers a related but distinct pathway in the aging equation.
Who Should Be Cautious
Supplements marketed for liver health can, paradoxically, cause liver injury. The American Association for the Study of Liver Diseases has noted that while herbal products are mostly safe, they can cause hepatotoxicities ranging from mild enzyme elevations to acute liver failure. The risk comes less from well-studied single-ingredient products like silymarin or NAC and more from multi-ingredient "liver cleanse" formulas, proprietary blends, and products contaminated with unlisted ingredients. The 2024 Hepatology Forum review emphasized that supplement toxicity more frequently stems from mislabeling, adulteration, and contamination than from the plants themselves.
Anyone with active liver disease should involve their hepatologist before starting supplements. Silymarin can interact with drugs metabolized by cytochrome P450 enzymes, and NAC at high intravenous doses can cause anaphylactoid reactions. Pregnant and breastfeeding individuals lack sufficient safety data for most liver supplements.
Frequently Asked Questions
Can milk thistle reverse liver damage that has already occurred?
Milk thistle appears most effective at slowing progression and supporting existing liver function rather than reversing established damage. The Ferenci trial showed improved survival in cirrhosis patients, but the liver architecture was not restored. Researchers have specifically noted that silymarin should be started early, when the liver still has regenerative potential. Once fibrosis has advanced to cirrhosis, the benefits diminish. For early-stage fatty liver disease, the data on enzyme normalization and reduced steatosis grading are more encouraging.
Is it safe to take milk thistle and NAC together?
There are no documented interactions between silymarin and NAC, and their mechanisms are complementary. Silymarin works primarily as an antioxidant and antifibrotic at the cellular membrane level, while NAC supplies the raw material (cysteine) for intracellular glutathione synthesis. Some practitioners combine them for this reason. That said, combining supplements should always be discussed with a healthcare provider, particularly for people taking prescription medications or managing active liver disease.
How long does it take for liver supplements to show measurable effects?
Most clinical trials showing significant results ran for at least eight weeks, with many extending to three to six months. The bariatric surgery study showed ultrasound-detectable improvements in steatosis grading within eight weeks on silymarin. NAC reduced ALT levels measurably within three months. Expecting changes in under a month is unrealistic based on the existing trial data. Liver enzymes measured through routine blood work offer the most accessible way to track progress.
Do "liver cleanse" or "liver detox" products actually work?
Most commercial liver cleanse products contain a mix of herbs, vitamins, and sometimes proprietary blends with no clinical evidence behind the specific combination. The concept of needing to "cleanse" your liver misrepresents how the organ works. Your liver continuously detoxifies through enzymatic pathways that require specific nutrients and cofactors. Products making dramatic detox claims generally lack the clinical trial data that supports individual compounds like silymarin, NAC, or TUDCA.
Should healthy people without liver issues take liver support supplements?
The research base for liver supplements focuses overwhelmingly on populations with existing liver disease or elevated risk factors. There is limited evidence that supplementation provides meaningful benefit to people with normal liver function, a healthy diet, moderate or no alcohol intake, and no hepatotoxic medication exposure. NAC does support general glutathione levels, which decline with age, but a food-first approach emphasizing cruciferous vegetables, sulfur-rich foods, and adequate protein provides the same substrates through diet.
Related Articles
- Health Benefits of Turmeric — Curcumin's anti-inflammatory and liver-protective properties are closely related to the compounds discussed in this guide.
- Berberine: A Natural Cholesterol Fighter for Heart Health — Berberine's metabolic effects extend to NAFLD through its impact on insulin resistance and lipid metabolism.
- NAD+ and NMN Supplements for Aging and Cellular Repair — NAD+ depletion parallels glutathione decline as a driver of age-related cellular dysfunction.
- The Gut-Brain Axis: How Your Microbiome Affects Mood and Cognition — The liver-gut axis shares key pathways with the gut-brain connection explored here.
- Polyphenol-Rich Foods for Heart Health — Many polyphenols that benefit the cardiovascular system also support hepatic antioxidant defenses.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











