Roughly one in three men prescribed Viagra never gets the result they paid for. Sildenafil and tadalafil work by relaxing penile blood vessels, but if the brain is not sending an arousal signal, or if the vascular damage is too severe, there is nothing for a PDE5 inhibitor to amplify. PT-141, also called bremelanotide, skips the plumbing and activates melanocortin receptors in the hypothalamus, the brain region that initiates sexual desire and the descending signals that produce erection. The peptide began as an experimental tanning agent in the 1980s, became Pfizer's most promising non-PDE5 ED candidate of the 2000s, was halted over a blood-pressure signal, then re-emerged in 2019 as Vyleesi, approved only for premenopausal women. Off-label male use has quietly exploded through telehealth and compounding pharmacies. This guide walks through what the human male trials actually showed, why the FDA wouldn't sign off for ED, and where the gray-market reality leaves men in 2026.
From sunless-tanning peptide to erection drug
PT-141 began in a University of Arizona dermatology lab. In the early 1980s, pharmacologists Mac E. Hadley and Robert T. Dorr designed two synthetic, enzymatically resistant analogs of alpha-MSH, the body's own pigmentation hormone, and named them Melanotan I and Melanotan II. The original goal was a "therapeutic tan" that might lower skin cancer risk. Hadley and Dorr patented both molecules and licensed them to Palatin Technologies, with Melanotan II redirected to male erectile dysfunction after unexpected sexual side effects appeared.
The pivot was an accident. Dermatologist Norman Levine, running early Melanotan II tanning trials, observed male volunteers presenting with sustained erections after their injections. Duration tracked with dose and outperformed placebo. The melanocortin system was doing two things at once: pigment in the skin, and arousal circuitry in the hypothalamus.
Palatin isolated the carboxylate metabolite of Melanotan II, a seven-amino-acid peptide called PT-141, or bremelanotide. By the early 2000s, Palatin had partnered with King Pharmaceuticals to take an intranasal version into Phase II for male ED. Then it stalled. King was acquired by Pfizer in 2010, the same Pfizer that holds the Viagra franchise. Innerbody's research desk has flagged the unusually quiet decade between 2007 and 2019 in the male-ED literature. The likelier explanation, which the FDA's own Vyleesi review supports, is that a blood-pressure signal in the larger intranasal trials was incompatible with the typical ED patient's cardiovascular-risk profile. The male program shelved itself, and Palatin pivoted toward female low-desire, eventually winning FDA approval in June 2019 for Vyleesi, a 1.75 mg subcutaneous auto-injector for premenopausal women with HSDD only.
Brain vs. blood flow: why melanocortin-4 works when PDE5 fails
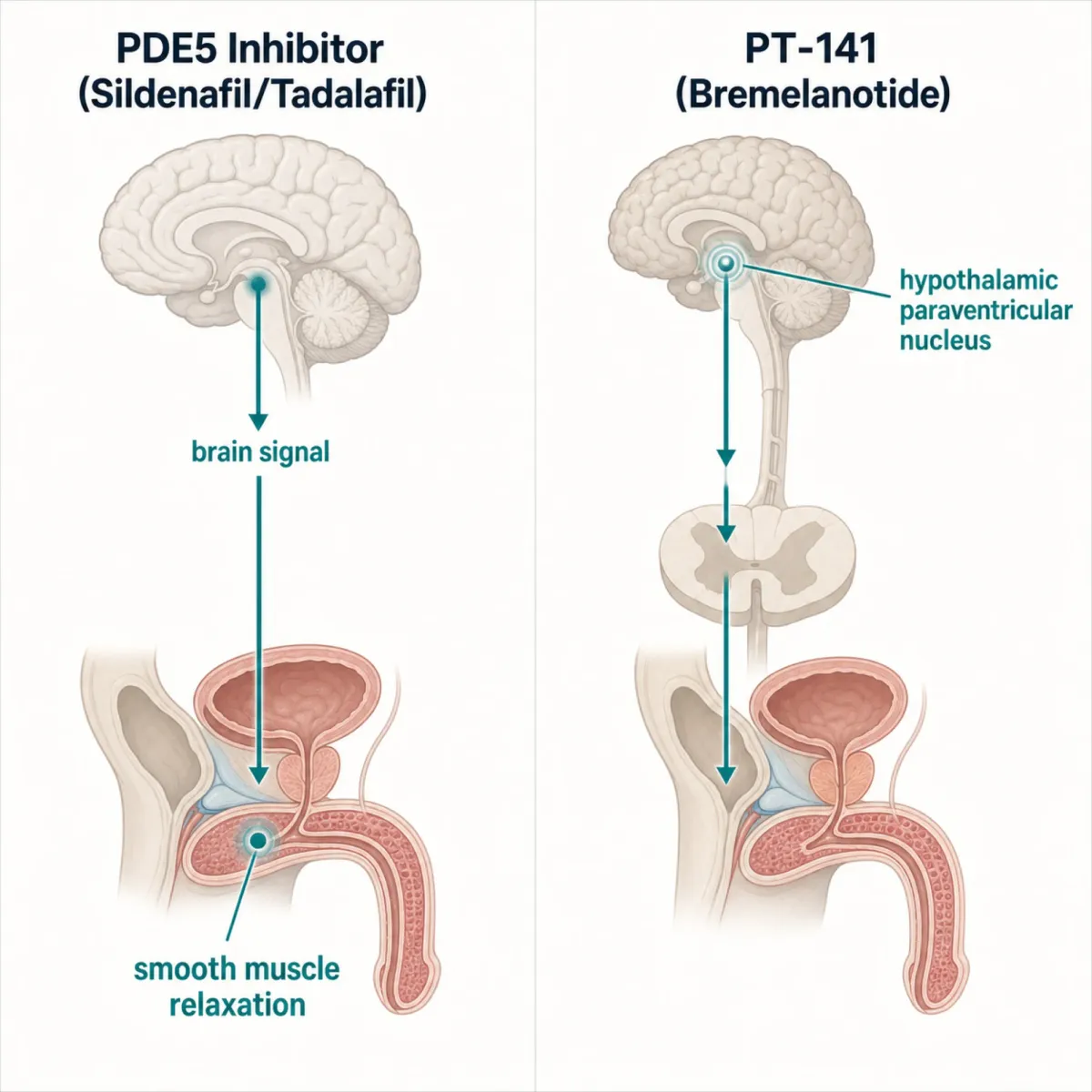
To see why PT-141 sometimes succeeds where sildenafil fails, draw the wiring of an erection. Sexual cues activate neurons in the hypothalamus's medial preoptic area and paraventricular nucleus. They fire descending signals down the spinal cord to the cavernous nerves, which release nitric oxide into the corpus cavernosum's smooth muscle. Smooth muscle relaxes, blood pours in, venous outflow compresses.
PDE5 inhibitors (sildenafil, tadalafil, vardenafil, avanafil) intervene at the last step. They block phosphodiesterase type 5, the enzyme that breaks down cyclic GMP, the messenger that keeps smooth muscle relaxed. With PDE5 inhibited, cGMP accumulates and relaxation persists long enough for blood to fill the cavernosum. Boston University's Sexual Medicine division puts the consequence cleanly: PDE5 inhibitors do nothing without an upstream sexual signal. They're amplifiers, not initiators.
PT-141 plugs in at the opposite end. It binds the melanocortin receptor family (MC1R, MC3R, MC4R) with strongest affinity for MC4R, which sits on neurons in the very paraventricular nucleus where sexual cues do their initiating work. Hunter Wessells's 2005 review in Peptides mapped the circuitry: melanocortin agonism in the PVN triggers oxytocin release and dopaminergic outflow to the spinal cord, producing both subjective desire and the autonomic signal for erection. Martin and MacIntyre's 2004 European Urology review confirmed MC4R carries the pro-erectile signal.
If the problem is downstream (healthy smooth muscle but a sluggish cGMP cascade), a PDE5 inhibitor works fine. If the problem is upstream — the brain not sending the signal because of psychogenic factors, neurogenic damage, or testosterone deficiency — flooding the cavernosum with PDE5 inhibition gives the body nothing to amplify. PT-141 attacks that upstream block directly.
The 30–40% PDE5 non-responder population
The marketing for sildenafil and tadalafil suggests near-universal effectiveness. The literature tells a different story: roughly 30% to 40% of men on PDE5 inhibitors do not respond satisfactorily even after dose optimization, the same figure Palatin Technologies cited in its 2023 announcement of a Phase II co-formulation program.
The non-responder bucket has recognizable subgroups: men with severe penile vascular disease, where diabetes or atherosclerosis has damaged the cavernous tissue badly enough that no amount of cGMP preservation matters; post-radical-prostatectomy neurogenic ED, where surgical injury to the cavernous nerves disrupts the very nitric-oxide signal a PDE5 inhibitor is designed to potentiate; psychogenic and CNS-driven ED, where the upstream arousal signal is the bottleneck; untreated hypogonadism, where low testosterone flattens both libido and the brain's sexual-cue processing; and antihypertensive or antidepressant interactions that dampen central arousal. Yale's Soum Lokeshwar and colleagues in World Journal of Men's Health place the neurogenic and psychogenic groups at the center of the search for non-PDE5 mechanisms.
For PT-141, the second through fourth subgroups are the patients in whom a brain-targeted agonist might restore something a peripheral drug cannot. The Safarinejad trial was designed around exactly this idea: take men in whom Viagra had been confirmed to fail and see whether activating the melanocortin system rescued any of them.
What the human male trials actually showed
The male-ED clinical record is small but specific. Three studies anchor the conversation.
Diamond, Earle, Heiman et al., Phase I, intranasal, 2004. The proof-of-concept trial was a randomized, double-blind, placebo-controlled study in 24 men with mild-to-moderate ED. Subjects received intranasal PT-141 from 4 mg to 20 mg, with no visual sexual stimulation. The headline RigiScan number: men on the highest PT-141 dose showed 140 minutes of rigid erection versus 22 minutes in placebo. Onset 34 to 63 minutes after dosing.
Diamond et al., Co-administration with sildenafil, 2005. The same group then tested whether combining a low PT-141 dose with a low sildenafil dose produced additive effects. The trial enrolled 32 men and gave each sildenafil at 50 mg or 100 mg with or without intranasal PT-141 at 7.5 mg or 10 mg, monitored over six hours by RigiScan. Co-administration enhanced erectile-response duration by an average factor of 5.3 (range 1.9 to 8.3) versus sildenafil alone, statistically significant in three of four comparisons, with no serious adverse events.
Safarinejad, Salvage of sildenafil failures, 2008. The most clinically important male-ED trial came four years later. Mohammad Reza Safarinejad recruited 448 men with ED and ran them through an aggressive sildenafil re-education protocol: written instructions on food timing, alcohol avoidance, and 12 home doses (11 at the maximum 100 mg) before declaring failure. Only 13% responded to re-education. The remaining 388 confirmed non-responders enrolled, with 304 completing the protocol, randomized to intranasal bremelanotide or placebo and re-challenged with sildenafil. The bremelanotide arm achieved a 33.5% rate of intercourse-grade erection. Placebo: 8.5%. The difference reached statistical significance at p = 0.03. Adverse events (predominantly nausea, flushing, and diaphoresis) were significantly more common in the bremelanotide group.
Together those studies make the male-ED case in plain numbers: PT-141 works, it nearly quadruples the response rate in confirmed Viagra failures, it stacks productively with PDE5 inhibitors, and the mechanism is consistent with Wessells's foundational rat work that established the Penile Erection Index methodology. None were Phase 3 trials. None enrolled the thousands of subjects modern approval requires. And the safety signal that killed the male program (transient blood-pressure elevation) never went away.
PT-141 plus sildenafil for refractory ED
The most clinically interesting result is the combination data, not the monotherapy. The 2005 Diamond co-administration trial demonstrated a true mechanistic synergy: sildenafil amplifies cGMP downstream in the cavernosum, PT-141 generates the central arousal signal that initiates the cascade, and stacking them runs erectile response 5.3 times longer than sildenafil alone, a magnitude that, if reproducible at scale, would be the most meaningful ED advance since Viagra's 1998 approval.
Palatin Technologies has bet on this thesis. In August 2023 the company initiated a clinical program developing bremelanotide co-formulated with a PDE5 inhibitor for the indication of ED in PDE5i non-responders, the same 30–40% subgroup. Bundling two mechanisms into one prescribable product is the deliberate regulatory strategy.
Whether the program reaches market depends on the same blood-pressure question that derailed the original male trajectory. Combining a transient pressor (PT-141) with a transient depressor (sildenafil) might cancel out, or produce unpredictable hemodynamic swings in a population enriched for hypertension. For now, the combination remains off-label. Strive Pharmacy's Olympus Peak is a single compounded preparation containing 1 mg bremelanotide, 20 mg tadalafil, and 20 IU oxytocin, the multi-mechanism stack the published trials hint at, marketed without trial-level safety data on the specific combination.
Why FDA said no for male ED: the blood pressure problem
The most important document in the bremelanotide story is the FDA Multi-Discipline Review for NDA 210557, the 2019 Vyleesi approval package. Its safety analysis contains the exact reason the agency would not have signed off on the molecule for male ED.
From the reviewer's summary: bremelanotide transiently raised mean systolic and diastolic blood pressure by 3 mmHg and transiently lowered heart rate by approximately 2 bpm. Changes returned to baseline by 12 hours post-dose, no cumulative effect across repeated dosing. MedlinePlus's Vyleesi monograph distills the same finding for patients.
For a young, healthy, premenopausal woman with no cardiovascular history, the exact Vyleesi indication, those numbers are clinically tolerable under the labeling FDA imposed: contraindication in uncontrolled hypertension or known cardiovascular disease, a warning about BP elevation, a 24-hour minimum interval between doses, and a hard cap of eight doses per month. The Phase 3 trials excluded women with uncontrolled hypertension or known cardiovascular disease, and did not establish safety in postmenopausal women.
For the typical man with ED, every one of those qualifications cuts the wrong way. ED is itself a marker of endothelial dysfunction; men presenting for ED treatment are disproportionately older, hypertensive, dyslipidemic, and at elevated cardiovascular risk. Contraindicating "uncontrolled hypertension or known cardiovascular disease" in a male-ED population rules out close to half the indication. The intranasal PT-141 male program was halted in 2007 for the same signal at higher delivered doses. Until a Phase 3 trial demonstrates cardiovascular safety in actual male-ED patients, not a curated cohort of low-risk healthy women, the FDA position on male PT-141 is essentially a deferred no.
Off-label use in 2026: telehealth, compounding, and gray-market vendors
None of that has stopped the off-label market. In 2026, men obtain PT-141 through three channels.
Telehealth peptide clinics. Online platforms like Hone Health, Marek Health, Healthon, and Boston Medical Group pair an online consultation with a licensed prescriber and a compounding pharmacy. Typical regimens: 1–2 mg subcutaneous, self-injected 30 to 60 minutes before sexual activity. The prescription is off-label, which U.S. medical practice permits.
Compounding pharmacies prescribing direct. Strive Pharmacy, Pharmacy & Compounding NW Florida, and Sarasota Compounding Pharmacy represent the many 503A and 503B compounders preparing bremelanotide products to a physician prescription — including triple-stack products combining PT-141 with tadalafil and oxytocin. The triple-stack approach has no published Phase 3 safety data and matches no FDA-approved formulation.
Gray-market "research peptide" suppliers. The unregulated channel. Online vendors sell PT-141 powder labeled "for research purposes only — not for human consumption," often with no prescription required. Daniel Imperiale, Managing Editor at Innerbody Research, has been explicit that this is the route to avoid: the "research chemical" label exempts vendors from FDA quality oversight, third-party purity testing is rare, and contamination, mislabeling, or sub-potency are recurring problems across the unregulated peptide trade.

WADA status, named skeptics, and the quality-risk reality check
Two questions come up at the end of any peptide deep-dive: is it banned in sport, and what do the skeptics actually say?
On the doping question, as of May 2026 bremelanotide is not on the World Anti-Doping Agency Prohibited List by name. The WADA 2025 Prohibited List, in force through the 2026 calendar year, does not enumerate bremelanotide, melanocortin agonists, or PT-141 in any substance category. The negative finding triangulates across WADA's landing page, the Wikipedia compiled list, and the BSCG reference. The caveat: WADA's S2 category covers "other substances with similar chemical structure or similar biological effects," giving WADA latitude to read a melanocortin agonist as in-scope. Tested athletes should treat the current absence as not-listed-but-not-cleared and verify with their national anti-doping organization.
On the skeptic side, the most consistent voice is consumer-facing. Daniel Imperiale, Managing Editor at Innerbody Research, is on record that PT-141 is not the right tool for the vast majority of men with ED — citing the side-effect profile (40% nausea in female Phase 3 trials, transient hypertension, hyperpigmentation), injection friction, cost relative to generic sildenafil and tadalafil, and four decades of PDE5 safety data. Jim Staheli, medical director at Broad Health, takes the conservative clinical line in the same analysis: men with cardiac disease, uncontrolled hypertension, severe liver disease, or renal failure should avoid PT-141 entirely. He further warns against combining PT-141 with PDE5 inhibitors in hypertensive men — a warning that runs counter to the Olympus Peak-style triple-stack products some compounding pharmacies are already selling.
Irwin Goldstein, Director of San Diego Sexual Medicine, takes the intermediate position closer to the Palatin co-formulation thesis: he acknowledges the 30–40% PDE5 non-responder rate and argues the rational treatment is a combined central-plus-peripheral mechanism — not PT-141 alone, not Viagra alone. That view bridges the skeptics and the Palatin Phase II program: the disagreement is less about whether PT-141 has value than whether it should ever be used as monotherapy.
For the female arousal context — the FDA Vyleesi approval pathway and how the same melanocortin pathway works on desire rather than blood flow — the companion article on PT-141 bremelanotide and the female Viagra desire mechanism covers the data Palatin used to win the indication.
Frequently asked questions
Is PT-141 FDA-approved for men?
No. Bremelanotide is approved only as Vyleesi for premenopausal women with hypoactive sexual desire disorder. MedlinePlus is explicit that the injection should not be used for HSDD in postmenopausal women, in men, or to improve sexual performance. Any prescription for a man is off-label.
Can PT-141 work where Viagra failed?
The 2008 Safarinejad salvage trial: in 304 men with rigorously confirmed sildenafil non-response, intranasal PT-141 produced a 33.5% rate of intercourse-grade erection versus 8.5% on placebo, a roughly 1-in-3 rescue rate. The caveat is that all this work used the intranasal form, no longer a regulated product, and the modern subcutaneous formulation has not been re-tested in confirmed PDE5 non-responders at Phase 3 scale.
What dose do men typically use off-label?
Telehealth platforms and compounding pharmacies typically prescribe 1 to 2 mg subcutaneous, self-injected 30 to 60 minutes before sexual activity. The FDA-approved Vyleesi female dose is 1.75 mg, with a 24-hour minimum interval and eight-dose monthly cap; male off-label protocols generally respect the same limits, since they're driven by the same blood-pressure data.
Why did the FDA reject PT-141 for male ED?
The agency never formally rejected a male-ED NDA, Palatin shelved the intranasal program in 2007 before filing, but the issue is documented in the FDA's 2019 Vyleesi review: transient BP increase of ~3 mmHg systolic and a transient heart-rate decrease of ~2 bpm, with a contraindication for uncontrolled hypertension or known cardiovascular disease. Vyleesi was approvable for low-cardiovascular-risk premenopausal women. The male-ED population, older, hypertensive, atherosclerotic, is a different risk calculation.
Is bremelanotide on the WADA banned list?
As of the WADA 2025 Prohibited List, in force for 2026, bremelanotide is not enumerated by name. The negative result triangulates across the WADA 2025 list PDF, the Wikipedia compiled list, and BSCG's reference document. The S2 peptide-hormone category does contain an open clause covering "other substances with similar chemical structure or similar biological effects" that gives WADA latitude to interpret a melanocortin agonist as in-scope.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.