What 95,000 Swedish patients revealed about semaglutide and depression
A drug designed to lower blood sugar may be doing something unexpected to the brain. In April 2026, a team led by Dr. Heidi Taipale at the Karolinska Institutet published findings in The Lancet Psychiatry that tracked 95,490 people across Sweden who had both a diagnosed mood disorder (depression, anxiety, or both) and were taking medication for diabetes. Among them, 22,480 used a GLP-1 receptor agonist at some point during the study period, and 13,445 specifically used semaglutide -- the active ingredient in Ozempic and Wegovy.
During periods when these patients were taking semaglutide, their risk of worsening mental illness dropped by 42% compared to periods when the same individuals were not taking GLP-1 medications (adjusted hazard ratio 0.58, 95% CI 0.51-0.65). "Worsening mental illness" wasn't a vague self-report -- the researchers defined it as a composite of psychiatric hospitalisation, sick leave exceeding 14 days for psychiatric reasons, hospitalisation for self-harm, or death by suicide.
The secondary outcomes were more specific. Semaglutide users saw a 44% reduction in worsening depression (aHR 0.56), a 38% reduction in worsening anxiety (aHR 0.62), and a 47% reduction in worsening substance use disorder (aHR 0.53). Psychiatric sick leave dropped too: an aHR of 0.55 for semaglutide, meaning 45% fewer sick days for psychiatric reasons during treatment periods.
Liraglutide, an older GLP-1 drug, also showed benefits -- but weaker ones. Its overall risk reduction was 18% (aHR 0.82), and it only reached significance for depression, not anxiety or substance use. Two other GLP-1 drugs, exenatide and dulaglutide, showed no mental health association at all (both aHR approximately 1.01).
That differential is one of the most interesting parts of the data. If the mental health benefit came simply from losing weight or from feeling better about taking any medication, you'd expect all four GLP-1 drugs to show similar effects. They didn't. Semaglutide stood apart -- and when the researchers directly compared it against other GLP-1 medications in the 3,705 people who used both semaglutide and another GLP-1 drug, semaglutide still came out ahead (aHR 0.67). This isn't a class effect. Something specific is happening with semaglutide.
The researchers also tested semaglutide head-to-head against empagliflozin, an SGLT2 inhibitor used for diabetes that serves as an active comparator. Semaglutide still showed a 27% lower risk of worsening mental illness (aHR 0.73) -- ruling out the possibility that any diabetes treatment would produce the same result.
Three pathways semaglutide may use to reach your brain
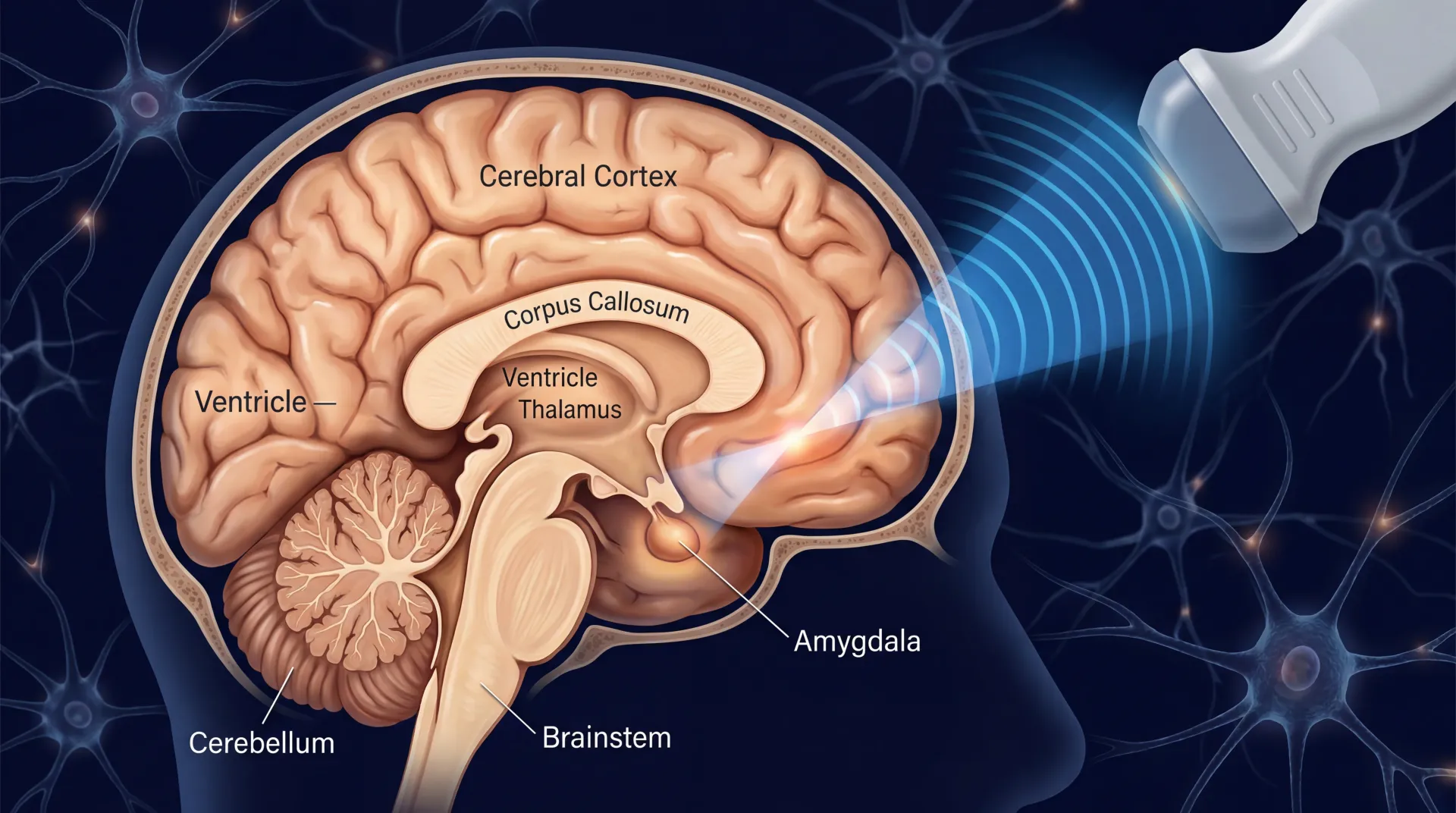
Semaglutide was designed to work on the gut and pancreas. But GLP-1 receptors aren't confined to the digestive tract. They're scattered across brain regions that regulate mood, reward, and stress -- and understanding where these receptors sit helps explain why a diabetes drug might affect how people feel.
Pathway 1: Dampening neuroinflammation. Think of chronic inflammation in the brain like static on a radio -- it doesn't stop the music entirely, but it degrades the signal until everything sounds distorted. GLP-1 receptor activation reduces that static. According to a systematic review published in Frontiers in Behavioral Neuroscience, GLP-1 decreases inflammatory markers including TNF-alpha and IL-6, while simultaneously reducing microglial activation -- the brain's immune cells that, when chronically triggered, damage the neural environment. The same review found that GLP-1 promotes neurogenesis through brain-derived neurotrophic factor (BDNF), a protein sometimes called "fertilizer for neurons." Depression consistently correlates with lower BDNF levels, so a drug that increases BDNF production could, in theory, support the biological infrastructure that mood regulation depends on.
Pathway 2: Modulating the reward system. GLP-1 receptors are densely expressed in areas of the mesolimbic reward pathway -- the circuitry responsible for motivation, pleasure, and craving. Stanford psychiatrist Dr. Anna Lembke, author of Dopamine Nation, described GLP-1 drugs as targeting "the brain's dopamine reward system", influencing dopamine release in regions linked to motivation and pleasure. This isn't just about food cravings -- the same reward circuitry goes haywire in depression, where patients often lose the ability to feel pleasure (anhedonia) or become trapped in compulsive behaviors. GLP-1 receptors sit alongside dopamine terminals in the lateral septum and are colocalized with dopamine-receptor-expressing cells, meaning they're physically positioned to modulate dopamine uptake, clearance, and transporter expression.
Pathway 3: Stress hormone regulation. The hypothalamic-pituitary-adrenal (HPA) axis governs the body's cortisol response -- and HPA dysregulation is one of the most consistent biological findings in depression. A systematic review in Diabetes, Obesity and Metabolism found that GLP-1 signalling modulates corticotropin-releasing hormone (CRH) neurons in the paraventricular nucleus of the hypothalamus. By recalibrating CRH output, GLP-1 drugs could potentially normalize the cortisol surges that characterize anxious and depressive states.
One piece of human evidence adds texture to these animal findings. A post-mortem investigation cited in a 2025 Nature Mental Health review found that people who had lived with mood disorders showed lower expression of the GLP-1 receptor gene in the dorsolateral prefrontal cortex and hippocampus compared to healthy controls. This association wasn't present in the brain tissue of people with schizophrenia, suggesting a specific relationship between GLP-1 receptor activity and mood -- not psychosis broadly.
There's also a curiosity from animal research: acute doses of GLP-1 drugs can actually increase anxiety-like behavior in rodents. But chronic administration normalizes it -- a pattern that mirrors how conventional antidepressants work (SSRIs often worsen anxiety before they improve it). This temporal pattern hints that GLP-1 drugs may engage serotonergic pathways in ways that parallel established psychiatric medications.
Why these numbers don't mean what you think they mean
Before anyone prints prescription pads based on the Swedish study, the researchers themselves -- and every independent expert who reviewed the paper -- issued the same caveat: this is an observational study. It cannot prove causation.
Dr. Vincenzo Oliva, a researcher at the Institute of Biomedical Research in Barcelona, stressed that the study measured "lower risk of worsening" rather than direct symptom improvement. That distinction matters. The study didn't measure whether people felt less depressed. It measured whether they were hospitalised less often, took fewer psychiatric sick days, and harmed themselves less frequently. Those are meaningful outcomes, but they're not the same as demonstrating that semaglutide treats depression.
Prof. Eduard Vieta, Chair of Psychiatry at the University of Barcelona, went further. These findings "should not yet be interpreted as evidence of a direct therapeutic effect on depression or anxiety," he wrote, noting that residual confounding cannot be fully excluded and that the COVID-19 pandemic may have influenced the results during parts of the study period.
The Swedish study's within-individual design is genuinely strong -- comparing the same person's outcomes during on-drug versus off-drug periods eliminates many of the biases that plague typical observational research (gender differences, baseline illness severity, genetic factors all cancel out). But it can't account for everything. The national registers used in the study didn't include data on weight change, HbA1c levels, or BMI. That's a significant gap, because we can't tell whether people felt better because of a direct brain effect or because losing 15% of their body weight improved their self-image, mobility, sleep, and social interactions -- all of which independently affect mental health.
Prof. Ian Maidment at Aston University summarized the core limitation plainly: the study showed that certain GLP-1 agonists are associated with lower risk of worsening mental illness, "but this needs testing in full clinical trials."
A 2025 BMJ study by Shapiro and colleagues provides a useful cautionary example. When they looked at GLP-1 receptor agonist users in UK primary care data, crude analysis showed GLP-1 users had roughly double the rate of suicidality compared to DPP-4 inhibitor users (HR 2.08). Alarming on its surface. But after adjusting for confounders -- the fact that GLP-1 users tend to have higher BMI, more comorbidities, and greater baseline psychiatric burden -- the association evaporated entirely (HR 1.02). The apparent signal was just confounding by indication, not a drug effect.
The Swedish study's within-individual design avoids much of this confounding, but it still cannot account for time-varying factors like weight loss, dietary changes, or improved diabetes control that coincide with GLP-1 treatment periods.
The broader evidence: from FDA reversals to failed predictions
The Swedish study didn't emerge in a vacuum. It landed in a research landscape that has been arguing about GLP-1 drugs and mental health for years -- and the overall picture has shifted considerably.
In January 2026, the U.S. Food and Drug Administration requested that manufacturers remove suicidal behavior and ideation warnings from GLP-1 drug labels. The FDA's review, covering 91 clinical trials and 107,910 patients, found no increased risk of suicidal thoughts or behavior compared to placebo -- and no increase in other psychiatric side effects including anxiety, depression, irritability, or psychosis. The original warnings had been inherited from older weight-loss drugs, not based on GLP-1-specific evidence. European drug labels never carried these warnings in the first place.
The largest meta-analysis to date, published in JAMA Psychiatry in May 2025 by Dr. Aureliane Pierret and colleagues, pooled data from 80 randomized controlled trials encompassing 107,860 patients. GLP-1 treatment showed no increased risk of serious psychiatric adverse events (log risk ratio -0.02, statistically null) and no worsening of depressive symptoms. What the meta-analysis did find was modest improvement in mental health-related quality of life (effect size 0.15) and meaningful reductions in emotional eating behaviors.
A separate large-scale study in Nature Medicine by Wang et al., co-authored by Dr. Nora Volkow (director of the National Institute on Drug Abuse), examined 240,618 patients with obesity and found semaglutide associated with a 73% lower risk of incident suicidal ideation (HR 0.27) compared to non-GLP-1 obesity medications. The result replicated in nearly 1.6 million patients with type 2 diabetes.
A comprehensive analysis in Nature Mental Health by De Giorgi and colleagues reviewed 374 studies (278 pre-clinical, 96 clinical) across the entire neuropsychiatric landscape. Their assessment: the evidence on mood effects remains genuinely mixed, with beneficial, harmful, and null findings all present in the literature. But the weight of evidence tilted toward safety. A meta-analysis of 31 RCTs with 84,713 patients found no difference in adverse neuropsychiatric events over more than a year of follow-up.
| Study | Design | Sample Size | Key Finding |
|---|---|---|---|
| Taipale et al. (Lancet Psychiatry 2026) | National cohort, within-individual | 95,490 | Semaglutide: 42% lower worsening mental illness |
| Pierret et al. (JAMA Psychiatry 2025) | Meta-analysis of 80 RCTs | 107,860 | No increased psychiatric adverse events vs placebo |
| Wang et al. (Nature Medicine 2024) | Retrospective cohort | 240,618 | Semaglutide: 73% lower incident suicidal ideation |
| Shapiro et al. (BMJ 2025) | Active comparator cohort | 362,658 | No increased suicidality after confounding adjustment |
| FDA Review (2026) | Pooled clinical trial analysis | 107,910 | No increased psychiatric risk; warning removed |
The substance use findings deserve separate mention. The Swedish team previously published work in JAMA Psychiatry showing semaglutide and liraglutide were associated with reduced alcohol use disorder. The current study adds a 47% reduction in worsening substance use disorder to semaglutide's profile. Meanwhile, early clinical data cited by Dr. Lembke at Stanford found GLP-1 medications reduced opioid cravings by 40% in a small study, with users showing 40% lower opioid overdose rates and 50% lower alcohol intoxication rates in another. All of this is early-stage, but the pattern keeps repeating across different substances and different research teams.
What this actually means if you're on a GLP-1 medication
If you're currently taking semaglutide for diabetes or weight management, this research carries a practical message: there is no psychiatric reason to stop your medication. The accumulated evidence -- from randomized trials to large observational studies to regulatory review -- consistently shows that GLP-1 drugs are psychiatrically safe. The FDA's decision to remove the suicidal behavior warning in January 2026 was based on 91 trials with nearly 108,000 patients.
If you have pre-existing depression or anxiety and are considering a GLP-1 medication for diabetes, the Swedish data suggests semaglutide specifically may offer a secondary benefit -- though this should inform, not drive, prescribing decisions. As the study authors note, for people with both diabetes and depression or anxiety, semaglutide "might be useful" as a "dually effective therapeutic option."
The JAMA Psychiatry meta-analysis also found that GLP-1 treatment improved quality of life across multiple dimensions -- mental health, physical health, diabetes-related, and weight-related -- beyond what placebo achieved. Emotional eating and restrained eating behaviors also improved. For people whose depression intertwines with disordered eating patterns, this is relevant.
Several practical caveats, though. One systematic review in Diabetes, Obesity and Metabolism flagged pharmacovigilance signals suggesting possible increased psychiatric risk in people simultaneously taking antidepressants or benzodiazepines alongside GLP-1 drugs. The evidence is thin and needs confirmation, but it's worth mentioning to your prescriber if you're on psychiatric medications.
GLP-1 medications are also not addictive and don't trigger withdrawal in the pharmacological sense. But stopping them can lead to weight regain and potentially to a return of whatever mood improvements coincided with treatment. We don't yet have data on whether mental health benefits persist after discontinuation, or whether they depend on maintained weight loss, ongoing brain-receptor effects, or both.
If you notice mood changes -- positive or negative -- after starting a GLP-1 medication, document them and discuss with your doctor. You are, at this point, living inside an ongoing natural experiment that researchers are still trying to understand.
For more on the safety profile of semaglutide, including gastrointestinal and other side effects, see our guide to Ozempic safety and semaglutide side effects. For broader context on this medication class, our GLP-1 weight loss drugs safety guide covers what current evidence says about benefits and risks.
The experiments that haven't happened yet
The most important study on GLP-1 drugs and depression hasn't been conducted. No randomized controlled trial has tested semaglutide with depression or anxiety as the primary outcome in patients selected because of their psychiatric diagnosis. Every study we've discussed either looked at psychiatric outcomes as a secondary endpoint, or observed them retrospectively in populations primarily treated for metabolic conditions.
Prof. David Nutt, head of the Centre for Neuropsychopharmacology at Imperial College London, offered a measured prediction in response to the Swedish findings. While the insulin-related mechanism hypothesis "might seem plausible," he noted, "I think it's unlikely that using GLP-1R agonists alone as treatments for depression or anxiety will work." That's a realistic expectation. The history of psychiatric drug development is full of promising observational signals that evaporated in controlled trials.
Several specific knowledge gaps need filling. The Swedish registers contained no data on weight change, so we cannot separate semaglutide's possible direct brain effects from the well-documented mood benefits of significant weight loss. We have no interaction data between GLP-1 drugs and antidepressant medications. The cohort was entirely Swedish, raising questions about generalizability to more ethnically diverse populations and to healthcare systems where medication access depends on insurance coverage and cost.
The question of what happens after stopping is particularly urgent. Over 15 million Americans are now estimated to use GLP-1 medications. If some portion of them are experiencing incidental psychiatric benefits, what happens when drug shortages, insurance changes, or personal decisions lead them to discontinue? The Swedish data's sensitivity analyses -- removing the first 30 and 60 days from analysis periods -- suggest the effect isn't just a short-term honeymoon, but we have no long-term discontinuation data.
The fact that semaglutide outperformed other GLP-1 drugs points toward pharmacological specificity worth investigating. Semaglutide has greater weight-loss efficacy and superior glycaemic control compared to liraglutide, dulaglutide, and exenatide. It may also penetrate the central nervous system differently. Disentangling these factors requires head-to-head trials with brain imaging, not just outcome data from registries.
What we can say with growing confidence: GLP-1 drugs don't cause psychiatric harm, and semaglutide may do some measurable psychiatric good. Whether "may" becomes "does" depends entirely on trials that treat depression as the primary target rather than a secondary curiosity. The Taipale team's own conclusion -- that "randomised controlled trials evaluating these findings are warranted" -- was echoed by every expert who reviewed the paper. The signal is strong enough to pursue, and honest enough to remain uncertain about.
Frequently Asked Questions
Does semaglutide treat depression?
Not in any established sense. No randomized controlled trial has tested semaglutide as a depression treatment. The Swedish study found that people already taking semaglutide for diabetes experienced fewer psychiatric hospitalisations and sick days, but this is an observed association, not proof of a therapeutic effect. Multiple experts have cautioned against interpreting the data as evidence that semaglutide works as an antidepressant. If you have depression, continue working with your mental health provider on evidence-based treatments.
Should I ask my doctor about Ozempic for my anxiety or depression?
The current evidence does not support prescribing GLP-1 medications specifically for psychiatric conditions. If you have both diabetes (or obesity) and depression or anxiety, the Swedish data suggests semaglutide may offer secondary mental health benefits alongside metabolic ones, and that information could be useful in discussions about which diabetes medication to choose. But GLP-1 drugs are not approved for psychiatric use, and off-label prescribing for mental health alone would be premature given the current evidence.
Did the FDA find that GLP-1 drugs cause suicidal thoughts?
No -- the opposite. In January 2026, the FDA requested removal of the suicidal behavior warning from GLP-1 drug labels after reviewing 91 trials with nearly 108,000 patients. The review found no increased risk of suicidal thoughts, behavior, or other psychiatric side effects compared to placebo. The original warnings were based on concerns from older weight-loss drugs, not GLP-1-specific data.
Why did semaglutide show better results than other GLP-1 drugs?
Researchers aren't certain. Semaglutide produces greater weight loss and better glycaemic control than liraglutide, dulaglutide, and exenatide, and it may cross the blood-brain barrier more effectively. The differential results suggest this is not a simple class effect but reflects pharmacological differences between individual drugs. Further research involving brain imaging and direct comparison trials is needed to understand why semaglutide specifically shows stronger associations with mental health outcomes.
Are there risks to my mental health from taking GLP-1 drugs?
Based on current evidence, the psychiatric safety profile of GLP-1 drugs is reassuring. The largest meta-analysis (80 trials, 107,860 patients) found no increased risk of psychiatric adverse events versus placebo. One pharmacovigilance signal suggests monitoring may be warranted if you're simultaneously taking antidepressants or benzodiazepines, but this needs confirmation. As with any medication, report new mood changes to your prescriber.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.