Your brain burns through 20% of your body's energy. What if it's running on the wrong fuel?
The human brain consumes roughly 20% of your body's total energy at rest while accounting for just 2% of your body weight. Almost all of that energy comes from glucose, delivered through a tightly regulated supply chain that never fully shuts off, even while you sleep.
But glucose is not the brain's only fuel option. When carbohydrate intake drops low enough, the liver begins converting fatty acids into molecules called ketone bodies, primarily beta-hydroxybutyrate (BHB). These ketones cross the blood-brain barrier through monocarboxylate transporters and feed directly into the same energy-producing machinery that normally processes glucose. During prolonged fasting, ketones can supply nearly 60% of the brain's energy needs, effectively replacing glucose as the primary fuel source.
Think of it like a hybrid engine. Your brain normally runs on gasoline (glucose), but it has a second fuel system (ketones) that kicks in when the primary tank runs low. For most people, this backup system sits dormant. A ketogenic diet activates it on purpose.
The question driving a growing number of psychiatrists is whether some mental illnesses involve a brain that struggles to use glucose efficiently, and whether switching to that backup fuel system might help. The theory is not that glucose is bad. The theory is that certain brains may not metabolize it well, creating an energy deficit in neurons that contributes to psychiatric symptoms.
Dr. Shebani Sethi, a Stanford psychiatrist who is board-certified in both psychiatry and obesity medicine, describes the mechanism this way: "The ketogenic diet can provide ketones as an alternative fuel to glucose for a brain with energy dysfunction." The ketones don't just provide raw energy. BHB suppresses inflammatory pathways, reduces pro-inflammatory gene expression, and enhances antioxidant defenses in neural tissue. It also appears to shift the balance between GABA (the brain's primary inhibitory neurotransmitter) and glutamate (the primary excitatory one), potentially calming overactive neural circuits.
None of this is new chemistry. Neurologists have used ketogenic diets to treat epilepsy since 1921, when endocrinologist Russell Wilder discovered the diet could mimic the anti-seizure effects of fasting. More than a dozen randomized controlled trials have confirmed that ketogenic diets stabilize neuronal networks in epilepsy. The psychiatric application asks a logical next question: if the same diet that quiets seizures also changes how neurons fire, what happens when you give it to people whose neurons fire in patterns we call depression, mania, or psychosis?
A 21-person pilot study that moved the field from case reports to clinical data
For decades, the evidence that ketogenic diets might help psychiatric patients existed only as scattered case reports. A patient here, a patient there, each one dramatic but scientifically unpersuasive on its own. That changed in 2024 when Dr. Sethi published results from a pilot trial at Stanford that, while small, produced numbers striking enough to attract serious attention.
The trial enrolled 21 adults diagnosed with schizophrenia or bipolar disorder who were already taking antipsychotic medications and had at least one metabolic abnormality like insulin resistance or elevated triglycerides. For four months, participants followed a ketogenic diet with roughly 10% of calories from carbohydrates, 30% from protein, and 60% from fat. They received keto cookbooks and access to a health coach but were not told to count calories.
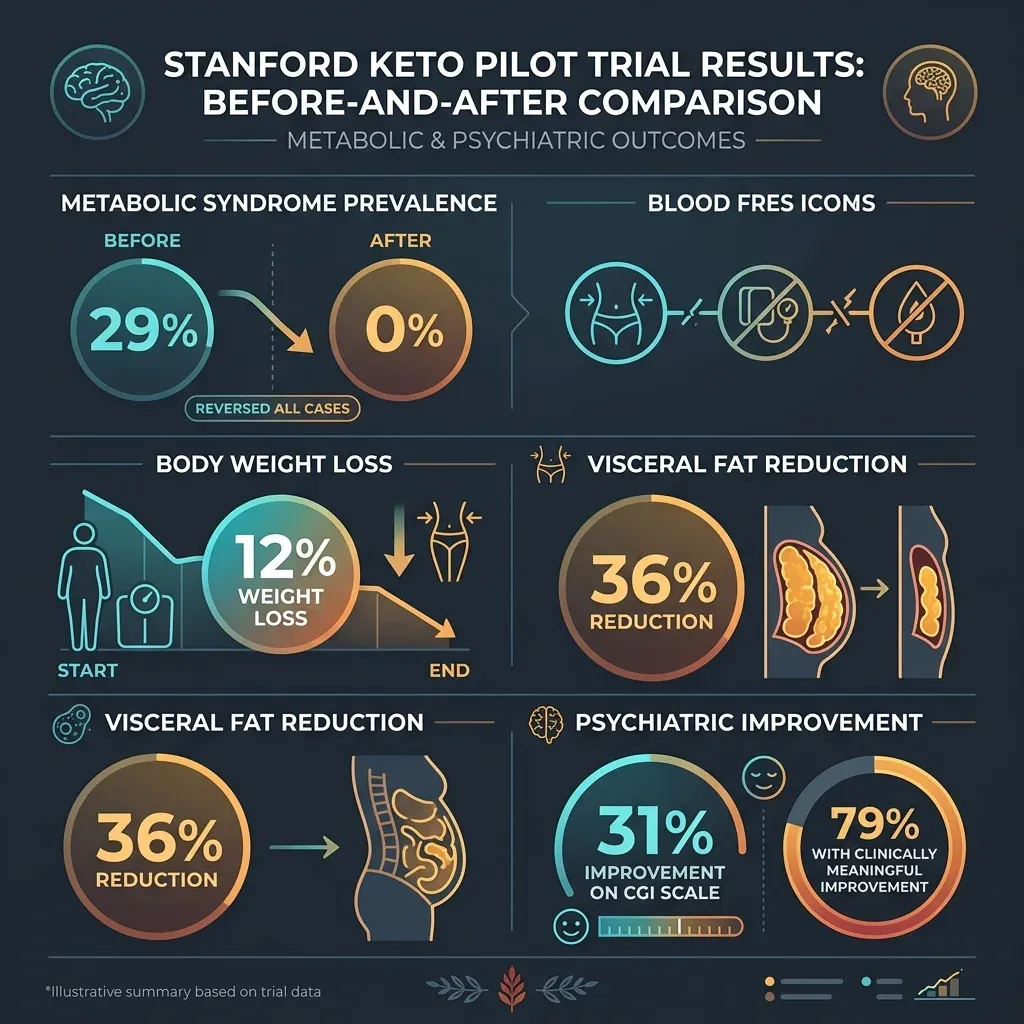
The metabolic numbers moved fast. Before the trial, 29% of participants met the criteria for metabolic syndrome. After four months, that number dropped to zero. Adherent participants lost an average of 12% of their body weight and 36% of their visceral adipose tissue. Insulin resistance, measured by HOMA-IR, fell 27%.
The psychiatric data was harder to dismiss. Participants improved an average of 31% on the Clinical Global Impressions scale, a standard psychiatrist rating of illness severity. Seventy-nine percent showed at least a one-point improvement on CGI, which represents clinically meaningful change. Among participants with schizophrenia specifically, scores on the Brief Psychiatric Rating Scale dropped 32%.
These participants were still on their antipsychotic medications. The diet was additive, not a replacement, and the combination appeared to produce benefits that neither approach had achieved on its own.
Sethi also observed what she described as a "potential dose-response relationship", with the fully adherent group showing more improvement than those who were semi-adherent. In pharmacology, dose-response relationships are a signal that something real is happening, not just placebo effects or natural fluctuation.
At Harvard, psychiatrist Dr. Christopher Palmer had arrived at similar conclusions through a different path. Palmer's interest began with his own health. Struggling with metabolic syndrome during his residency, he tried a ketogenic diet and noticed improvements not just in his blood work but in his mood, energy, concentration, and sleep. He began cautiously using the approach with treatment-resistant patients.
The case that Palmer describes as his turning point came in 2016. A patient with schizoaffective disorder whom Palmer had treated for eight years across 17 different medications, none of which stopped his hallucinations or delusions, tried a ketogenic diet and experienced what Palmer called "profound" psychiatric changes. Earlier, in a 2019 paper, Palmer had documented two cases of long-term schizophrenia remission on a ketogenic diet, including an 82-year-old woman who had been diagnosed at age 17 and achieved complete remission of psychotic symptoms after starting the diet in 2008.
A separate study reinforced the pattern from a different angle. Dr. Albert Danan, a psychiatrist in Toulouse, France, published a retrospective analysis of 31 inpatients with treatment-refractory mental illness who were placed on a ketogenic diet during hospitalization. The depression scores were particularly striking: Hamilton Depression Rating Scale scores fell from 25.4 to 7.7, a drop of nearly 70%. Among the ten patients with schizoaffective illness, PANSS scores dropped from 91.4 to 49.3.
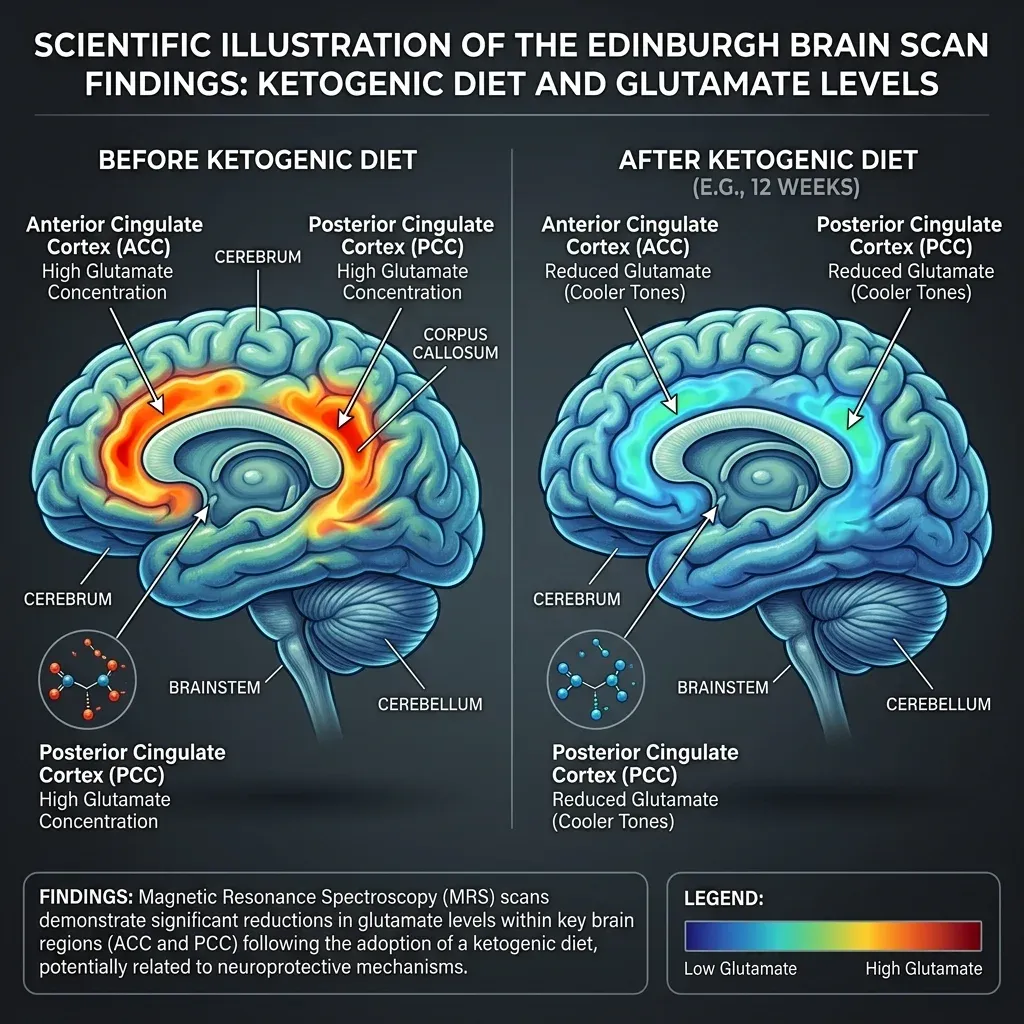
Edinburgh brain scans revealed something ketogenic diets actually change in bipolar patients
While the Stanford and Toulouse data showed that something was happening, a pilot study from the University of Edinburgh provided the first imaging evidence of what might be changing inside the brain. Dr. Iain Campbell, a psychiatrist who has bipolar disorder himself and manages it with a ketogenic diet, led the study.
Campbell's team recruited 27 euthymic individuals with bipolar disorder (meaning they were in a stable period between mood episodes) for a 6-to-8-week modified ketogenic diet. Unlike the Stanford trial, which studied acutely ill patients, Edinburgh deliberately selected stable patients to isolate the diet's effects from the confounding noise of active mood episodes. Twenty of the 26 who started the diet completed it.
The study used magnetic resonance spectroscopy (MRS) to measure brain metabolites before and after the intervention. The key finding: glutamate-plus-glutamine concentration (Glx) decreased by 11.6% in the anterior cingulate cortex and 13.6% in the posterior cingulate cortex. Both reductions were statistically significant. This matters because elevated glutamate is among the most consistent findings in brain imaging studies of bipolar disorder, and glutamate modulation is the proposed mechanism of action for several mood stabilizers already used in clinical practice.
The daily ecological momentary assessments told a complementary story. Among participants providing reliable daily data, higher ketone levels in the blood correlated with better mood (r=0.21, P<0.001) and higher energy (r=0.19, P<0.001). Ketone levels were inversely correlated with impulsivity (r=-0.30, P<0.001) and anxiety (r=-0.19, P<0.001). The impulsivity finding is particularly relevant to bipolar disorder, where impulsive behavior during manic or hypomanic episodes causes significant harm.
| Measure | Correlation with ketone levels | P-value |
|---|---|---|
| Mood | r = 0.21 (positive) | <0.001 |
| Energy | r = 0.19 (positive) | <0.001 |
| Impulsivity | r = -0.30 (inverse) | <0.001 |
| Anxiety | r = -0.19 (inverse) | <0.001 |
| Speed of thought | r = -0.08 (no correlation) | >0.05 |
The depression data tells a different story. A 2025 systematic review published in JAMA Network Open analyzed 50 studies involving 41,718 participants and found that across 10 randomized controlled trials, ketogenic diets were associated with a statistically significant reduction in depressive symptoms (SMD -0.48). The effect was modest but real, and it was stronger in studies that verified ketosis through blood ketone monitoring rather than relying on self-reported diet adherence.
But here is where the depression-anxiety split gets interesting. The same meta-analysis found that across 9 RCTs examining anxiety, there was no significant association (SMD -0.03). Ketogenic diets appear to help depression measurably, help bipolar symptoms across multiple domains, but may not do much for anxiety on its own. This differential response pattern matters for patient selection, which we will return to later.
Why the difference between bipolar and depression? Dr. Sethi has offered one framework: "Bipolar mania involves fluctuations in energy states in which neuronal firing is more unstable," she said, noting that both antipsychotic medications and ketogenic therapy can reduce that instability. Bipolar disorder may respond more robustly because it involves more overt neuronal excitability problems that ketones directly address through the GABA-glutamate mechanism. Depression likely involves a more complex mix of inflammation, neurotransmitter depletion, and neural circuit dysfunction, where ketones address some but not all pathways.
From fringe idea to funded specialty: the institutions backing metabolic psychiatry
Suggesting to a room of psychiatrists five years ago that diet could meaningfully affect schizophrenia would have ended the conversation. The institutional money now flowing into this research tells a different story.
Dr. Sethi coined the term "metabolic psychiatry" and founded the first metabolic psychiatry clinic at Stanford Medicine. At Harvard, Dr. Palmer directs research at McLean Hospital and published "Brain Energy" in November 2022, arguing that mental disorders are fundamentally metabolic disorders of the brain. The University of Edinburgh established the UKRI Hub for Metabolic Psychiatry.
The clearest sign came in February 2026, when the Wellcome Trust funded ENERGISE-BD, a £7.9 million Phase III randomized controlled trial. This is not a pilot. It is a full-scale clinical trial comparing a nutritional ketosis diet against standard NHS dietary guidelines for bipolar depression, co-led by the Universities of Edinburgh and Birmingham. Phase III trials are what regulatory agencies and clinical guidelines rely on. If ENERGISE-BD produces positive results, it would be the kind of evidence that changes treatment recommendations.
Stanford is also scaling up. Sethi is recruiting for a larger randomized controlled trial evaluating ketogenic therapy for schizophrenia, bipolar disorder, and depression. Additional studies of ketogenic approaches in Alzheimer's disease, ADHD, and anorexia nervosa are underway at other institutions.
These studies share one uncomfortable observation that psychiatry has mostly treated as coincidental: more than 40% of people with severe mental illness also have metabolic syndrome. The conventional explanation was that psychiatric medications cause weight gain and metabolic problems. That is partly true. But Palmer points to evidence that the metabolic-psychiatric overlap may run deeper. Observations dating back to the 1800s noted that diabetes and serious mental illness clustered in the same families, long before antipsychotic medications existed. If metabolic dysfunction is not just a side effect of treatment but a contributing cause of mental illness, then treating the metabolic dysfunction directly becomes a logical therapeutic target.
| Institution | Researcher | Study/Initiative | Status |
|---|---|---|---|
| Stanford Medicine | Dr. Shebani Sethi | Pilot trial (21 patients); larger RCT recruiting | Pilot published 2024; RCT ongoing |
| Harvard/McLean Hospital | Dr. Christopher Palmer | Brain Energy theory; clinical work | Book 2022; ongoing research |
| University of Edinburgh | Dr. Iain Campbell | Bipolar pilot (27 patients); ENERGISE-BD co-lead | Pilot published 2025; Phase III funded |
| University of Birmingham | Prof. Steven Marwaha | ENERGISE-BD co-lead | £7.9M Phase III funded Feb 2026 |
| Toulouse, France | Dr. Albert Danan | Retrospective analysis (31 inpatients) | Published 2022 |
What metabolic psychiatry lacks is the evidence required for standard-of-care status. Every researcher in the field acknowledges this openly. The pilot studies involve dozens of participants, not thousands. They lack control groups or use single-arm designs. Follow-up periods are measured in weeks or months, not years. The ENERGISE-BD trial and Sethi's expanding RCT are designed to fill exactly these gaps. The next two to three years will determine whether the promising signals from small studies replicate at scale.
The realistic patient profile: metabolic comorbidity, treatment resistance, and medical supervision
The research to date points toward a specific patient profile that is most likely to benefit, and an equally important list of people who should not attempt this without serious medical consideration.
The strongest evidence currently exists for people who fit this description: diagnosed with bipolar disorder or schizophrenia, taking antipsychotic medications, and experiencing metabolic side effects like weight gain, insulin resistance, or metabolic syndrome. This is the exact population studied in the Stanford pilot, and the results were most pronounced in this group. The Danan retrospective study adds evidence that treatment-refractory patients (those who have not responded adequately to conventional medications) may benefit substantially.
For depression specifically, the JAMA meta-analysis found that ketogenic diet benefits were stronger in nonobese participants, in studies using very low-carbohydrate interventions, and when ketosis was verified through blood monitoring rather than self-report. This suggests that the metabolic mechanism matters more than simple calorie restriction, and that actually achieving ketosis (not just eating fewer carbohydrates) is what drives the psychiatric effect.
The critical distinction that researchers emphasize: a ketogenic diet for mental health is a medical intervention, not a weight-loss fad diet. It requires physician oversight, nutritional guidance, and regular metabolic monitoring. Dr. Sethi frames it plainly: "The objective is not to replace conventional treatments with ketogenic therapy, but to use the diet as one powerful therapeutic metabolic tool among many."
Who should be cautious or avoid this approach entirely? The ketogenic diet is medically contraindicated for people with pyruvate carboxylase deficiency (a rare inborn metabolic error) and those with acute pancreatitis. Keto therapy can interact dangerously with certain antipsychotic medications, making unsupervised attempts potentially harmful. Without professional guidance, people risk reducing fiber and vitamin intake, increasing saturated fat consumption, and elevating cardiovascular risk. Some individuals experience elevated LDL cholesterol on ketogenic diets, though the Edinburgh study found no significant adverse changes in lipid profiles on average over their 6-to-8-week trial.
People with anxiety disorders alone may not be good candidates based on current evidence. The JAMA meta-analysis found no significant effect of ketogenic diets on anxiety across RCTs. And anyone who has heard claims that diet can "cure" serious mental illness should know that even the researchers producing the most optimistic data reject that framing. Dr. Palmer stated directly: "I have never claimed to have cured schizophrenia or any other mental disorder, and I certainly never use the word 'cure' in my work." Dr. Paul Appelbaum, a psychiatrist at Columbia University, put it more bluntly: "It is simply misleading to suggest that we know that ketogenic diets can improve the symptoms of schizophrenia, much less that they can cure the condition."
What supervised ketogenic therapy actually looks like
If you and your psychiatrist decide that a ketogenic approach is worth trying, here is what the clinical protocols from published studies actually involve. This is not the same as downloading a keto meal plan from Instagram.
The Stanford protocol used a macronutrient split of approximately 10% carbohydrates, 30% protein, and 60% fat, with an emphasis on whole, unprocessed foods including protein and non-starchy vegetables. The Edinburgh protocol was slightly more aggressive on fat: 60-75% of calories from fats, 5-7% from carbohydrates, with the remainder from protein and a preference for unsaturated fats.
Both studies provided significant professional support. Stanford participants received keto cookbooks, meal ideas, and access to a health coach. Edinburgh participants had weekly remote consultations with a dietitian, with additional contacts as needed. The Edinburgh team tracked a revealing number: the median time their study dietitian spent with each participant was 505 minutes, or roughly eight and a half hours over the study period. That level of support is not optional. It is what made adherence possible.
| Protocol Element | Stanford Trial | Edinburgh Trial |
|---|---|---|
| Carbohydrates | ~10% of calories | 5-7% of calories |
| Protein | ~30% of calories | Remainder after fat/carbs |
| Fat | ~60% of calories | 60-75% of calories |
| Duration | 4 months | 6-8 weeks |
| Monitoring | Weekly blood ketone levels | Daily glucose + ketone (KetoMojo device) |
| Support | Health coach + cookbooks | Weekly dietitian calls (median 505 min total) |
| Completion rate | 21 of 23 enrolled | 20 of 26 who started |

Monitoring is central to psychiatric ketogenic therapy. Both trials measured blood ketone levels regularly, not to count macros for their own sake, but because the psychiatric benefits appear to depend on actually achieving and maintaining ketosis. The Edinburgh study found that 91% of participants' readings tested positive for blood ketones, and the daily correlation data showed that the benefits tracked with ketone levels on a day-to-day basis. The JAMA meta-analysis confirmed this pattern, finding stronger effects in studies that used biochemical ketosis verification.
Adherence in the research setting has been better than many clinicians expected. In the Stanford trial, 14 of 21 participants were fully adherent, 6 were semi-adherent, and only 1 was non-adherent. In Edinburgh, 7 of the 20 completers requested to continue the ketogenic diet beyond the study period, opting out of the planned dietary cessation phase. The Danan inpatient study had the strictest control over adherence, with only 3 of 31 patients unable to adhere for more than 14 days.
The practical reality for someone considering this outside of a clinical trial: you need a psychiatrist who is willing to monitor the interaction between ketogenic therapy and your medications, a dietitian experienced with therapeutic (not weight-loss) ketogenic protocols, regular blood work including metabolic panels and lipid profiles, and a ketone monitoring device for home use. You should not stop or reduce psychiatric medications without direct physician guidance. The improvements seen in trials occurred with patients continuing their existing medications.

Frequently Asked Questions
Can a ketogenic diet replace psychiatric medications?
No. Every published study on ketogenic diets for mental health used the diet as an addition to existing psychiatric medications, not a replacement. Some individual patients in case reports have eventually reduced or discontinued medications under close physician supervision, but this is not the recommendation from any current research. Dr. Sethi describes the approach as using "the diet as one powerful therapeutic metabolic tool among many," not as a substitute for conventional treatment.
How quickly do psychiatric benefits appear on a ketogenic diet?
The Edinburgh study measured daily correlations between ketone levels and mood, finding real-time associations. Palmer's case report described noticeable changes within two weeks for one patient. However, the clinical trials ran for 6 weeks to 4 months before measuring outcomes, and the metabolic changes that likely drive psychiatric benefits need sustained ketosis to develop fully. Researchers caution against expecting rapid results.
Is this the same as the keto diet people use for weight loss?
The macronutrient ratios are similar, but therapeutic ketogenic protocols involve medical supervision, regular blood ketone monitoring, nutritional supplementation, and coordination with psychiatric medications that weight-loss keto diets do not. The Edinburgh trial participants received a median of 505 minutes of dietitian time. The distinction matters because the psychiatric benefits appear to depend on actually achieving and maintaining ketosis, which requires more precision than typical weight-loss approaches.
Does a ketogenic diet help with anxiety?
Current evidence suggests it may not. The JAMA meta-analysis found no significant effect on anxiety across 9 randomized controlled trials. The Edinburgh bipolar study did find a negative correlation between ketone levels and anxiety, but this was in participants with bipolar disorder, not anxiety disorders specifically. If your primary concern is anxiety without depression or bipolar disorder, the evidence does not currently support trying a ketogenic approach.
What are the biggest risks of trying a ketogenic diet for mental health without medical supervision?
The most serious risk is dangerous interactions between ketosis and certain psychiatric medications, particularly those that affect blood sugar or metabolic function. Without monitoring, people may also experience reduced fiber and vitamin intake, increased cardiovascular risk from excessive saturated fat, and elevated uric acid levels. Some individuals see elevated LDL cholesterol. Additionally, abruptly stopping psychiatric medications (which some people attempt when they feel better on the diet) can precipitate severe psychiatric crises, as documented in one of Palmer's case reports where a patient who stopped 14 medications experienced severe psychosis requiring hospitalization.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.