
Vyleesi: The 2019 Approval That Made PT-141 Legal Medicine
On 21 June 2019, the U.S. Food and Drug Administration approved bremelanotide under the brand name Vyleesi. Wikipedia, drawing on the FDA press release, records the date and the indication: acquired, generalized hypoactive sexual desire disorder in premenopausal women. The road there was long. Palatin Technologies licensed the parent compound melanotan-II, abandoned it in 2000, and synthesized bremelanotide as a metabolite. An intranasal version made it to Phase II in both female sexual dysfunction and male erectile dysfunction before the FDA halted the trials in 2007 over blood-pressure spikes.
In January 2017, AMAG Pharmaceuticals paid Palatin $60 million up front, plus up to $80 million in regulatory milestones and $300 million in sales milestones, for North American rights. AMAG took the subcutaneous autoinjector through Phase III. The agency classified Vyleesi as the second drug ever approved for HSDD, after Sprout Pharmaceuticals' flibanserin (Addyi) in 2015.
The FDA prescribing information caps Vyleesi at one 1.75 mg subcutaneous dose every 24 hours, no more than eight doses per month, injected at least 45 minutes before anticipated sexual activity. Post-marketing pregnancy registries and contraindications for uncontrolled hypertension and known cardiovascular disease are required. This is not a casual prescription. It sits closer to a controlled medication with serious dosing rails than to a wellness peptide.
Brain Chemistry, Not Blood Flow
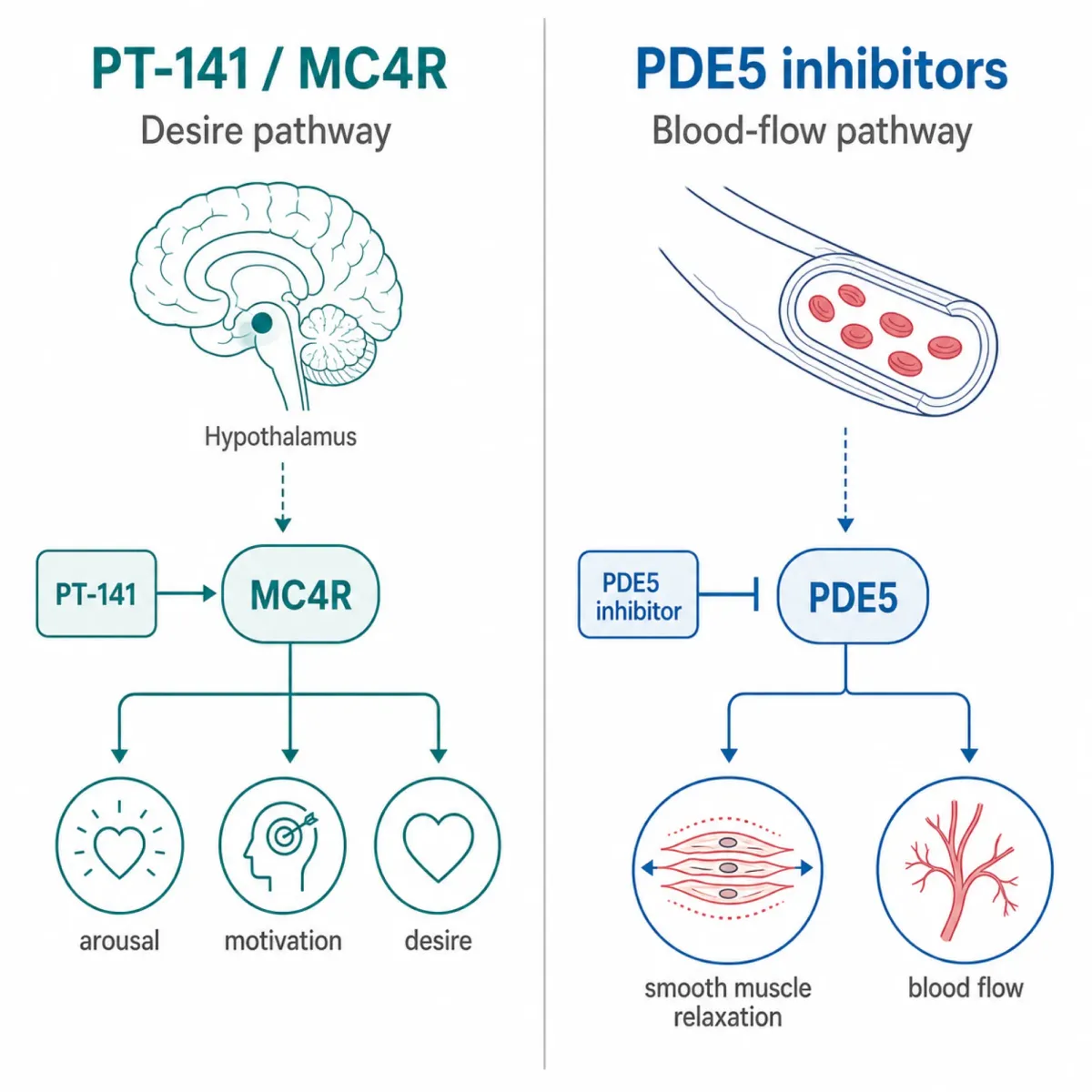
The single most important fact about PT-141 is what it doesn't do. It doesn't dilate blood vessels in the genitals. It doesn't inhibit phosphodiesterase 5. It doesn't change nitric oxide signaling. The mechanism review by Edinoff and colleagues in Neurology International (2022) frames bremelanotide as a synthetic analog of alpha-melanocyte-stimulating hormone that acts as a non-selective melanocortin receptor agonist with therapeutic activity primarily at the MC4 receptor. The site of action is the brain, specifically the medial preoptic area of the hypothalamus.
The downstream effect is dopaminergic. A crossover fMRI study of 31 premenopausal women with HSDD by Layla Thurston, Alexander N. Comninos, Waljit S. Dhillo and colleagues in the Journal of Clinical Investigation observed that MC4R agonism enhanced functional connectivity between the amygdala and insula while deactivating the secondary somatosensory cortex bilaterally during erotica viewing. The researchers interpreted this as the drug reducing self-monitoring while increasing sexual motor imagery. Self-reported desire rose significantly versus placebo for up to 24 hours after a single dose.
This is a genuine pharmacological category split. Pfaus, Sadiq, Spana and Clayton, writing in CNS Spectrums, argue the relevant subtype is MC4R, with downstream dopamine release in the mPOA, nucleus accumbens, VTA, and amygdala. Sildenafil and tadalafil work in the corpus cavernosum. They make blood vessels easier to dilate when arousal is already firing. They don't create arousal.
That difference is also why the side effects diverge. Sildenafil produces flushing and nasal congestion, both vascular. Bremelanotide produces nausea, a brainstem effect. The same pathway that switches on desire also irritates the area postrema.
HSDD: Real Diagnosis or Manufactured Disease?
Vyleesi only works if HSDD is a real condition. That premise is contested.
The American Psychiatric Association removed HSDD from the DSM-5 in 2013, replacing it for women with Female Sexual Interest/Arousal Disorder (FSIAD), a stricter diagnosis requiring at least three of six listed symptoms in 75% or more of sexual encounters over six months. The change reflected a sense that HSDD lumped together biological, psychological, and relational issues. The same Wikipedia entry notes that the UK's National Institute for Health and Care Excellence does not recognize HSDD as a medical disorder, citing Hypoactive sexual desire disorder: inventing a disease to sell low libido by Antonie Meixel, Elena Yanchar, and Adriane Fugh-Berman.
Stahl's review in The Journal of Clinical Psychiatry describes HSDD as the subject of debate, including the accusation that pharmaceutical companies engaged in disease mongering by inventing or exaggerating a disorder to sell expensive medications. Critics including Ray Moynihan, Leonore Tiefer, and Fugh-Berman argue drug firms funded the diagnostic instruments used to define HSDD severity, then pointed at those instruments as evidence of unmet need.
The "Even the Score" campaign that preceded both flibanserin and bremelanotide approvals reframed FDA caution as gender bias, claiming the agency had approved 26 drugs for male sexual dysfunction and none for women. The framing collapsed the distinction between drugs treating mechanical erection failure and drugs treating low desire. Glen I. Spielmans, in his 2021 re-analysis, calls this the "corporate appropriation of feminist language" and notes that no FDA-approved drug existed for male low desire either.
None of this means low desire is fake. Some women experience genuinely distressing low libido that's not explained by the usual confounders. The question is how big that subgroup is, and whether the trials enrolled the right women.
Inside the RECONNECT Trials: What 1,247 Women Reported
The approval rested on two identically designed Phase 3 trials called RECONNECT, registered as Studies 301 and 302. Edinoff and colleagues describe the trial as randomizing 1,247 premenopausal women with HSDD to 1.75 mg bremelanotide or placebo, taken as needed by autoinjector over 24 weeks. The co-primary endpoints were change in the Female Sexual Function Index desire domain (FSFI-D) and change in the Female Sexual Distress Scale Item 13 (FSDS-DAO).
The drug hit both co-primary endpoints. A ScienceDirect summary of the RECONNECT effect-size analysis pegs Cohen's d at 0.39 for improving sexual desire and 0.27 for decreasing related distress, both versus placebo. By FDA standards, statistically convincing enough for approval. By Cohen's original conventions, small-to-medium.
The trials missed on a different endpoint. Glen I. Spielmans, re-analyzing the trials using FDA New Drug Application data in The Journal of Sex Research, reports that the change from baseline in satisfying sexual events was 0.0 for bremelanotide versus -0.1 for placebo in Study 301, with no statistically significant difference between groups. Spielmans argues the sponsors moved satisfying sexual events from a co-primary measure to a secondary measure mid-trial, then leaned on the FSFI-D and FSDS-DAO scores as the success metrics.
The Spielmans paper is uncomfortable reading. He found that 72.72% of the protocol-listed outcomes were not reported in the primary journal publication by Kingsberg and colleagues, while 15 favorable secondary outcomes were introduced post-hoc without empirical justification. He calculated a relative risk of 9.95 for adverse-event-driven dropout on the drug versus placebo, with a number-needed-to-harm of 6. And he noted that more women in the placebo group elected to continue into the open-label extension phase than women in the active drug group, the kind of pattern that suggests participants were voting with their feet.
The official trial publication called the safety profile favorable and the side effects mild to moderate. Both characterizations can be true of the same data, depending on what you choose to report.
The Practical Picture: 45 Minutes, Nausea, and the 8-Dose Cap
The Vyleesi label is unusually candid about side effects. The FDA prescribing information lists nausea as the most common adverse reaction at 40% of patients, requiring anti-emetic therapy in 13%, and leading to premature discontinuation in 8%. Onset is roughly 30 minutes to one hour after injection, with a median duration around 2.4 hours. The label notes that nausea improves for most patients with the second dose, with first-dose incidence around 21% dropping to about 3% on subsequent doses. Adaptation is real; the first-dose experience is rough.
Cardiovascular effects are predictable but transient. Each dose produces maximal increases of 6 mmHg in systolic blood pressure and 3 mmHg in diastolic, peaking 2 to 4 hours post-dose, with a heart rate drop of up to 5 beats per minute, returning to baseline usually within 12 hours. The 24-hour and 8-doses-per-month rails exist because stacked doses produce additive BP effects. The label is contraindicated in uncontrolled hypertension and known cardiovascular disease.
The hyperpigmentation issue surprises most patients. In the Phase 3 trials, focal hyperpigmentation involving the face, gingiva, and breasts was reported in 1% of patients receiving up to 8 doses per month, but in a separate study, 38% of patients developed it after daily dosing for 8 days, with another 14% developing changes after another 8 days. Darker-skinned patients were more affected. Resolution after discontinuation was not confirmed in all patients. This is the mechanistic price of binding MC1R alongside MC4R; the same receptor family that drives sexual brain processing also drives melanin synthesis.
DailyMed records absolute bioavailability near 100% after subcutaneous injection, median Tmax of about 1 hour, and a mean terminal half-life of 2.7 hours. The 45-minute pre-activity window fits the Tmax. The LiverTox monograph at NCBI Bookshelf adds that bremelanotide slows gastric emptying, which decreases systemic exposure of orally administered naltrexone and can alter absorption of other concomitant oral medications.
Cost, Insurance, and the Compounded PT-141 Underground
The brand-name Vyleesi is expensive, and most insurance plans treat HSDD therapies as outside their formulary. Out-of-pocket pricing has been variable, with manufacturer copay programs and telehealth bundles at different price points. Our research base doesn't include verified retail-pricing data, but many patients facing the autoinjector list price walk away from the prescription.
The walkaway created the gray market. PT-141 is widely sold by online "research peptide" suppliers as unregulated powder, and a parallel ecosystem of compounding pharmacies and telehealth clinics offers compounded injectables. LIVV Natural's product page is typical: marketed for female libido, with disclaimers stating "All products on this site are for Research, Development use only. Products are Not for Human consumption of any kind". The same pages signal at human dosing elsewhere. It's the research-chemical-with-a-wink model the FDA has been chasing across peptides for years.
The GLP-1 compounding pharmacy boom normalized telehealth-prescribed compounded peptides, and bremelanotide rides the same channels. The same LIVV page is explicit that "LIVV Peptides is a chemical supplier. LIVV Peptides is not a compounding pharmacy or chemical compounding facility as defined under 503A of the Federal Food, Drug, and Cosmetic act". That's a regulatory firewall, not a quality claim. The product is not held to USP sterility standards, the dose is not verified, the supply chain is opaque.
The clinical risk is real. The 8-doses-per-month cap is a safety limit, set because daily dosing produced focal hyperpigmentation in 38% of patients in a controlled study. Compounded PT-141 sold without that framing tends to land in customers' hands without the same cautioning. The blood-pressure contraindication for uncontrolled hypertension still matters whether the prescription comes from a primary-care physician or a telehealth screening form.
The other thing the gray market hides is who PT-141 is for. The Vyleesi label is specific: acquired, generalized HSDD in premenopausal women. Off-label use slides into postmenopausal patients, women without HSDD, and male users (a separate audience covered in a companion piece). The data does not support those uses at the same level.
The Pink-Pill Backlash
The bremelanotide story sits inside a longer argument about whether the pharmaceutical industry should be in the female desire business at all.
The flibanserin precedent loomed over Vyleesi. Sprout Pharmaceuticals' Addyi was approved in 2015 after the FDA had rejected it twice, partly under pressure from the "Even the Score" campaign. Spielmans documents how the campaign's framing of FDA caution as gender bias produced political cover for the flibanserin and then the bremelanotide approval, despite modest effect sizes and tolerability issues. Researchers including Adriane Fugh-Berman and Judy Z. Segal have argued the campaign weaponized feminist language to advance a corporate agenda.
The skeptics are not anti-treatment. They are anti-overclaim. Stahl's review acknowledges that some women genuinely suffer from distressing low libido. The question is whether the trials enrolled those women or instead enrolled women whose low desire was better explained by partner-specific issues, depression, hormonal changes, or other common confounders. The DSM-5 removal of HSDD reflects exactly that uncertainty in psychiatry.
Independent epidemiology is messier than the Vyleesi marketing suggests. Generalized acquired HSDD with documented distress and no other explanation is rare. Distress about low desire that has a specific cause (a relationship issue, a medication, a thyroid problem, perimenopausal change) is common. The drug was approved for the first category, and is often marketed as if it fit the second.
Spielmans summarized it bluntly: bremelanotide produced "modest benefits on incompletely reported post-hoc measures of questionable validity," with an adverse-event-driven dropout pattern that suggested patients "substantially preferred placebo". The Kingsberg trial publication called the same data clinically meaningful. Both readings sit in the literature. PT-141 is a real centrally acting MC4R agonist that changes brain processing of erotic stimuli in fMRI and produces statistically significant gains on validated desire and distress scales. It also produces nausea in 40% of users and an 18% adverse-event dropout rate. The honest version of the conversation acknowledges all of that at once.
Frequently Asked Questions
Is PT-141 the same as Viagra for women?
No. Viagra (sildenafil) is a PDE5 inhibitor that acts on blood vessels to support an existing arousal response. Bremelanotide is a melanocortin-4 receptor agonist that acts in the hypothalamus and triggers dopamine release. The "female Viagra" framing is marketing shorthand, not pharmacology. The two drugs share neither target nor side-effect profile.
Who is FDA-approved to use Vyleesi?
Premenopausal women with acquired, generalized HSDD. "Acquired" means a normal desire baseline that declined; lifelong low desire is excluded. "Generalized" means the low desire isn't limited to one partner or one situation. Use is contraindicated in uncontrolled hypertension or known cardiovascular disease. Postmenopausal use, male use, and use in women without HSDD are off-label.
How well does it actually work in trials?
The Phase 3 RECONNECT trials showed statistically significant gains on the FSFI desire domain and the FSDS Item 13 distress measure, with Cohen's d effect sizes of 0.39 and 0.27. The drug did not show a statistically significant gain on satisfying sexual events versus placebo. That endpoint was moved from co-primary to secondary mid-trial, a target of methodological critique.
What does the side-effect experience look like?
Forty percent of trial patients experienced nausea, with median onset around 30 minutes and duration about 2.4 hours. Thirteen percent needed anti-emetic therapy; 8% dropped out specifically because of nausea. Twenty percent reported flushing, 11% headache, and about 1% developed focal skin darkening on the face, gums, or breasts. Each dose produces a transient blood-pressure rise of roughly 6 mmHg systolic and 3 mmHg diastolic for several hours. Discontinuation due to adverse events was 18% on bremelanotide versus 2% on placebo.
Why is compounded PT-141 different from Vyleesi?
Vyleesi is the FDA-approved 1.75 mg autoinjector with a verified manufacturing process, a labeled dose, and a defined indication. Compounded or research-grade PT-141 is bulk peptide reconstituted by the patient or a compounding pharmacy. Quality, sterility, dose accuracy, and supply chain are not held to the same standards. The dosing rails and cardiovascular contraindications still apply, but the gray-market path tends to skip them.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











