Why ADHD Brains Look for Alternatives to Stimulants
A significant number of patients with ADHD either fail to respond to stimulant medications or experience side effects that preclude their use. That single sentence, buried in a 2007 paper in Medical Hypotheses, captures why an underground market for cognitive peptides exists in the first place. When the drugs that are supposed to help you concentrate instead give you insomnia, appetite loss, heart palpitations, or a personality your friends barely recognize, the search for alternatives begins.
ADHD medications work primarily by increasing dopamine and norepinephrine activity in the prefrontal cortex. Think of these neurotransmitters as volume knobs for attention and impulse control. Stimulants crank them up. For many people, that works well enough. But the blunt-force approach comes with real costs, and some brains simply do not respond the way the textbooks predict.
Then came the Adderall shortage. Starting in late 2022 and stretching into 2024, patients with legitimate ADHD prescriptions found themselves unable to fill them. Clinics that had never mentioned peptides began discussing Semax as a potential bridge during the shortage. That crisis accelerated a trend that had been building quietly in biohacker forums for years: what if there were molecules that modulated the same attention-relevant brain systems without the DEA scheduling, the pharmacy lines, or the cardiovascular strain?
The answer to that question is not simple, and anyone telling you otherwise is selling something. But the question itself is worth examining, because the neuroscience behind it reveals real mechanisms that pharmaceutical companies have largely ignored.
How Peptides Interact With Dopamine and Norepinephrine Pathways
To understand why certain peptides interest ADHD researchers, you need to understand what ADHD actually is at the neurochemical level. ADHD is characterized as a neurodevelopmental disorder with disturbances in dopamine and brain-derived neurotrophic factor (BDNF) function. Those two systems are the relevant targets.
Semax, the peptide generating the most ADHD-related discussion, is a synthetic heptapeptide derived from adrenocorticotropic hormone (ACTH). The critical detail: it retains the neurotrophic effects of ACTH while being completely devoid of hormonal activity. Imagine stripping a car engine down to just the fuel injection system without the exhaust, the transmission, or the brakes. You get a narrower set of effects but lose the safety systems too.
The mechanism researchers find interesting is twofold. First, Semax can augment the effects of psychostimulants on central dopamine release. It does not simply flood the brain with dopamine the way amphetamines do. Instead, it appears to modulate how the dopamine system responds to other inputs. Second, it stimulates central BDNF synthesis, which promotes the formation of new neural connections. BDNF functions as fertilizer for neurons. Low BDNF has been linked to ADHD, depression, and cognitive decline.
Here is where the story gets more nuanced. According to the Alzheimer's Drug Discovery Foundation's research review, intranasal Semax increased serotonin but not dopamine levels directly. However, it potentiated the stimulatory effects of d-amphetamine. That distinction matters enormously. Semax is not a dopamine booster on its own. It may instead work as an amplifier of whatever dopamine activity is already present, whether from natural brain function or from prescription stimulants.
Selank, the other peptide that shows up in ADHD conversations, operates through an entirely different mechanism. Research published in Frontiers in Pharmacology found that Selank affects the expression of genes involved in GABAergic neurotransmission. GABA is the brain's primary inhibitory neurotransmitter, the one responsible for calming neural activity. If dopamine and norepinephrine are the gas pedals, GABA is the brake. For someone with ADHD who also deals with anxiety (a common comorbidity), a peptide that helps regulate the braking system while something else handles the acceleration is an appealing idea.
Key distinction: Semax appears to modulate dopamine indirectly (amplifying existing activity, not generating new activity). Selank works primarily through the GABA system. Neither works the way Adderall or Ritalin does.
Selank and Semax: What the ADHD-Specific Research Actually Shows
Semax was developed at the Russian Academy of Sciences and has been used clinically in Russia for stroke recovery, dyscirculatory encephalopathy, Parkinson's disease, optic nerve atrophy, and even in newborns with neurological deficits. That clinical history is real, documented, and spans decades. It is not a supplement-company invention.
But here is the catch that every productivity guru glosses over: there are few published English-language studies in humans. The bulk of the clinical data exists in Russian-language journals that most Western researchers cannot access or evaluate.
What does the accessible research show? In one pilot study of 24 healthy subjects, intranasal 1% Semax solution (total dose 1.2 mg) increased resting fMRI signal in the default mode network relative to placebo. That is a real finding from a controlled study, published by Lebedeva and colleagues in 2018. A separate study reported that Semax at doses of 250-1000 mcg/kg improved attention and short-term memory with EEG changes resembling those seen with established neuroprotective drugs.
In stroke patients, the data is somewhat stronger. A study of 110 stroke patients found that Semax treatment (two courses of 6,000 mcg/day for 10 days with a 20-day interval) increased plasma BDNF levels, and patients with higher BDNF showed improved rehabilitation timing.
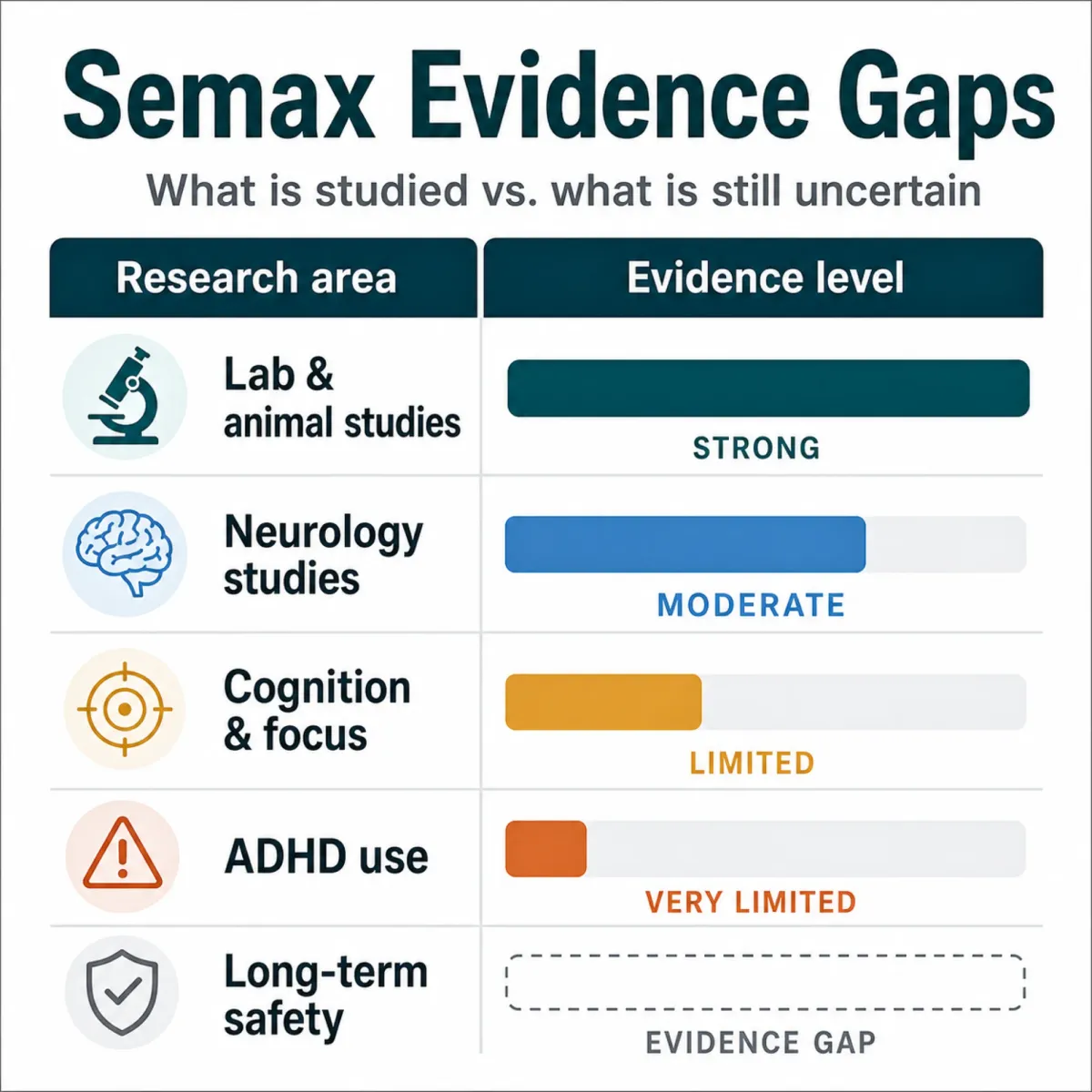
For ADHD specifically, the evidence is a single hypothesis paper. Published in Medical Hypotheses in 2007, it proposed that Semax may have good therapeutic potential in ADHD based on its dopamine-modulating and BDNF-stimulating properties. A hypothesis paper is an argument for why a study should be conducted. It is not evidence that the treatment works. That distinction is the single most important thing anyone considering peptides for ADHD needs to understand.
Nobody has run that study. There is no randomized controlled trial of Semax in ADHD patients. Not in Russia, not anywhere else. The proposed mechanism is plausible. The animal data is encouraging. The human ADHD data does not exist.
| Peptide | Primary Mechanism | Human ADHD Trials | Regulatory Status |
|---|---|---|---|
| Semax | BDNF upregulation, dopamine modulation | None (1 hypothesis paper only) | Rx in Russia; not FDA approved |
| Selank | GABAergic gene expression, anxiolytic | None | Rx in Russia; not FDA approved |
| Dihexa | HGF/c-Met pathway, synaptogenesis | None | Research chemical only |
| Noopept | AMPA receptor modulation, NGF/BDNF | None for ADHD | Rx in Russia; not FDA approved |
The Productivity Guru Stack: What People Are Actually Taking
Spend an hour on r/Biohackers or r/Nootropics and you will find elaborate peptide protocols that read like chemistry homework. The most common ADHD-adjacent stack that surfaces across multiple Reddit threads combines Semax and Selank intranasally, often layered on top of existing stimulant prescriptions.
The logic, at least in theory, is not random. Semax for the dopamine/BDNF angle, Selank for the anxiety-calming GABA angle. Together, the idea is a smoother version of what stimulants deliver alone: focus without the jitters, clarity without the crash.
One user who tracked their cognition for eight months on Semax reported working memory improvements of approximately 18% from baseline by week 10, with reaction time dropping roughly 40 milliseconds on average. They used a 5-days-on, 2-days-off protocol and described subjective focus as "the most noticeable thing, particularly in the first 2-3 hours after dosing." That is a single person's self-report. It is interesting, but it proves nothing about whether Semax works for ADHD in general.
The more aggressive stacks go further. One user combining Dihexa, Alpha GPC, and Vyvanse described "10-12 hours of insane clear productivity" and recommended adding Semax nasal sprays at the four-hour mark as a booster. Another user on the same thread gave a sharply different assessment, noting that "Semax enhances the more autonomic effects of stimulants but not the executive function benefits. Anxiety, HR, that sort of thing."

The community is not monolithic. Users disagree about whether Semax crosses the blood-brain barrier effectively via intranasal delivery and whether subcutaneous injection produces meaningfully different results. Users with diagnosed ADHD already on Vyvanse or Adderall report that Selank helps most by reducing stimulant-induced anxiety rather than adding cognitive benefits. A more modest claim than peptide clinic marketing, and probably closer to reality.
| Stack Component | Reported Role | Community Consensus |
|---|---|---|
| Semax (intranasal) | Focus, BDNF, dopamine modulation | Mixed: some report clear effects, others notice nothing |
| Selank (intranasal) | Anxiety reduction, calming | More consistent reports of reduced jitteriness |
| Dihexa (oral) | Synaptogenesis, memory | Controversial: potent in animal models, minimal human data |
| Alpha GPC | Choline supply for acetylcholine | Widely used, modest evidence for cognition |
| Noopept | AMPA modulation, NGF | Caution: may risk stimulant neurotoxicity |
Peptides vs. Adderall, Ritalin, and Vyvanse: An Honest Comparison
Adderall, Ritalin, and Vyvanse have decades of randomized controlled trials, well-characterized side effect profiles, dose-response curves established across diverse populations, and regulatory oversight. When your doctor prescribes Vyvanse, both of you know what you are working with.
Peptides have none of that. As Dr. Eric Topol wrote in his review of the peptide trend, there is no evidence from randomized trials in humans that any of the non-FDA-approved peptides provide the benefits that are advocated. Topol, a cardiologist and researcher at Scripps Research, noted that non-approved peptides are being sold under the rubric of "research chemicals" to bypass FDA review.
Bottom line: Stimulant medications for ADHD have extensive Level 1 evidence. Peptides for ADHD have zero. Presenting them as equivalent choices is dishonest.
That said, stimulants carry real downsides: appetite suppression, insomnia, increased heart rate, potential for dependence, and personality-flattening effects that some patients find intolerable. Peptides appear to have a milder side effect profile based on available data, though the data is thin. The most common reported adverse effects of Semax in clinical use are nasal cavity discoloration in approximately 10% of patients and increased blood glucose in about 7.4% of diabetic patients.
| Factor | FDA-Approved Stimulants | Cognitive Peptides (Semax/Selank) |
|---|---|---|
| Human RCTs | Hundreds | Zero for ADHD indication |
| FDA approval | Yes, multiple formulations | No (Rx in Russia only) |
| Mechanism clarity | Well-characterized | Partially understood |
| Side effect data | Extensive, population-level | Limited, mostly from Russian literature |
| Abuse potential | Schedule II controlled substance | Not scheduled (not studied for abuse liability) |
| Insurance coverage | Typically covered | No coverage; cash pay only |
| Prescriber availability | Any psychiatrist/PCP | Specialty peptide clinics only |
Risks, Legal Gray Zones, and What Your Doctor Won't Prescribe
The FDA has identified certain bulk drug substances used in compounding that may present significant safety risks. Compounding pharmacies are where most Americans access peptides. Unlike FDA-approved medications manufactured under strict quality controls, compounded peptides have variable purity, potency, and sterility depending on the pharmacy.
Health Canada has issued warnings telling consumers to "think twice before injecting peptides bought online", noting that unauthorized products can seriously harm health. The AP News investigation into peptide injection risks documented cases of contaminated products, inconsistent dosing, and adverse reactions that went unreported because the products exist outside normal pharmacovigilance systems.
The legal status of cognitive peptides in the United States occupies genuine gray territory. Semax and Selank are not FDA-approved drugs. They are not scheduled controlled substances. They exist in a regulatory limbo where they can be purchased as "research chemicals" but cannot legally be marketed for human consumption with therapeutic claims. Peptide companies exploit this ambiguity by selling products labeled "for research purposes only" while their marketing materials clearly target human use.
Your psychiatrist almost certainly will not prescribe these peptides, not from hostility but from practical barriers: no FDA-approved version exists, no established dosing guidelines for ADHD, no way to bill insurance, and no malpractice protection if something goes wrong. Specialty peptide clinics fill this gap, but they profit from prescribing these compounds and operate with minimal oversight.
The Gap Between Reddit Anecdotes and Clinical Evidence
The biohacker community has generated more data on peptides for focus than any research institution. User reports on Reddit include tracked metrics, detailed protocols, and comparative notes across sources. Some of this is genuinely thoughtful, like the user who tracked eight months of cognitive metrics on Semax with baseline comparisons.
But self-experimentation cannot replace controlled research. No one in these threads uses placebo controls or blinding. No one accounts for confounders like sleep, exercise, stress, and diet that drift over months. As one commenter on that thread noted: "most of the substantive Semax research comes from a pretty narrow set of Russian institutions, which doesn't invalidate it, but it does mean independent replication is thin."
Science News has characterized the broader peptide trend as "unproven" health products gaining increased access. The Guardian found that the peptide wellness market has grown rapidly with minimal scientific substantiation for many claimed benefits. The research that would actually settle the question, a double-blind trial of Semax in adults with diagnosed ADHD, does not exist. The pharmaceutical industry has little incentive to fund it (not patentable). Academic researchers face difficulty because the compounds lack FDA approval. And much of the Russian literature remains inaccessible in English.

Where does that leave someone with ADHD who is curious about peptides? In a position that demands more honesty than most wellness content provides. The mechanisms are plausible. The animal data is real. The community experience is not uniformly positive, which is actually a reassuring sign (universally glowing anecdotes usually indicate strong placebo effects or suppressed negative reports). But plausible is not proven. Pilot studies with 24 participants do not constitute clinical evidence.
If your current ADHD treatment is not working, the responsible first steps remain: work with your prescriber on dose adjustments, try different stimulant formulations, explore approved non-stimulant options like atomoxetine or guanfacine, and address lifestyle factors. If after exhausting those options you choose to explore peptides, do so with a physician's involvement, from a reputable compounding pharmacy, and with full awareness that you are making an informed gamble rather than following established medical guidance.
Frequently Asked Questions
Are peptides like Semax FDA-approved for treating ADHD?
No. Semax is not FDA-approved for any indication in the United States. It is approved as a prescription medication in Russia for neurological conditions including stroke recovery, but it has never undergone FDA review for ADHD or any other use. There are no randomized controlled trials of Semax for ADHD in any country.
Can you take Semax or Selank alongside Adderall or Vyvanse?
There are no formal drug interaction studies between these peptides and stimulant medications. Community reports suggest that some users combine them without acute adverse effects, while others report increased autonomic stimulation (elevated heart rate, anxiety) when stacking Semax with stimulants. Without clinical data, the safety of this combination is unknown. Anyone considering it should discuss it with their prescribing physician.
What is the difference between Semax and Selank for focus?
Semax primarily modulates dopamine pathways and stimulates BDNF production, targeting focus and cognitive performance. Selank primarily affects GABAergic neurotransmission, producing anxiolytic (anti-anxiety) effects. Users commonly report that Semax is "more for focus and cognition" while Selank is "more of a calming, less anxiety kind of thing." They operate through different mechanisms and are sometimes combined.
Where do people get cognitive peptides in the US?
Most Americans access these peptides through specialty compounding pharmacies (often associated with peptide therapy clinics), online "research chemical" vendors, or gray-market importation. Quality and purity vary significantly between sources. The FDA has raised concerns about safety risks associated with certain bulk drug substances used in compounding.
Is there any evidence that peptides work better than approved ADHD medications?
No comparative evidence exists. No randomized trials in humans have demonstrated that non-FDA-approved peptides provide the benefits advocated for any indication, including ADHD. FDA-approved stimulant and non-stimulant medications have extensive clinical trial data supporting their efficacy. The evidence bases are not comparable.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.