What 17 Million Americans Are Still Living With
Picture a software engineer in her late thirties who used to run sprint planning, juggle three Slack channels, and remember the names of every junior on her team. Six months after a moderate COVID infection, she can barely follow a conversation. Her boss is patient. Her brain is not cooperating with anyone.
She is a composite, but the population she represents is not. CDC data from March 2024, cited by Yale Medicine, put the number of U.S. adults reporting Long COVID at roughly 7% — about 17 million people. Stanford's 2025 long-COVID symposium called out the same figure, with internist Lauren Grossman, MD, adding that two million of those are out of work. A narrative review in the Journal of Alzheimer's Disease Reports reported that 17 to 28 percent of long-COVID patients have prolonged cognitive dysfunction, with deficits clustered in working memory, attention shifting, and processing speed.
A 297-person Brazilian cohort followed for at least three years after infection found that cognitive deficits persisted across attention, memory, and executive function, with severity tracking how sick someone had been at the start. Yale's Lindsay McAlpine, MD, who runs the school's NeuroCovid Clinic, described it bluntly: people who could once multitask "can do only one thing at a time."
The medical system, even five years in, has admitted what most patients already know. Stanford's Grossman put it this way: "There's no confirmatory test, no single fix, and no specialty that fully owns this condition." Into that vacuum, online clinics have arrived with a new offer: a four-peptide stack, a thirty-day course, and the suggestion that the fog can lift.
The mechanism story behind that promise is real. The proof that the stack works specifically for long-COVID brain fog is not. Both matter to anyone considering paying for a vial.
Why a Peptide Stack Makes Sense on Paper
To understand why the peptide pitch sounds plausible, you have to understand what is happening in the brain during long COVID. The honest summary is that the brain is inflamed, the gatekeepers between blood and brain are leaking, and the molecules the brain uses to repair itself are running low.
A 2025 review by Akiko Iwasaki's lab at Yale, published in Psychiatry and Clinical Neurosciences, laid out four mechanistic theories: direct viral invasion (rare), persistent inflammation, viral antigen reservoirs, and autoimmunity. The clearest signal in the data sits in the second category. Long-COVID patients show elevated plasma IL-1β, IL-6, and TNFα 8 to 10 months after infection, with autopsy studies showing brain-wide CD8+ T-cell infiltration in severe cases. A separate 2024 review in International Journal of Molecular Sciences connected this state to reduced levels of brain-derived neurotrophic factor (BDNF) and microglial activation patterns that share features with neurodegenerative disease.
Then there is the blood-brain barrier itself. A 2024 Nature Neuroscience study, summarized for clinicians by Yale, used dynamic contrast MRI to show that the protective barrier was leaking in temporal lobes and frontal cortex — not subtly, but measurably, and the leaks persisted for up to a year. A separate Nature paper that year found that SARS-CoV-2 spike protein binds to fibrin to form abnormal clots that activate microglia, sustaining inflammation long after the virus is gone.
This is where the peptide story gets traction. Selank, marketed for stress-driven cognitive complaints, modulates GABA receptors and shifts noradrenaline, dopamine, and serotonin levels. Semax, an analog of a fragment of the adrenocorticotropic hormone, is claimed to support BDNF and learning. Cerebrolysin is a porcine brain-derived peptide preparation that has been used in stroke and dementia trials abroad. BPC-157 is marketed for the gut-brain axis and inflammation. Each peptide's claimed mechanism touches a part of the long-COVID picture: BDNF deficit, GABA dysregulation, neuroinflammation, gut-brain crosstalk.
The honest read on this: the lock fits the key. That is not the same as the key opening the door. Mechanism plausibility is the first hurdle a treatment has to clear, not the last. For long-COVID brain fog specifically, the published clinical evidence for any peptide in this stack is best described as absent.
The Four Peptides Clinics Are Selling

A scan of clinic websites in 2026 shows a recurring cast. Klearmind's brain-fog page, for example, names five peptides as the standard "stack": Semax, Selank, Cerebrolysin, BPC-157, and the more experimental Dihexa. Variants combine Semax with Selank "for focus and calm clarity," BPC-157 with Semax "for inflammation and performance," and Selank with Cerebrolysin "for stress and recovery." None of these combinations have been tested in a randomized trial for long-COVID brain fog. Each has its own backstory.
Selank (also called TP-7) was developed in Russia at the Institute of Molecular Genetics as an analog of tuftsin, an immune-system peptide. As Innerbody Research summarized in early 2026, its anxiolytic action is GABAergic — meaning it modulates the same receptors benzodiazepines target — but does so without the dependence and amnesia that make Valium and its cousins so problematic. A 2020 functional MRI study in Doklady Biological Sciences tested Selank and Semax in 52 healthy participants and reported real, measurable changes in connectivity between the right amygdala and right temporal cortex. That is one of the cleanest pieces of human evidence in the entire stack — and it shows brain-effect, not clinical-effect.
Semax is the heptapeptide Met-Glu-His-Phe-Pro-Gly-Pro, a hybrid of an ACTH(4–7) fragment with a stabilizing tripeptide. It sits on Russia's official list of "Vital and Essential Drugs," used there for stroke recovery and cognitive complaints. A 2025 paper in Acta Naturae tested Semax intranasally at 50 micrograms per kilogram in transgenic mice modeling Alzheimer's. The animals improved on novel-object recognition and Barnes-maze tasks and showed reduced amyloid plaques in cortex and hippocampus. The same paper notes a "preliminary trial of Semax in a limited cohort of AD patients" with potential — and the authors immediately add that "more detailed investigation" is needed before broader use.
Cerebrolysin is not a single peptide but a porcine brain-derived preparation containing thousands of low-molecular-weight peptides. The manufacturer, Ever Pharma, posted a piece in November 2020 hypothesizing that the drug "could be effective in CIACI prevention" — cognitive impairment after critical illness. That was a hypothesis written when worldwide deaths first crossed 1.4 million. Five and a half years later, no major published RCT has tested Cerebrolysin specifically for long-COVID brain fog. It remains unapproved by the FDA in the United States.
BPC-157 is the most contested entry on the list. It does not appear in any RCT for long-COVID cognitive symptoms, and its place in the cognitive-stack pitch rests entirely on the gut-brain-axis argument: that calming systemic inflammation might reduce brain inflammation downstream. The FDA has placed BPC-157 in Category 2 of bulk drug substances with a flag for immunogenicity risk and the comment that the agency "lacks sufficient information to know whether the drug would cause harm when administered to humans."
Dihexa, when it is mentioned, is the disclaimer-laden footnote. The FDA's plain-language verdict on it: "FDA has not identified any human exposure data on drug products containing dihexa acetate administered via any route of administration." Vendors call it advanced. Regulators call it unstudied in humans, period.
The practical takeaway for anyone reading a clinic's stack pitch: ask which of the four peptides has been tested in a randomized controlled trial for long-COVID brain fog. The answer in mid-2026 is none of them. That fact should be on the table before any vial is opened.
The "30 Days" Claim, Pressure-Tested
The "30 days" framing is the heart of the marketing — and the part most likely to confuse new patients. Where does the timeline come from, and what does the actual data say should happen in that window?
Innerbody Research, summarizing what peptide-prescribing clinicians describe as a typical Selank course, lays out a vendor-claimed timeline: subjective improvement in mental clarity within 1 to 2 weeks, sharper learning and recall at 4 to 6 weeks, and full long-term cognitive and mood-stabilizing effects between 8 and 12 weeks. Day thirty falls inside the cognitive-effect window. That is convenient for a 30-day product pitch.
Now the trial data. The largest test of any cognitive intervention for long COVID brain fog ran for ten weeks, used five arms with active comparators, and was published in JAMA Neurology on November 10, 2025. RECOVER-NEURO enrolled 328 adults at 22 U.S. sites between August 2023 and December 2024. Patients were randomized to BrainHQ alone, BrainHQ plus a virtual cognitive rehab program (PASC-CoRE), BrainHQ plus active brain stimulation (tDCS), unstructured online puzzles, or BrainHQ plus a sham tDCS device. All five arms showed modest improvement. None outperformed the comparison groups.
Lead investigator David Knopman, MD, of the Mayo Clinic, was direct: "None of our rehabilitation approaches to treatment for cognitive Long COVID proved to be effective."
The most important detail for the 30-day claim is what happened to subgroups. Coverage of the trial in The Psychiatrist's Newsletter highlighted a finding that gets buried in most clinic marketing: "the length of time someone had been living with long COVID mattered more than the treatment they received." People with more recent infections improved the most, regardless of which arm they were in. Those further out from infection improved less.
That detail does damage to the "I tried these and the fog lifted in 30 days" anecdote. If you started a peptide stack three or four months after a moderate COVID infection — when most patients begin chasing answers — you are still inside the natural-recovery window Yale describes, where many people improve over six to nine months on their own. Improvement at week four cannot be distinguished, without a control arm, from improvement that would have happened anyway.
A small Bulgarian observational study illustrates the same trap. Twenty-three patients with cortical atrophy were prescribed Citicoline, Piracetam, or Memantine; all groups improved at three months. The authors' own caveat: "limited data," no comparator.
What this means practically: a 30-day improvement on a peptide stack is not evidence the stack worked. It is consistent with the stack working, with placebo response, with regression to the mean, and with the body healing on its own schedule. A controlled trial would tell us which. None has been run.
What RECOVER and the NIH Actually Say
The most telling thing about peptides in the long-COVID treatment landscape is what the largest publicly funded long-COVID research program does not say about them.
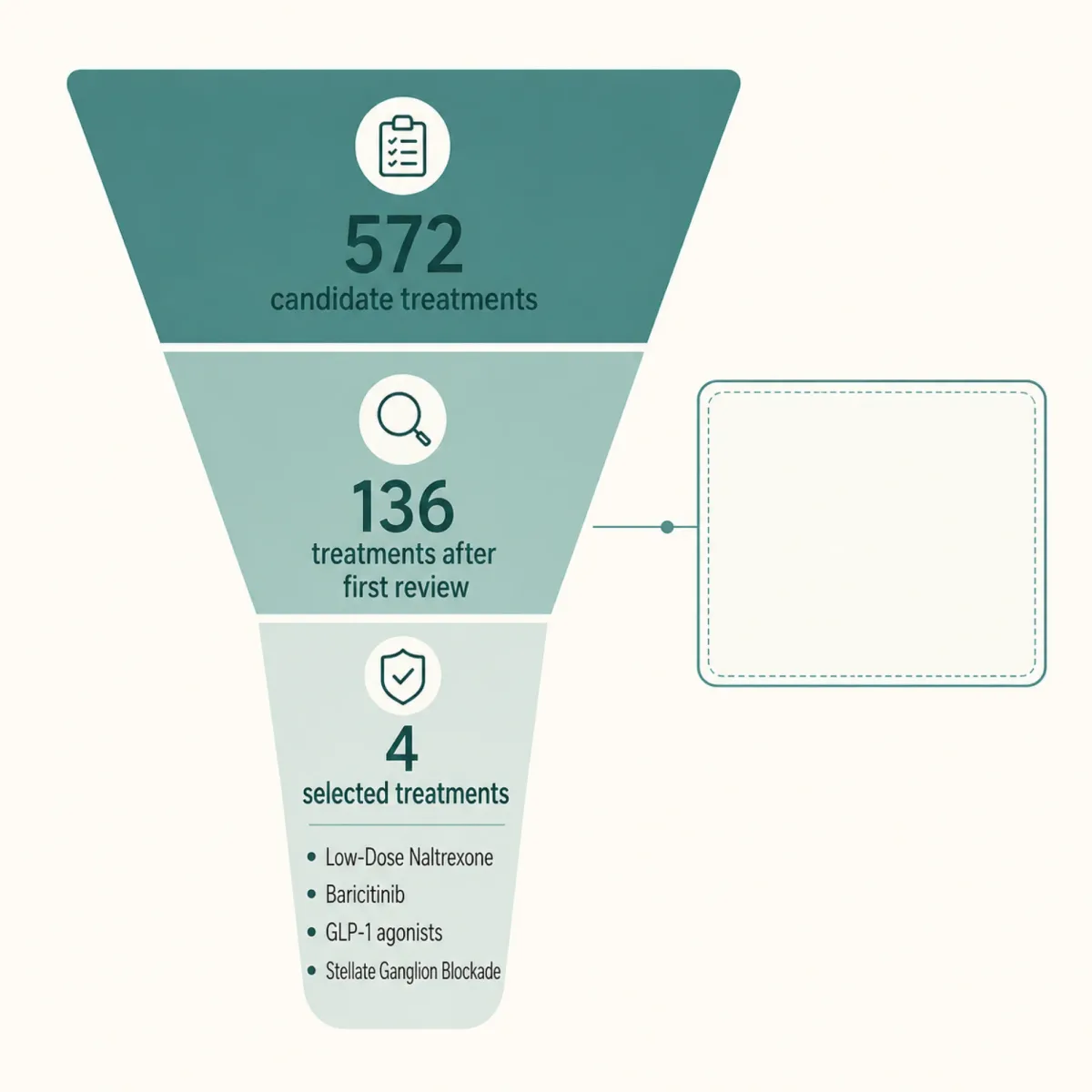
The NIH's RECOVER initiative — formally Researching COVID to Enhance Recovery — has commanded roughly $1.8 billion in funding. After a first round of trials that drew widespread criticism for landing modestly, RECOVER opened a second round in 2025. According to reporting by the long-COVID news outlet Health Rising, RECOVER asked the public for treatment ideas. The community responded with 572 candidates. After review, 136 made it through the first cut. From those, four were chosen for trials: low-dose naltrexone, baricitinib, GLP-1 agonists, and stellate ganglion blockade.
None of the four are peptides. Not Selank. Not Semax. Not Cerebrolysin. Not BPC-157. Not Dihexa.
That is not an accident of design. RECOVER specifically prioritized treatments with existing clinical signal — published case series, off-label experience, ongoing trials with promising signals. The four it picked include a generic that has decades of off-label use in chronic pain and fatigue (LDN), a JAK inhibitor with strong neuroinflammation rationale (baricitinib), a major drug class with new long-COVID interest (GLP-1s), and a procedural intervention with striking case reports (stellate ganglion blockade). Peptides did not survive the same review.
The academic medical centers running long-COVID care speak in similar terms. Stanford's 2025 symposium endorsed low-dose naltrexone as the most promising drug therapy in their toolkit and explicitly warned about the "wild west" of supplements pushed by private clinics. Yale's NeuroCovid clinic uses N-acetylcysteine paired with off-label guanfacine — based on a small Yale study published in November 2023 in Neuroimmunology Reports, with researchers now hoping for funding for larger trials. The University of Alabama at Birmingham published a 14-patient pilot RCT of Constraint-Induced Cognitive Therapy (CICT) in Rehabilitation Psychology in February 2026 — four of five non-retired CICT patients returned to work, versus none of five usual-care controls.
None of these labs and clinics endorse a peptide stack. None mention Cerebrolysin or Semax or Selank in their patient guidance. That silence is not subtle. It is the consensus position of the people running the largest evidence-based long-COVID programs in the United States.
What this means practically: if a clinic offering a peptide stack tells you their protocol is "evidence-based," ask which RCT they are referring to. The answer will be small Russian studies, mouse work, healthy-volunteer fMRI, or off-label clinical experience. None of it is at the level the FDA, NIH, or major academic centers consider sufficient to recommend.
Side Effects, Contraindications, and the FDA
The safety conversation around these peptides is shaped less by individual side effects — though those exist — and more by what the FDA has explicitly flagged about the substances themselves.
The FDA maintains a list of "bulk drug substances for use in compounding that may present significant safety risks." As of April 2026, the agency has placed Selank, Semax, BPC-157, Dihexa, and Epitalon — the entire palette of nootropic peptides marketed for cognitive support — on this list. The shared concern is immunogenicity: the risk that aggregated peptide impurities will trigger a damaging immune response when injected. The agency states bluntly for several of these compounds that it "lacks sufficient information to know whether the drug would cause harm when administered to humans."
Cerebrolysin sits in a different regulatory category. It is not on the FDA's bulk-substance list because it is a porcine-derived multi-peptide preparation rather than a single bulk peptide. It is approved abroad — in Russia, China, Mexico, and several European countries — but has never been FDA-approved in the United States.
Beyond the agency's structural concerns, the side-effect profiles reported by clinicians who prescribe them are not zero. Innerbody Research reports that Selank can cause injection-site reactions, GI discomfort, nausea, headaches, and dizziness, with contraindications including pregnancy, breastfeeding, and active cancer. Similar profiles apply to Semax. BPC-157's profile is poorly characterized in peer-reviewed human literature — itself a safety signal.
There is also a sourcing problem most patients do not fully understand. As Innerbody notes, most Selank sold online is "research-grade," not pharmaceutical-grade, meaning it has not met purity standards required for human use. Vials labeled "for research only" are, by FDA classification, not for injection into humans.
Stanford's Grossman captured the financial dimension cleanly: "Some patients are spending thousands of dollars on supplements they don't need. That's not ethical." Cerebrolysin courses run hundreds to thousands of dollars; Selank–Semax monthly programs commonly land in the $200 to $500 range. None of it is covered by insurance for off-label use.
What this means practically: a patient considering a peptide stack should know three things — the FDA has flagged most of these compounds for safety review, peer-reviewed human safety data is thin to absent, and most online supply is not legally for human use. None of those three statements is contested.
How to Talk to Your Post-COVID Clinician
Patients living with long-COVID brain fog do not need to be lectured out of investigating peptides. They need a structured conversation with a clinician who can help. The literature points to a clear set of questions worth raising at the next visit.
Start with the workup. Yale's protocol, as Lindsay McAlpine describes it, rules out the conditions that mimic long-COVID brain fog before settling on the diagnosis. Bloodwork covers complete blood count, comprehensive metabolic panel, thyroid function, and B-12. Obstructive sleep apnea is an under-diagnosed contributor. ADHD that was previously well-managed can decompensate after infection. POTS co-occurs in roughly 31% of highly symptomatic long-COVID patients per research summarized by Cognitive FX. ME/CFS overlap is common. Each of these has its own treatment path and can blunt cognitive recovery.
Once the workup is done, the questions worth asking your clinician are:
- "Have you ruled out OSA, thyroid dysfunction, B-12 deficiency, ADHD relapse, POTS, and ME/CFS overlap?"
- "What is your read on N-acetylcysteine plus guanfacine off-label, based on the Yale data?"
- "Am I a candidate for low-dose naltrexone? What dose?"
- "Are there RECOVER-TLC trials I qualify for in my region?"
- "What do you think about peptide therapy for this condition? What evidence are you relying on?"
That last question is the cleanest test of any clinic offering a peptide stack. The right answer is not a marketing brochure. It is a list of trials by name, sample size, and outcome. If the answer is small Russian fMRI work or unpublished case series — fine, but understand that is the level of evidence you are relying on.
What the literature recommends against, with rare unanimity across Stanford, Yale, and the NIH: spending thousands at a private clinic on protocols not backed by RCT data, buying research-grade peptides online for self-injection, and skipping the standard medical workup in favor of a stack.
The honest summary: long-COVID brain fog is real, the mechanisms behind it map plausibly onto what nootropic peptides claim to do, and there is currently no published RCT showing any of these peptides treats it. A 30-day course will deliver something — placebo response, real subjective benefit, the natural arc of recovery, a side effect, or nothing. What it will not deliver, in 2026, is evidence that the stack worked. Until that evidence exists, the useful thing a patient can do is get the workup, ask the questions, and be honest about which boxes are ticked and which are not.
Frequently Asked Questions
Is there any FDA-approved peptide treatment for long-COVID brain fog?
No. As of mid-2026, the FDA has not approved any peptide for long-COVID cognitive symptoms. The agency has flagged Selank, Semax, BPC-157, Dihexa, and Epitalon on its Category 2 list for compounding safety risks. Cerebrolysin is not FDA-approved in the United States, though it is approved in several other countries. The largest U.S. trial of cognitive interventions for long COVID, RECOVER-NEURO, did not include any peptide arms.
How long does long-COVID brain fog usually last?
Most patients see resolution between six and nine months after infection, though Yale's Lindsay McAlpine, MD, has seen cases last 18 months or more. A Brazilian cohort study of 297 patients found measurable cognitive deficits persisting at least three years after infection in older adults and those with severe initial illness. Severity at infection and age are the strongest predictors of persistence.
What pharmaceutical treatments do major long-COVID clinics actually use?
Yale's NeuroCovid Clinic uses N-acetylcysteine combined with off-label guanfacine, based on a 2023 study in Neuroimmunology Reports by Arman Fesharaki-Zadeh, MD, PhD. Stanford's program endorses low-dose naltrexone as the most promising drug therapy. The University of Alabama at Birmingham reported success with Constraint-Induced Cognitive Therapy (CICT) in a 14-patient pilot RCT published in Rehabilitation Psychology in early 2026. The NIH's RECOVER-TLC initiative is currently funding trials of low-dose naltrexone, baricitinib, GLP-1 agonists, and stellate ganglion blockade.
Why do some patients report improvement on peptide stacks if there's no trial evidence?
Several explanations apply. RECOVER-NEURO's coverage by The Psychiatrist's Newsletter noted that people with more recent infections improved the most regardless of treatment — meaning natural recovery accounts for many "I tried this and got better" stories. Placebo response is well-documented in cognitive trials. Anxiety reduction from a calming protocol like Selank's GABAergic action might genuinely help patients whose fog has a stress component. None of these effects requires the peptide to be doing what its marketing claims.
Is it safe to buy these peptides online?
Most peptides sold online are labeled "research-grade" — meaning they have not met FDA chemical purity standards for human use and are technically not for injection into humans. The FDA's immunogenicity concerns specifically relate to aggregated peptide impurities from inadequately controlled production. A patient buying online may receive a vial that contains the labeled peptide alongside contaminants the agency considers a safety signal. Even pharmaceutical-grade compounded peptides require an FDA-registered compounding pharmacy and a clinician's prescription.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.