Somewhere on a research-chemical site this afternoon, a 5-milligram vial of dihexa is sitting in a shopping cart for $69. The customer has read that this peptide is "seven times stronger than BDNF," the so-called "Miracle-Gro for the brain." Maybe he has read it is "seven orders of magnitude" stronger, which is ten million times. He clicks "checkout."
What he probably has not read is that Athira Pharma, the company that built its entire pipeline on dihexa, watched its Phase 2/3 Alzheimer's trial fail in September 2024, with a p-value of 0.70 on the primary endpoint. Or that the foundational synaptogenesis paper was retracted in April 2025. Or that the CEO resigned over altered images in her dissertation.
This is the gap between research and reputation. Dihexa might be the most lopsided story in the nootropic world right now: real biology, real patents, real intrigue, and zero published human trials of the molecule itself. Here is the honest version, end to end.
What Dihexa Actually Is (And Why The Chemistry Matters)
Dihexa is six letters of pharmacology shorthand for a compound with an unwieldy real name: N-hexanoic-Tyr-Ile-(6) aminohexanoic amide. It carries the developmental code PNB-0408 and the CAS number 1401708-83-5. The molecule weighs 504.66 grams per mole, with formula C27H44N4O5. That is small for a peptide drug, about half the size of insulin, and the size is the whole engineering point.
The starting material is angiotensin IV, a six-amino-acid peptide most people have never heard of. Angiotensins generally regulate blood pressure, but in 1992, medicinal chemist Joseph Harding and neuroscientist John W. Wright at Washington State University noticed something odd in their hippocampal experiments: angiotensin IV, or early derivatives of it, could reverse the learning deficits seen in dementia models. The catch was that the natural peptide got chewed up by enzymes within minutes and could not cross the blood-brain barrier. The only way to test it was to drill a hole and deliver it directly into the brain. "That's useless," Harding recalled saying. "I mean, who wants to drill holes in people's heads?"
Five years of tinkering later, in 2007, Harding built a smaller version that solved both problems. The hexanoyl groups at each end act like armor against protein-cleaving enzymes. The compact, lipophilic shape lets it slip across the blood-brain barrier and even cross the gut wall when swallowed. Studies confirm dihexa is "an oral active, blood-brain barrier-permeable angiotensin IV analogue" with "a long cyclic half-life." Translation: it is one of the rare peptides you can take orally and still have it reach your brain in active form. Most peptides (insulin, GLP-1 agonists, growth-hormone-releasing peptides) die in the stomach.
Where The 7× BDNF Number Comes From, Sourced Honestly
The phrase you keep seeing in nootropic videos and Reddit threads, "7 times stronger than BDNF" or "7× BDNF," is a corruption of a much bigger and more specific claim that came directly from the original 2012 Washington State University press release.
The original wording was clear. Harding, Wright, and colleagues compared dihexa head-to-head with brain-derived neurotrophic factor in cell-culture assays of new synapse formation. Their finding: dihexa was "seven orders of magnitude more powerful than BDNF." Not seven times. Seven powers of ten. The press release spelled it out: "It would take 10 million times as much BDNF to get as much new synapse formation as Dihexa."
Somewhere along the way to the supplement aisle, "ten million times" became "seven times." A 2021 paper from a peripheral-nerve regeneration group, citing the same finding, rendered it as "seven times greater than BDNF". From there it propagated. By the time you see it on a peptide vendor's homepage, the qualifier (that this was an in-vitro assay in rat hippocampal cell culture, comparing molar potency on dendritic spine formation) has usually been quietly removed.
Quick fact: The "7× BDNF" headline is a degraded telephone-game version of "seven orders of magnitude," and that bigger number is itself a measurement of in-vitro spinogenesis potency, not human cognition.
Why does BDNF matter as the comparison at all? Because BDNF is the gold-standard neurotrophic factor that brain-health researchers have been chasing for thirty years. Autopsy studies of Alzheimer's patients show lower BDNF levels in the brain. The problem is that BDNF itself, as a 27-kilodalton protein, cannot cross the blood-brain barrier, costs a fortune to synthesize, and has never been successfully developed as a drug. So when a 504-dalton peptide comes along claiming a fraction of BDNF's effect at a fraction of BDNF's molecular weight, drug developers get interested.
The honest read: dihexa was, in those original cell-culture experiments, dramatically more potent than BDNF on a per-molecule basis at making rat hippocampal neurons sprout new dendritic spines. That is a chemistry result. It does not mean dihexa is "ten million times better at making you smarter." Nobody has ever measured anything close to that, in any species, on any cognitive task.
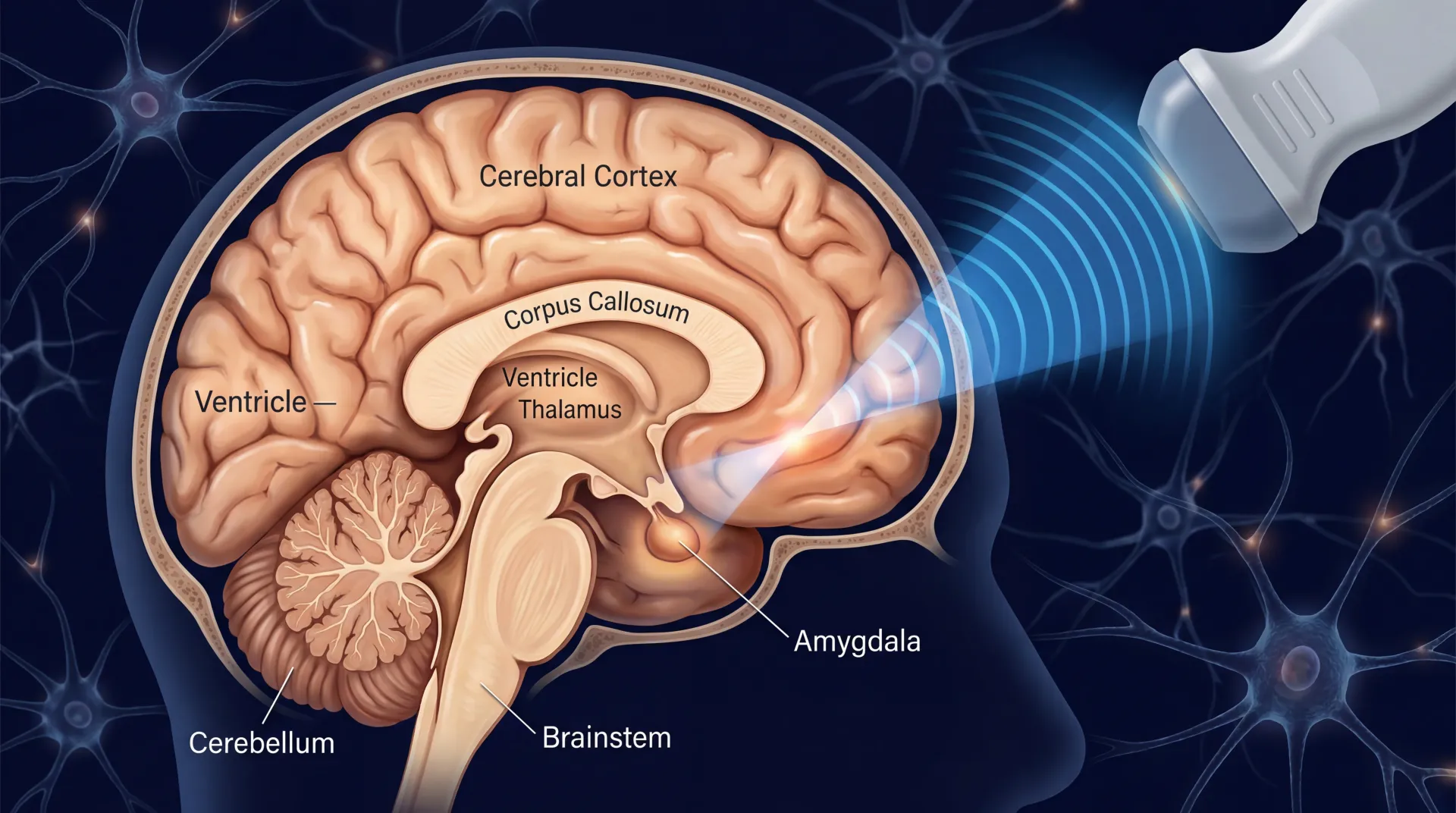
How Dihexa Builds New Synapses: HGF, c-Met, And Brain Plumbing
Forget angiotensin for a minute. Once dihexa is in the brain, the protein it actually grabs is hepatocyte growth factor, usually written HGF. HGF was originally discovered by liver biologists, but HGF and its receptor, c-Met, are also expressed across the brain, particularly in hippocampal neurons, prefrontal cortex, and glial cells. This system promotes neuron survival, dendrite growth, and synapse wiring. In Alzheimer's brains, the MET receptor in the hippocampus appears to be downregulated.
Dihexa's binding affinity for HGF is genuinely impressive. Vendor data sheets list a Kd of 65 picomolar, picomolar not nanomolar, meaning dihexa sticks to HGF at concentrations far below what most drugs require. Once bound, dihexa makes HGF more likely to dimerize, which is the configuration HGF needs to fire its c-Met receptor. Think of it less as a drug that turns on a switch and more as a chaperone that helps two HGF molecules find each other so they can do what they were going to do anyway.
Imagine a busy office where two coworkers need to shake hands to start a project, but the room is too crowded for them to find each other. Dihexa is the colleague who taps them both on the shoulder and points them in the right direction. The handshake (HGF dimerization) activates c-Met, which triggers downstream pathways that make neurons sprout new dendritic spines.
Independent confirmation arrived from a non-WSU group in 2025. Rowan University researchers, working in a closed-head mild traumatic brain injury model in rats, used dihexa to rescue working memory after repeated brain impacts. When they pre-treated animals with a MET antagonist, the effect vanished, exactly what you would expect if HGF/MET signaling is the mechanism. That control matters because it pins the mechanism without depending on data from the original WSU lab.
The practical implication: when you see a peptide marketed as "amplifying BDNF directly," that's a misstatement. The mechanism is HGF-dependent. BDNF is the comparison baseline, not the target.
What Rodent Studies Have Shown (And What They Have Not)
The animal data on dihexa is more substantial than its critics admit, and weaker than its promoters imply. Both can be true.
The strongest line of evidence is in scopolamine-induced learning deficits. Scopolamine blocks acetylcholine receptors and reliably wrecks rats' performance on the Morris water maze. Harding's group reported that scopolamine-treated rats given dihexa orally, by injection, or directly into the brain all relearned the task. "Same result, every time," Harding said. Aged-rat experiments showed similar improvements in smaller groups.
A separate group at Nanjing First Hospital published a 2021 paper in Brain Sciences using APP/PS1 transgenic mice. They gave dihexa orally at 1.44 and 2.88 mg/kg per day for three months. The high-dose group showed restored spatial learning, increased neuronal cell counts, lower pro-inflammatory cytokines (IL-1β and TNF-α), and higher anti-inflammatory IL-10. Wortmannin, a PI3K inhibitor, blocked the effects, pointing to the PI3K/AKT pathway downstream of HGF.
A 2021 Harding-co-authored paper used dihexa with mesenchymal stem cells in a rat sciatic nerve transection model, finding improved limb function recovery, so the synaptic-rebuilding story is not strictly limited to the brain.
Here is the awkward part. The foundational mechanistic paper, Benoist et al. 2014 on the HGF/c-Met dependence, was retracted in April 2025. An expression of concern appeared in 2021. The retraction cites image and data integrity issues. Several downstream papers cited Benoist 2014 as primary evidence for the synaptogenic mechanism, so its retraction reverberates through the literature.
What rodent studies have not shown: that dihexa improves cognition in healthy animals beyond baseline, that benefits persist after dosing stops, or that doses translate cleanly to humans. The 2013 patent itself acknowledged that "short duration safety studies with dihexa have uncovered no apparent toxicity," short duration being the operative phrase, since c-Met is a recognized oncogene and chronic c-Met potentiation in humans has never been characterized.
The Human-Trial Gap: Why There Is No Clinical Data
Here is the cleanest way to say it: there has never been a published human clinical trial of dihexa. Zero.
Every human dataset attached to the dihexa story is actually a trial of fosgonimeton, also known as ATH-1017 or NDX-1017, a phosphate prodrug administered as a daily subcutaneous injection. AlzForum notes the prodrug generated "higher blood and brain levels" than direct delivery of the active metabolite would have allowed. So when peptide-vendor sites cite "human safety trials," they are talking about fosgonimeton. Different molecule. Different route. Read carefully.
The Phase 1 trial (NCT03298672), published by Hua and colleagues in 2022, enrolled 88 participants: 48 healthy young men, 29 healthy elderly volunteers, and 11 Alzheimer's patients. Doses ran from 2 to 90 milligrams subcutaneously. The drug was safe and well-tolerated; pharmacokinetics were dose-proportional. In the small Alzheimer's subgroup (seven on 40 mg versus four on placebo), researchers measured a statistically significant normalization of ERP P300 latency (p=0.027). No cognitive tests were administered.
The Phase 2 ACT-AD trial (NCT04491006) enrolled 77 mild-to-moderate Alzheimer's patients on 40 mg, 70 mg, or placebo for six months. It failed its primary ERP P300 endpoint. Athira's post-hoc explanation: 60% of participants were also on acetylcholinesterase inhibitors that may have antagonized fosgonimeton.
The Phase 2/3 LIFT-AD trial (NCT04488419) ran 26 weeks at 90 US sites, enrolling 549 participants with 287 in the efficacy analysis. In September 2024, Athira announced the trial had failed its primary endpoint and both key secondary endpoints. The published numbers from the trial paper:
- Global Statistical Test (combined cognitive and functional): change of −0.08 favoring fosgonimeton, p=0.70
- ADAS-Cog11 (cognition): change of −0.70 favoring fosgonimeton, p=0.35
- ADCS-ADL23 (activities of daily living): change of +0.67 favoring fosgonimeton, p=0.61
Only plasma p-tau217 reached nominal significance. Twenty-two percent of participants dropped out due to injection-site reactions. The Parkinson's-disease-dementia trial (SHAPE, NCT04831281) had already failed in December 2023. The open-label extension (NCT04886063) was terminated after LIFT-AD failed, with sponsorship moving from Athira to LeonaBio. The prodrug failure is the closest signal we have to "does it work in humans." It did not work in the population that mattered most.
WSU To Athira Pharma: The Drug-Development Story Behind It
Harding and Wright spun off M3 Biotechnology Inc. from WSU around 2012 to commercialize dihexa. M3 became Athira Pharma in 2019. The lead compound, originally NDX-1017, became ATH-1017 in 2020. In March 2022, the World Health Organization's International Nonproprietary Names Expert Committee designated it fosgonimeton and created the suffix stem "-meton" as a novel drug-class designation for HGF/MET positive modulators. Fosgonimeton was the first.
The patent, US 8,598,118, issued in December 2013, listing Harding, Wright, Caroline Benoist, Leen Kawas, and Gary Wayman as inventors. Kawas, who became Athira's chief executive, is where this story takes a difficult turn.
In June 2021, Kawas was placed on temporary leave after questions surfaced on PubPeer about figures in her doctoral dissertation, work that had laid foundations for ATH-1017. According to AlzForum's compilation, an independent investigation found altered images in her dissertation and at least four publications related to her graduate work. She resigned in October 2021.
None of this means dihexa is fake or that HGF/MET activation isn't a real mechanism; the independent 2025 Rowan University replication suggests the basic biology is intact. But the foundational papers that cemented dihexa's reputation as a synaptogenic powerhouse need to be read with the retraction and integrity context in mind.
After LIFT-AD failed in September 2024, Athira announced a strategic pivot away from dihexa-derived compounds toward a newer, orally available HGF/MET modulator called ATH-1105 for amyotrophic lateral sclerosis. The takeaway is not "the science was a fraud." It is closer to "the company that bet its identity on this molecule could not get a clinical win after a decade and several hundred million dollars." That should temper expectations regardless of what individual users feel they experience.
The Research-Chemical Reality: Sourcing, Dosing, Risks
If you actually walk into the dihexa marketplace, here is what it looks like. MedChemExpress sells 2 mg for $120, 100 mg for $950, and 1 g for $2,850. Cayman Chemical lists 5 mg at $69 and 50 mg at $449. These are research-grade vendors selling to laboratories. Their packaging carries the standard disclaimer: "For research use only. We do not sell to patients."
The actual nootropic-consumer market is downstream of these vendors and operates under different rules. A 2025 surveillance study run by twelve official medicines control laboratories across the European Union and Australia examined 159 illicit nootropic samples from January 2020 through September 2024. Sixty-nine percent of the samples were collected from the illegal market. The study explicitly flagged the problem: many of these products contain "research chemicals for which limited or no pharmacological and/or toxicological data are available." That category includes peptides like dihexa.
What is the dose? The honest answer is nobody knows the human dose. Athira used 40 mg subcutaneously per day, but that's a different molecule. Rodent oral dosing in the APP/PS1 study was 1.44 to 2.88 mg/kg per day, which scales by rough body-surface-area conversion to about 14 to 28 mg per day for a 70 kg human. Reconstitute-and-inject protocols in nootropic forums suggest 8 to 10 mg orally per day, which has zero validation.
Side effects? MediSearch acknowledges: "There isn't enough data on the side effects of Dihexa." That's the cleanest statement in the consumer literature. No long-term human data exists. The c-Met receptor dihexa potentiates is a known oncogene, and the patent itself notes only "short duration" safety studies, weeks not years.
For readers familiar with other nootropic peptides, like Selank and Semax, or the polypharmacy stack discussed in our long-COVID brain-fog piece, dihexa sits in a more dangerous category. Selank and Semax have Russian clinical-use history and decades of human experience. Dihexa has neither. Anyone considering it is doing first-in-human research on themselves.
So what: If you are tempted by the "7× BDNF" headline, ask whether the trade you are actually making is "I am buying a research chemical with zero human trials, an indeterminate dose, and an unmeasured oncogenic risk, in exchange for a marketing claim that started its life as an in-vitro spinogenesis assay measurement that has since been partially retracted." That is the trade. It is not the trade most consumers think they are making.
Frequently Asked Questions
Is dihexa actually 7× stronger than BDNF, or is that a myth?
The original 2012 Washington State University claim was that dihexa was seven orders of magnitude (roughly ten million times) more potent than BDNF in cell-culture spinogenesis assays. The "7×" version that circulates online is a degraded restatement. Even the original number measures molar potency in rat hippocampal neuron culture, not cognitive effect in humans. The headline does not translate to a real-world cognitive benefit anyone has measured.
Is dihexa FDA-approved?
No. Dihexa itself has never entered FDA-monitored clinical trials in humans. The phosphate prodrug fosgonimeton (ATH-1017) reached Phase 2/3 trials with Athira Pharma but failed its primary endpoint in mild-to-moderate Alzheimer's disease in September 2024. All Athira Alzheimer's, Parkinson's-dementia, and dementia-with-Lewy-bodies programs have been discontinued.
What happened to the Benoist 2014 paper?
The foundational HGF/c-Met mechanism paper was retracted in Journal of Pharmacology and Experimental Therapeutics in April 2025, after an expression of concern in 2021. The retraction cited data integrity issues and is part of the broader WSU investigation that also resulted in former Athira CEO Leen Kawas's resignation.
Can dihexa be taken orally?
In rodents, yes; that is one of the molecule's chemistry advantages. Dihexa was specifically designed to survive gut digestion and cross the blood-brain barrier. In humans, oral pharmacokinetics have not been characterized in any published trial. The Athira clinical program used the prodrug fosgonimeton via subcutaneous injection, not oral dihexa.
Why did Athira's trials fail if the rodent data was so strong?
This is the multi-billion-dollar question in Alzheimer's drug development. Many compounds that work in transgenic mouse models have failed in human trials; mouse models capture only a slice of human Alzheimer's biology. Athira's specific theory was that concomitant cholinesterase inhibitors antagonized fosgonimeton, which is why LIFT-AD restricted enrollment to AChEI-free patients. It still did not produce a significant cognitive benefit.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.