What happens when you point sound waves at the brain's fear center?
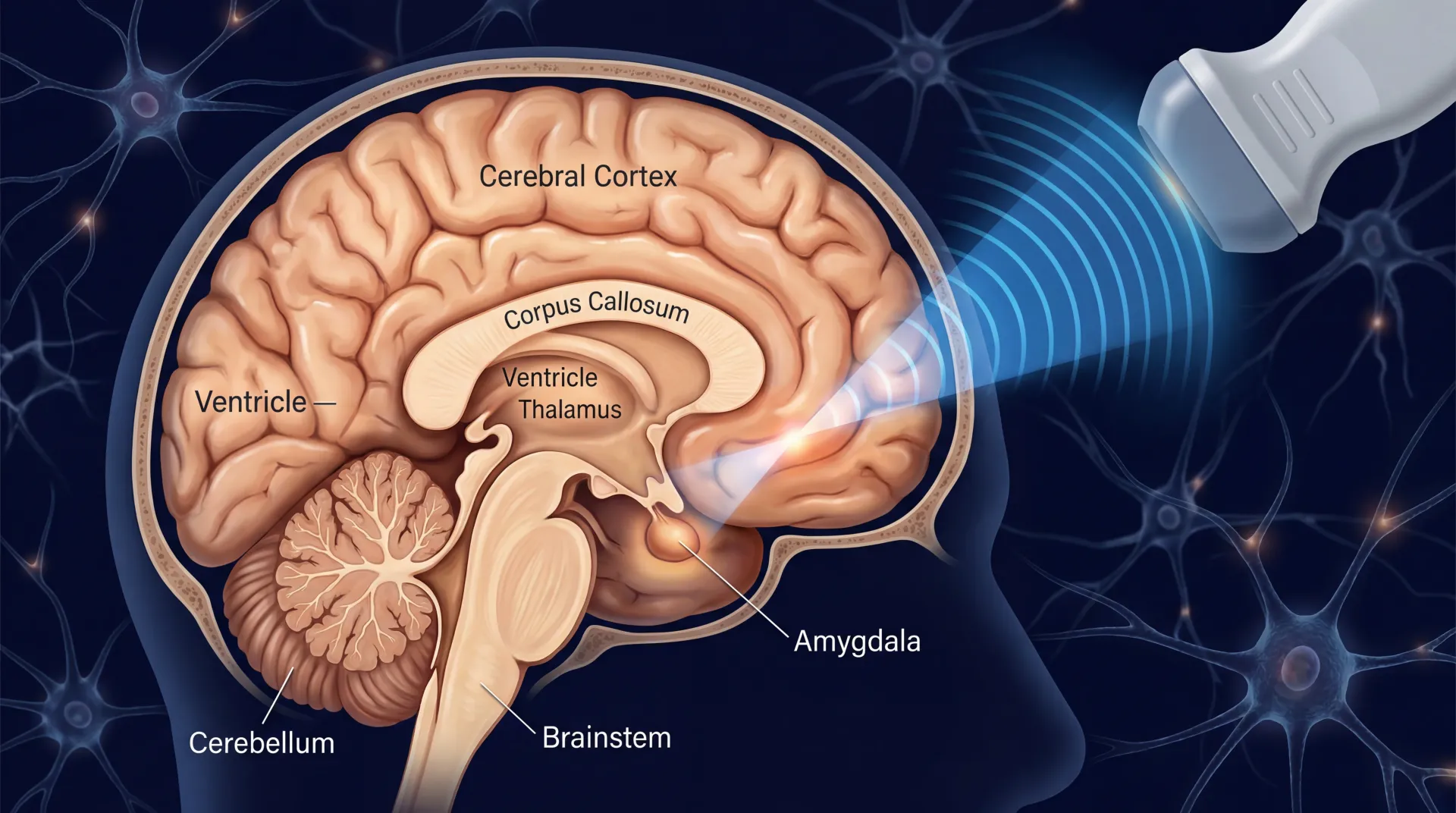
Somewhere between the frequency of a dog whistle and the hum of a medical ultrasound, there is a band of acoustic energy that can pass through your skull, converge on a region the size of a grain of rice deep inside your brain, and change how the neurons there fire. No incision, no electrode, no anesthesia. The patient sits in a chair with a transducer pressed against their temple, and the treatment session lasts minutes.
That is low-intensity focused ultrasound (LIFU), and it works through a mechanism that scientists have been chasing since 1929, when a physiologist named E.N. Harvey discovered that ultrasonic stimulation of a frog's sciatic nerve could trigger muscle twitching and alter heart rate. Nearly a century later, the principle is the same — sound waves can nudge neurons — but the precision has improved by orders of magnitude.
Think of it like using a magnifying glass to focus sunlight on a single point, except the energy source is sound rather than light, and the target is a specific brain structure rather than a leaf. A transducer sends acoustic pulses into the brain, and the geometry of those pulses creates a focal point — called a sonication zone — where the energy concentrates. Outside that zone, the sound passes through tissue harmlessly. Inside it, the acoustic pressure activates mechanosensitive ion channels on neuron membranes, particularly Piezo1 channels, triggering calcium influx that modulates how those neurons fire.
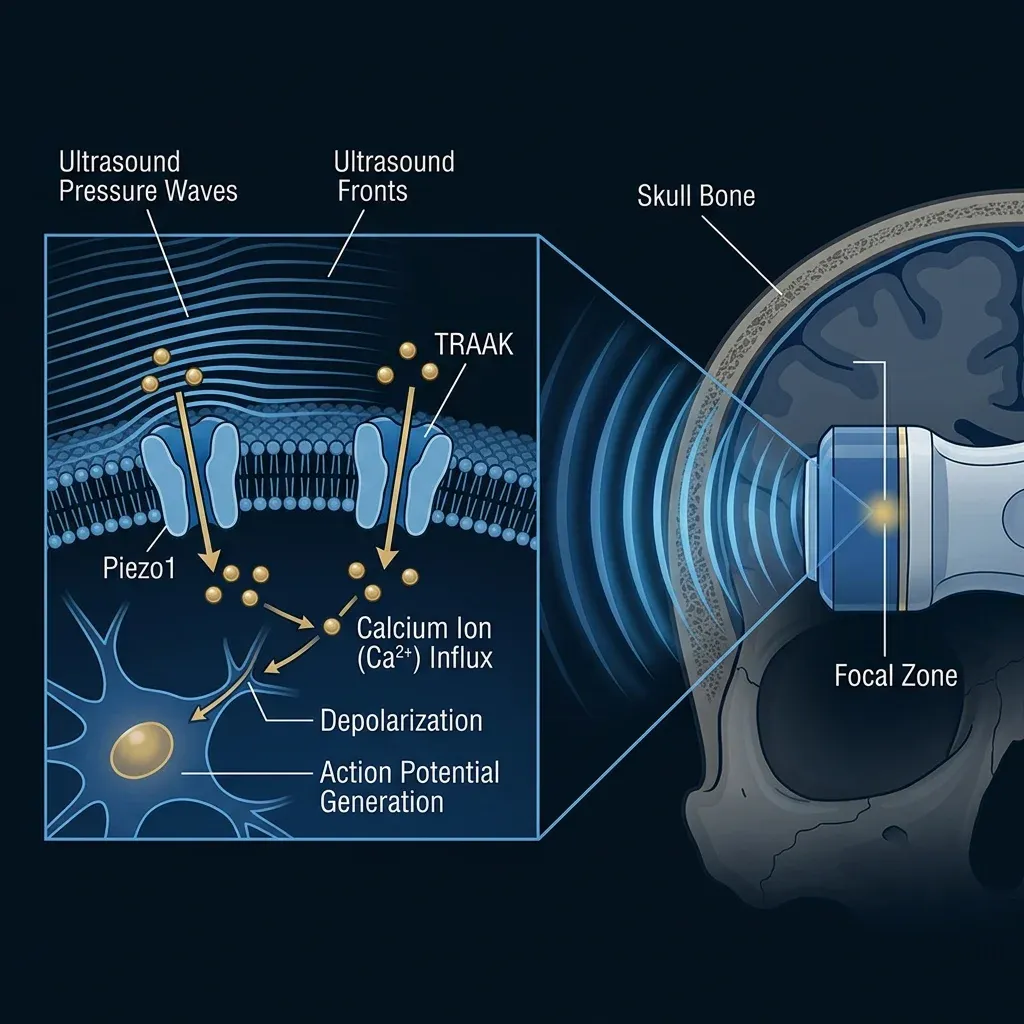
The temperature change this produces in brain tissue is less than two-tenths of a degree Celsius — negligible compared to the thermal ablation used in surgical focused ultrasound, which heats tissue above 55 degrees to destroy it. LIFU operates in a completely different range. It modulates neurons. It does not damage them.
What separates this from sticking electrodes in someone's brain or aiming magnetic pulses at their cortex is where the effect happens. LIFU can reach structures like the amygdala, the thalamus, the nucleus accumbens, and the subgenual cingulate cortex — the deep-brain regions most implicated in depression, anxiety, PTSD, and addiction — without requiring any part of the treatment to cross the blood-brain barrier or break the skin.
The effects are not limited to the seconds during sonication. Research in macaques demonstrated that a single sonication produced changes in brain connectivity that persisted for over an hour. In repeated-session protocols, evidence points to synaptic plasticity — the brain physically rewiring in response to treatment, including new dendritic spine formation and upregulated BDNF-TrkB signaling pathways, the same molecular machinery involved in learning and memory. That persistence is what makes LIFU a candidate for treating psychiatric conditions rather than just probing them.
The 3-week experiment that changed how we treat mood disorders
In April 2025, a team at the University of Texas at Austin published results that shifted the conversation from "this technology is interesting" to "this technology works in patients." Gregory Fonzo, a psychiatrist and neuroscientist at Dell Medical School, had spent years building toward a question nobody had answered: what happens when you aim focused ultrasound at the amygdala — the brain's threat-detection hub — in people who are clinically depressed, anxious, or traumatized, and you do it every day for three weeks?
The study ran in two phases. Phase one was a double-blind, sham-controlled target engagement trial with 29 patients with mood, anxiety, and trauma-related disorders (MATRDs) and 23 healthy controls. Each participant received both active and sham ultrasound sessions, separated by about a week, without knowing which was which. The active sessions used a BrainSonix Pulsar 1002 transducer placed against the left temporal bone — the thinnest part of the skull — and guided by structural MRI to hit the left amygdala. The sham sessions used an identical setup with a blocking pad that prevented the ultrasound from reaching the brain.

The results from phase one confirmed that the ultrasound was actually reaching and affecting the amygdala. Active treatment, compared to sham, reduced left amygdala blood oxygenation level-dependent (BOLD) signal and produced differences in hippocampal and insular responses specific to patients.
Phase two was the treatment trial. Twenty-five patients with diagnosed conditions including major depression, bipolar disorder, generalized anxiety, PTSD, social anxiety, and panic disorder received daily ultrasound sessions — fifteen total, delivered Monday through Friday for three consecutive weeks. Twenty-one of twenty-four participants who started treatment completed all fifteen sessions — an 88% completion rate.
The primary outcome measure was the Mood and Anxiety Symptom Questionnaire General Distress subscale. The treatment hit its target: statistically significant reductions in general distress scores (p = 0.001) with a Cohen's d of 0.77 — a medium-to-large effect size. Secondary measures showed effect sizes ranging from 0.43 to 1.50 across depression, anxiety, and trauma-specific scales. Amygdala activation to emotional stimuli dropped significantly after the three-week course.
"What makes this approach revolutionary is that it's the first time we've been able to directly modulate deep brain activity in patients without invasive procedures or medications." — Gregory Fonzo, PhD, UT Austin Dell Medical School
No serious adverse events occurred. By the standards of psychiatric interventions, the treatment was well tolerated. For context, the three-week daily protocol is similar in time commitment to an intensive TMS course, but it reached a brain region that TMS physically cannot.
TMS, DBS, and the depth problem nobody solved — until now
To understand why LIFU matters, you need to understand the limitation it overcomes. Psychiatric brain stimulation has been trapped in a tradeoff for decades: you can go deep, or you can be non-invasive. You could not do both.
| Feature | TMS | Deep Brain Stimulation | Focused Ultrasound (LIFU) |
|---|---|---|---|
| Invasiveness | Non-invasive | Surgical implant | Non-invasive |
| Depth reach | ~2-4 cm (cortical) | Any depth (electrode) | Any depth (acoustic) |
| Spatial precision | Centimeters | Millimeters | Millimeters |
| Reversible | Yes | Yes (while active) | Yes |
| FDA-approved for psychiatry | Depression, OCD | OCD (humanitarian) | Not yet |
| Targets subcortical structures | Indirectly | Directly | Directly |
| Requires anesthesia/surgery | No | Yes | No |
Transcranial magnetic stimulation uses alternating magnetic fields to induce electrical current in the brain, but those fields decay exponentially with depth. Standard TMS coils reliably affect cortical tissue — the outer few centimeters. "Deep" TMS coils, like the H-coil used in some depression protocols, can push to about four centimeters, but with reduced spatial focus and at intensities that approach the upper safety limits for seizure risk. The amygdala sits roughly six to seven centimeters from the scalp. TMS cannot reach it directly. Instead, clinicians target cortical regions like the dorsolateral prefrontal cortex and rely on downstream network effects to indirectly modulate deeper structures. That indirect approach works for many patients, but it depends on the integrity of the connections between cortical and subcortical regions — connections that may themselves be disrupted in the illness being treated.
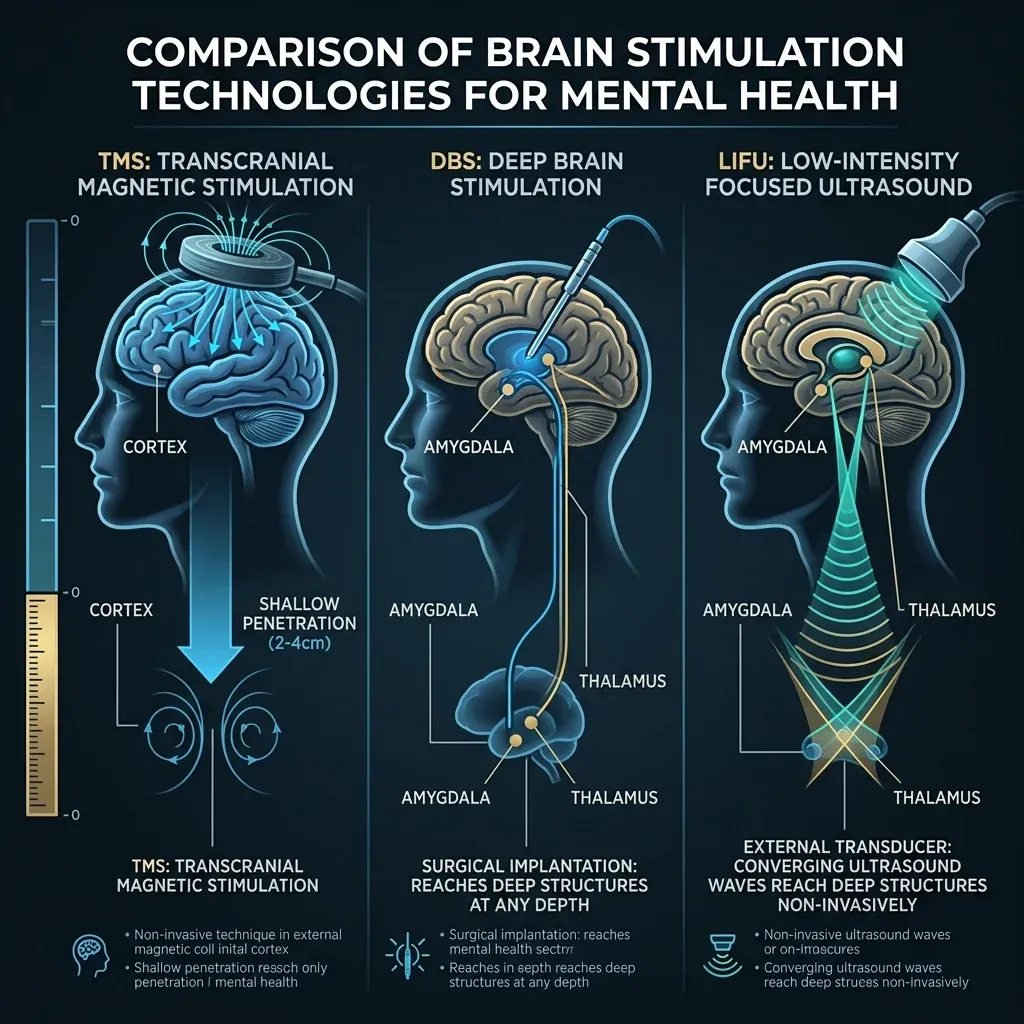
Deep brain stimulation solves the depth problem completely. Surgeons implant electrodes directly into target structures — the subthalamic nucleus for Parkinson's, the ventral capsule for OCD — and deliver continuous electrical stimulation. DBS has FDA humanitarian device approval for intractable obsessive-compulsive disorder and is investigational for treatment-resistant depression. The precision is excellent. The drawback is obvious: it requires brain surgery, with associated risks of infection, bleeding, and the complexity of maintaining an implanted device indefinitely.
LIFU occupies the space these two approaches left empty. It matches DBS for depth — reaching the amygdala, nucleus accumbens, thalamus, or any other deep structure — while matching TMS for non-invasiveness. The patient goes home after the session. There is nothing left in their brain when treatment ends. If the approach does not work, there is nothing to remove.
Six countries, a dozen labs, and the race to prove it works
The Fonzo trial was a proof of concept. What followed is an international push to turn that proof into a clinical treatment. A 2026 scoping review in the Journal of Neural Transmission screened 320 studies and identified 14 that met criteria for human psychiatric applications of focused ultrasound neuromodulation. The conditions studied span major depressive disorder, generalized anxiety, schizophrenia, OCD, and substance use disorder. Symptomatic improvement was reported across all of them, though the strength of evidence varies considerably.
The most developed evidence base is in depression. The largest randomized controlled trial to date enrolled 30 MDD patients and found significant reductions in depression severity that persisted — and even further improved — at three-month follow-up (Cheung et al., 2023). A separate RCT by Oh et al. in 2024 found significant clinical improvement in depression scores and suicidal ideation, with further gains at two-week follow-up.
At UCLA, Taylor Kuhn and Michelle Craske are running ILIAD — the first double-blinded, sham-controlled RCT targeting the caudate head and nucleus accumbens specifically in people with anhedonic depression. Anhedonia — the inability to feel pleasure — is one of the most treatment-resistant features of depression, responding poorly to both medication and psychotherapy. Anhedonic depression carries higher suicide risk and longer episodes. The ILIAD protocol delivers three LIFUP sessions over five to nine days and tracks changes through functional MRI, digital phenotyping via Apple Watch, and an array of self-report measures over seven weeks.

At the VA Providence Healthcare System in Rhode Island, Noah Philip's team is running NCT05147142 — a randomized, single-blind crossover trial of LIFU targeting the amygdala in 25 veterans with major depressive disorder. The study started in September 2021 and has an estimated completion date of March 2026. Philip's lab is also launching controlled trials evaluating FUS for PTSD and anhedonia.
Beyond those, the Focused Ultrasound Foundation tracks active depression trials in Utah, South Carolina, Ontario (Canada), and France, each using different devices and targeting strategies. This diversity is both strength and challenge — researchers are exploring multiple approaches simultaneously, but the heterogeneity makes it harder to compare results across sites.
One brain injury, a skull that fights back, and other reasons for caution
The safety profile of LIFU is clean so far, with one serious exception that researchers are transparent about. A patient receiving focused ultrasound to the nucleus accumbens for substance use disorder suffered a microhemorrhage and edema at the target site. The team later disclosed that the mechanical index during the procedure exceeded 1.9 — the FDA's upper safety limit. In practical terms, this means the injury occurred during a protocol that would not qualify as low-intensity focused ultrasound by current safety standards. The incident prompted significant attention to safe administration practices, similar to how early TMS seizures led to stricter stimulation guidelines.
Within the low-intensity range, the data is encouraging. Across multiple studies, between 4% and 11% of participants report mild-to-moderate adverse events — typically neck pain, sleepiness, muscle twitches, itchiness, or headache. These resolve quickly, usually within a week. The Fonzo trial recorded no serious adverse events across all 15 treatment sessions in 24 patients.
| Concern | Current Evidence | Severity |
|---|---|---|
| Mild side effects (headache, sleepiness) | 4-11% of participants | Low — resolves in days |
| Skull attenuation | 56% pressure loss, 84% intensity loss | Technical challenge, not patient risk |
| Brain injury | 1 case — MI exceeded safety limit | Serious, but outside LIFU parameters |
| Suicidal ideation | Flagged in 1 subcallosal cingulate study | Under investigation |
| Long-term effects unknown | Limited follow-up data | Unknown |
The skull itself is one of the technology's biggest physical obstacles. Computational modeling shows that the human skull absorbs 56% of peak pressure and 84% of peak intensity as ultrasound passes through it. That is 20 times more attenuation than soft tissue. Skull thickness, bone density variations, and the angle of the transducer all affect whether the acoustic beam arrives at the intended target with the intended intensity. In 6% to 27% of patients, skull heterogeneity prevents achieving adequate energy delivery without correction algorithms.
There are also questions that simply do not have answers yet. How long do treatment effects last? The scoping review found mixed durability across studies — some showing sustained improvement at three months, others showing regression. What are the optimal parameters? Session durations range from 5 to 64 minutes across different protocols, with no consensus on frequency, intensity, or number of sessions. Whether the same parameters work for depression, anxiety, and PTSD — or whether each condition requires a different recipe — remains an open question.
One uncomfortable finding from the subcallosal cingulate study: FUS targeting that region was associated with improved mood and depression, but also raised questions about near-term emergence of suicidal ideation in at-risk patients. This does not mean the treatment caused suicidal thinking — the study design makes causation impossible to determine — but it means the question needs to be answered before that particular target is used widely.
Your realistic timeline for getting focused ultrasound treatment
If you want to schedule an appointment, you cannot — not yet. But the gap between "experimental" and "available" may be narrower than you would guess for something this new.
Right now, focused ultrasound for depression is only approved in one country: South Korea. That approval exists within the South Korean National Health Insurance System. No other country has approved LIFU for any psychiatric indication. The BrainSonix Pulsar device used in the major trials is classified as an unapproved/uncleared device by the FDA — it can be used in registered clinical trials but not in clinical practice.

The path from current trials to clinical availability follows a predictable — if frustratingly slow — sequence. The existing trials (Fonzo's work, the UCLA ILIAD study, Philip's VA trial) are Phase 0 and Phase 1/2 equivalent studies. They establish safety, demonstrate target engagement, and provide initial efficacy signals. What comes next is larger, multi-site randomized controlled trials — the kind that regulatory agencies require before approving a device or treatment for widespread use. Those trials take years to design, fund, enroll, complete, and publish.
There are factors that could accelerate this. The technology builds on existing ultrasound physics already used in FDA-approved applications — high-intensity focused ultrasound is cleared for essential tremor and Parkinson's tremor, meaning the regulatory pathway is not entirely novel. The 2024 FUS-PULSE symposium produced a roadmap document specifically for psychiatric applications, which helps coordinate research efforts and regulatory strategy.
The hardware is also evolving in the direction of accessibility. Current trials typically require MRI guidance, which limits treatment to facilities with MRI scanners and adds cost. But researchers in the scoping review note that LIFU could evolve to a TMS-like outpatient treatment delivered with neuronavigation alone — no MRI required for each session. A structural MRI at intake for targeting, followed by neuronavigation-guided sessions in a clinic, would dramatically reduce cost and expand access. Separately, wearable LIFU devices operating at 30-150 mW/cm2 have been developed, with some functioning as IoT devices that allow remote physician control via mobile apps.
A realistic assessment: clinical availability in the United States for depression or anxiety through an approved device is unlikely before 2029 at the earliest, and that estimate assumes larger RCTs begin soon and produce positive results. If the trials underway right now confirm what the early data suggests — that this technology safely reduces symptoms across multiple psychiatric conditions — the pressure to approve and deploy it will be substantial. The unmet need is enormous: roughly one-third of patients with major depression do not respond adequately to first-line treatments. LIFU is not competing with treatments that already work for everyone. It is filling a gap.
Frequently Asked Questions
Is focused ultrasound the same as the ultrasound used during pregnancy?
They share the same underlying physics — both use sound waves above human hearing — but the applications are completely different. Diagnostic ultrasound (pregnancy scans) uses very low energy to create images. Low-intensity focused ultrasound for the brain uses higher energy concentrated at a precise focal point to modulate neural activity, though still far below the levels used in surgical ablation. The FDA safety limits for neuromodulatory ultrasound include a maximum intensity (ISPTA) of 720 mW/cm2 and mechanical index below 1.9.
Does focused ultrasound treatment hurt?
The treatment itself is not painful. Patients sit with a transducer pressed against their temple, sometimes held by a head strap. The most common side effects reported are mild — neck pain, sleepiness, slight headache, or itchiness at the transducer site — and these typically resolve within a few days. No anesthesia is required.
Can I get focused ultrasound treatment for depression right now?
Not through standard clinical care in most countries. South Korea is currently the only country where focused ultrasound for depression is approved and reimbursed through national health insurance. In the United States and elsewhere, LIFU for psychiatric conditions is only available through registered clinical trials. The Focused Ultrasound Foundation maintains an updated list of active trials on their website.
How is this different from transcranial magnetic stimulation (TMS)?
Both are non-invasive, but they work through different physics and reach different parts of the brain. TMS uses magnetic fields that induce electrical current in cortical tissue — the outer 2-4 centimeters of the brain. It cannot directly reach deep structures like the amygdala. LIFU uses acoustic energy that can penetrate to any depth with millimeter-scale precision. TMS is FDA-approved for depression and OCD; LIFU is still investigational for psychiatric use.
What psychiatric conditions might focused ultrasound eventually treat?
Clinical trials and early research span major depressive disorder, generalized anxiety disorder, PTSD, social anxiety, panic disorder, bipolar disorder, OCD, substance use disorders, and schizophrenia. Depression and anxiety have the most developed evidence base. The technology's ability to target specific brain circuits means different conditions could potentially be treated by adjusting which structure is targeted and how the ultrasound parameters are configured.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.