
Roughly a quarter of American women between 15 and 44 who use contraception rely on the pill. Millions more use patches, rings, implants, or injections. Yet many of them learn about the real trade-offs only after side effects show up — and at that point, the information they find online is either dismissive ("just give it three months") or terrifying ("it'll ruin your hormones forever"). Neither extreme is useful. This guide sits in the middle, using the largest and most recent clinical data to explain what hormonal contraceptives actually do inside your body, which side effects are backed by strong evidence, and which fears are overblown.
How Hormonal Contraceptives Work Inside Your Body
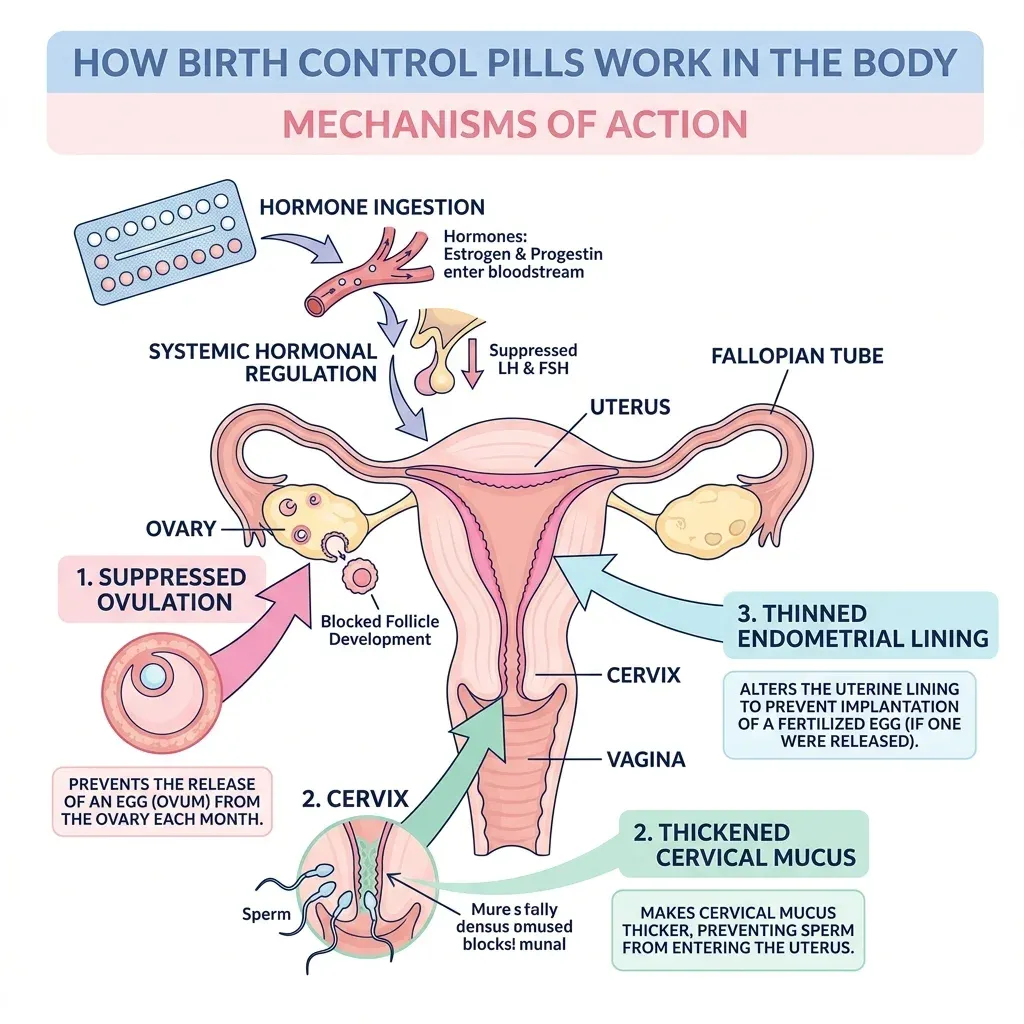
Every hormonal contraceptive on the market uses one of two approaches: a combination of synthetic estrogen and progestin, or progestin alone. Understanding the difference matters because it determines which side effects you're likely to experience.
Combined methods (most pills, the patch, the vaginal ring) deliver both estrogen and progestin. Their primary job is shutting down ovulation by suppressing FSH and LH, the two pituitary hormones that trigger egg release each month. Without that hormonal surge, no egg matures or leaves the ovary. As a backup, these methods also thicken cervical mucus (making it harder for sperm to reach the uterus) and thin the uterine lining.
Progestin-only methods (the mini-pill, hormonal IUDs, the implant, the injection) work differently depending on the dose. Higher-dose options like the injection suppress ovulation reliably. Lower-dose options like the hormonal IUD primarily thicken cervical mucus and thin the endometrium — some cycles still produce an egg, but the other barriers prevent pregnancy.
Quick fact: With perfect use, hormonal contraceptives prevent pregnancy in more than 99% of cases. Typical real-world use drops that to about 91-96%, mostly because people miss doses or refill prescriptions late. The method itself rarely fails — human behavior does.
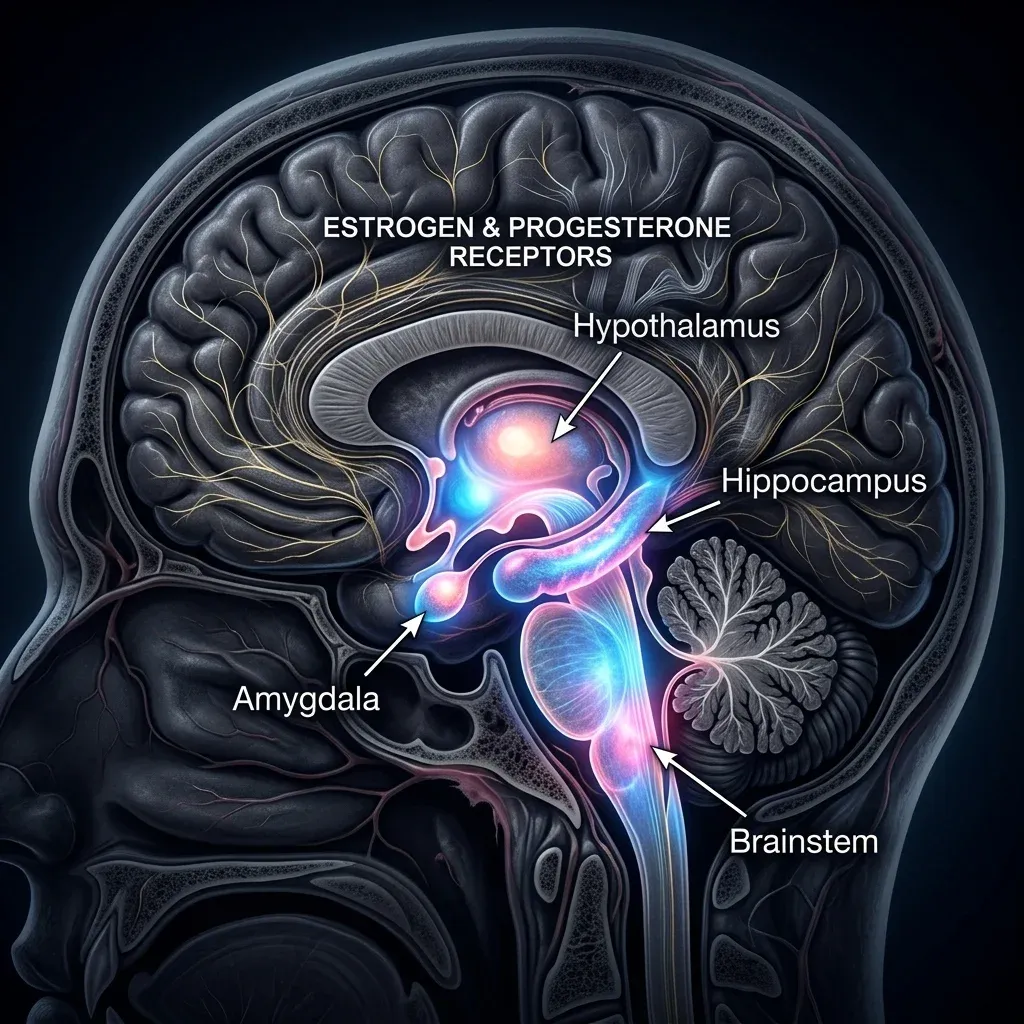
These hormones don't just affect the reproductive system. Estrogen receptors exist throughout the brain — in the hypothalamus, hippocampus, amygdala, and brainstem. Progesterone receptors cluster in the amygdala, cerebellum, cortex, and hippocampus. So when you flood the body with synthetic versions of these hormones while simultaneously flattening the natural monthly cycle, effects ripple far beyond the uterus. That's the biological foundation for everything discussed in the rest of this guide.
The Most Common Side Effects and Why They Happen
If you've started hormonal birth control and noticed changes within the first few months, you're not imagining things — and you're far from alone. A cross-sectional study of 1,699 women found that 79.2% of oral contraceptive users reported at least one negative side effect. The majority of users experience at least one.
The data on the most frequently reported issues breaks down like this:
| Side Effect | Reported Prevalence | Typical Timeline |
|---|---|---|
| Mood swings | 58.4% | First 1-3 months, may persist |
| Decreased libido | 51.1% | Gradual onset, often persistent |
| Depressed mood | 41.9% | First 6 months, variable |
| Breakthrough bleeding | Most frequent physical complaint | First 3 months, usually resolves |
| Headaches | Common | First 1-3 months |
| Breast tenderness | Common | First 1-3 months, usually resolves |
| Nausea | Common | First 1-3 months, usually resolves |
The physical side effects — breakthrough bleeding, headaches, nausea, breast tenderness — typically emerge in the first one to three months as your body adjusts to the new hormonal environment. ACOG notes these are generally minor and often resolve without intervention. Breakthrough bleeding is the single most common physical complaint and is triggered by the endometrial lining adjusting to continuous progestin exposure rather than the natural ebb and flow of hormones.
But the psychological side effects — mood swings, depressed mood, reduced sex drive — don't always follow that "wait three months" trajectory. Some persist for the entire duration of use. And in the same study, 45.3% of women eventually discontinued their pills specifically because side effects were intolerable. That statistic deserves more attention than it gets, because it suggests the standard advice to just power through isn't working for nearly half of users.
Age plays a role, too. Women under 25 reported side effects at rates above 80%, compared to 75% in older users. This isn't surprising when you consider that younger women's endocrine systems are still fine-tuning their natural hormone patterns, making them more sensitive to synthetic disruption.
The flip side is real, though: 97.1% of those same women reported at least one positive effect — regular cycles (74.1%), reduced menstrual pain (65.4%), and less stress (64.6%). Birth control side effects are a trade-off, not a one-sided negative.
Mood, Mental Health, and the Pill: What Large Studies Found
For years, women who reported feeling depressed or emotionally flat on birth control were told it was "probably something else." The research now shows otherwise — though the picture is more nuanced than either camp typically presents.
A landmark Danish study that followed over one million women found that hormonal contraceptive users had a measurably higher rate of first-time antidepressant use and new depression diagnoses compared to non-users. The effect was strongest among adolescents. A 2025 review in the Open Access Journal of Contraception analyzing a decade of research (2014-2024) confirmed that "younger/adolescent users and those who have used HCs for a short duration have the most elevated risks of depression following HC onset," with risk peaking around six months after first use.
The mechanism appears to involve two separate pathways. First, hormonal contraceptives suppress the natural mid-cycle surge of estrogen that normally produces a brief mood lift around ovulation. Flattening the cycle means flattening that peak. Second, research from Australian Prescriber shows that synthetic progesterone (progestin) elevates monoamine oxidase concentrations in the brain, which breaks down serotonin faster. Less serotonin available means a higher vulnerability to low mood. Meanwhile, natural estrogen is actually neuroprotective — it supports serotonin, dopamine, and noradrenaline activity. Replacing it with synthetic estrogen doesn't fully replicate those benefits.
Not all methods affect mood equally. The same 2025 review noted that "non-oral and progestin-only options carried higher depression risks compared to combined oral contraceptives in some populations." Injectable medroxyprogesterone acetate (the shot) appears to carry the highest mood risk among progestin-only methods, likely because it delivers a large bolus of synthetic hormone every three months with no estrogen to buffer the neurochemical effects.
| Contraceptive Method | Depression Risk Profile | Key Consideration |
|---|---|---|
| Combined oral pill | Moderate (varies by formulation) | Newer estradiol-based pills may have lower mood impact |
| Progestin-only pill | Moderate to high | No estrogen buffer for serotonin protection |
| Hormonal IUD | Low to moderate | Lower systemic hormone exposure |
| Injectable (Depo-Provera) | Higher | High-dose progestin, no estrogen, quarterly dosing |
| Implant | Moderate | Progestin-only, steady release |
There's an important caveat: some women experience less mood variability on hormonal contraceptives. For those with severe premenstrual dysphoric disorder (PMDD), the pill can actually function as an antidepressant by eliminating the wild hormonal swings that trigger depressive episodes. The 2025 review acknowledged that "some contraceptives also appear to decrease depression risk in some instances." Hormonal birth control restructures neurochemistry. Whether that restructuring helps or hurts depends on individual brain chemistry.
What the evidence does clearly support: if you develop new depressive symptoms within the first six months of starting hormonal contraception, the contraception is a legitimate suspect. Clinical guidelines now recommend monitoring mood closely during the first 3 to 24 months of use.
Blood Clot Risk: Separating Real Danger From Overblown Fear
Blood clots generate the most fear of any contraceptive side effect, and the numbers are frequently quoted without enough context.
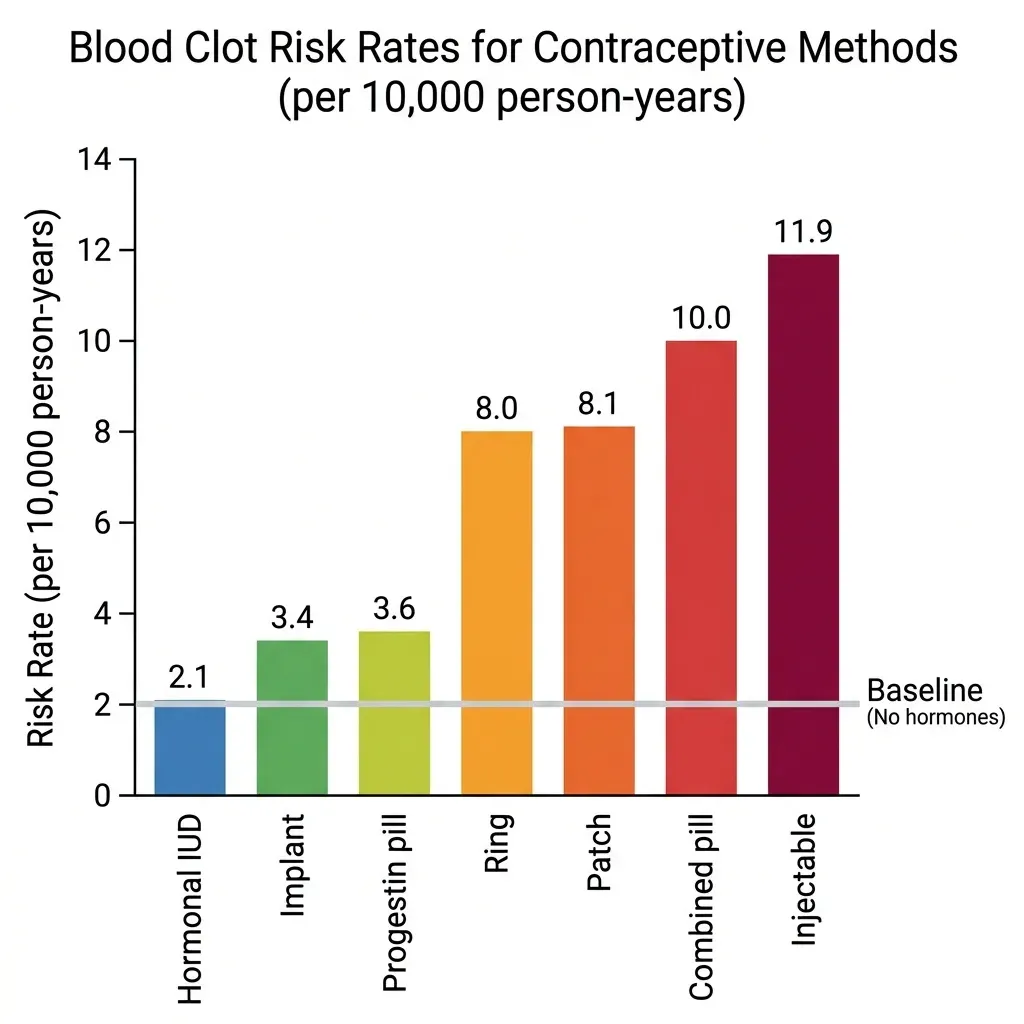
A 2025 Danish cohort study published in JAMA tracked 1,397,235 women aged 15 to 49 over 8.4 million person-years. It measured venous thromboembolism (VTE) — blood clots in deep veins or the lungs — across every major hormonal contraceptive type. The baseline VTE rate for women using no hormonal contraception was 2.0 per 10,000 person-years.
| Contraceptive Method | VTE Rate (per 10,000 person-years) | Risk vs. No Hormones |
|---|---|---|
| No hormonal use | 2.0 | 1.0x (baseline) |
| Hormonal IUD | 2.1 | 1.0x |
| Progestin-only pill | 3.6 | 1.8x |
| Implant | 3.4 | 1.7x |
| Vaginal ring | 8.0 | 4.0x |
| Patch | 8.1 | 4.1x |
| Combined oral pill | 10.0 | 4.6x |
| Injectable | 11.9 | 5.7x |
A 4.6-fold increase sounds alarming — until you anchor it in absolute numbers. Going from 2 events per 10,000 to 10 events per 10,000 means 8 additional women out of every 10,000 will experience a VTE per year. That's a 0.08% annual absolute risk. For comparison, the VTE risk during pregnancy and the postpartum period runs substantially higher than any contraceptive method on this list.
The type of progestin matters significantly. Third-generation progestins (desogestrel and gestodene) carried the highest excess risk — 14.2 additional VTE events per 10,000 person-years. The lowest-risk combined option was a pill containing 20 micrograms of estrogen with levonorgestrel, showing only about 3 extra events per 10,000 person-years. The StatPearls clinical reference identifies formulations with 30 micrograms of estrogen plus levonorgestrel as the safest combined option overall.
The hormonal IUD stands out: its VTE rate of 2.1 per 10,000 is statistically indistinguishable from using no hormones at all. That's because the IUD delivers progestin locally to the uterus with minimal systemic absorption. If clot risk is your primary concern, this is the hormonal method with the best safety profile by a wide margin.
Who needs to be especially careful: The FDA flags specific risk factors — smoking over age 35, personal or family history of clots, known thrombogenic mutations (like Factor V Leiden), migraine with aura, and uncontrolled hypertension above 140/90. If any of these apply, combined hormonal methods are contraindicated. Progestin-only options or the copper IUD are the standard alternatives.
Weight, Skin, and Libido: Three Changes Nobody Warns You About
These are the three side effects that dominate online forums and rarely get straight answers in a clinical setting.
Weight: Fear of weight gain is the number-one concern women express about starting the pill — 74% in one survey cited it as their top worry. Controlled research tells a different story: clinical data indicates the pill does not cause weight gain. Randomized controlled trials comparing pill users to placebo groups consistently find no significant difference in weight. Some women retain a small amount of water in the first few months due to estrogen's effect on fluid balance, but this is transient and not the same as gaining body fat. The injectable (Depo-Provera) is the one exception — it has been associated with modest weight gain in some studies, likely due to its appetite-stimulating properties at high progestin doses.
Skin: Many combined pills actually improve acne, which is one of their most well-documented non-contraceptive benefits. The estrogen component suppresses androgen activity, reducing sebum production. That's why some formulations (particularly those containing drospirenone or norgestimate) are specifically FDA-approved for acne treatment. However, progestin-only methods can occasionally worsen acne in some women, since certain progestins have mild androgenic activity. If clear skin is a priority, a combined pill is the better bet — but switching methods can cause temporary breakouts during the hormonal transition.
Libido: Reduced sex drive is real, common, and under-discussed. The Polish survey found 51.1% of users reported decreased sexual desire, making it the second most common complaint after mood changes. The mechanism is straightforward: combined pills increase sex hormone-binding globulin (SHBG), which binds to free testosterone and reduces the amount available to drive libido. Research on the psychobehavioral effects of hormonal contraceptives confirmed that "women using HCs report higher rates of depression, reduced sexual functioning compared to naturally-cycling women." SHBG levels can remain elevated even after stopping the pill, though they typically normalize within a few months.
What makes these three side effects particularly frustrating is the mismatch between clinical messaging and lived experience. Weight gain fears are often dismissed entirely (reasonably, based on the data), but that dismissal can make women feel unheard about the other changes they're experiencing. Libido loss is real and measurable, yet it rarely appears in the brief counseling that accompanies a new prescription.
Long-Term Effects on Fertility, Bone Density, and Cancer Risk
Fertility: One of the most persistent myths about the pill is that it causes lasting infertility. It doesn't. The WHO states explicitly that oral contraceptives "do not cause infertility." Clinical data backs this up: 97% of women had spontaneous menses within 90 days of discontinuing combined oral contraceptives. Some women experience a brief delay — particularly after long-acting methods like the injection, where return to ovulation can take 6 to 12 months — but this represents a delay, not permanent damage. The pill simply pauses your natural cycle; it doesn't erase it.
Bone density: This concern is specific to one method: Depo-Provera (the injectable). It suppresses estrogen levels enough to measurably reduce bone mineral density during use, similar to the bone-thinning effect seen in menopause. The good news is that bone density recovers after discontinuation in most women. Combined pills, by contrast, maintain sufficient circulating estrogen and don't appear to negatively affect bone density. The hormonal IUD and implant also show no significant bone impact.
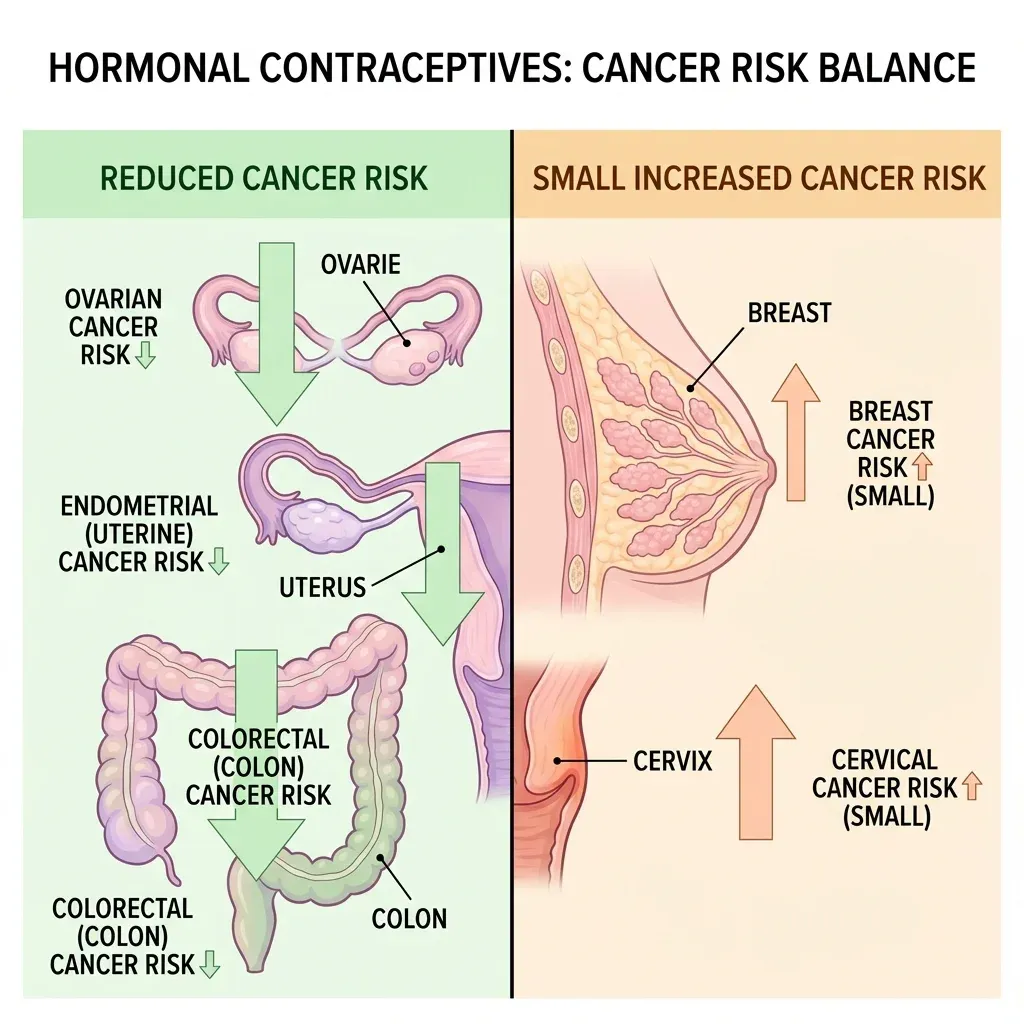
Cancer: The cancer picture is mixed. Hormonal contraception offers measurable protection against some cancers while slightly increasing the risk of others.
| Cancer Type | Effect of HC Use | Data Source |
|---|---|---|
| Endometrial cancer | 50% risk reduction (lasts 20+ years after stopping) | StatPearls/NCBI |
| Ovarian cancer | 27% risk reduction (increases with longer use) | StatPearls/NCBI |
| Colon cancer | 18% risk reduction | StatPearls/NCBI |
| Breast cancer | Relative risk 1.20 vs. never-users | ACOG / Danish cohort study |
| Cervical cancer | Higher risk with long-term use | WHO |
The breast cancer numbers need context. ACOG's analysis of the 2017 Danish cohort study found that the relative risk of 1.20 translates to 1 additional case of invasive breast cancer for every 7,690 women using hormonal contraception. For women under 35, that drops to 1 additional case per 50,000 users. The risk increases with duration — from RR 1.09 for less than one year to RR 1.38 for over ten years — but the absolute numbers remain small. Meanwhile, the protective effects against endometrial and ovarian cancer are substantially larger in magnitude and last decades after discontinuation.
Women with BRCA1 or BRCA2 mutations face a different calculus. The WHO notes these carriers "may have a higher risk" with long-term hormonal contraceptive use, and this is a conversation that warrants genetic counseling, not a blanket recommendation.
Myth vs. Fact: What Hormonal Birth Control Actually Does
| Myth | Fact | Evidence |
|---|---|---|
| "The pill makes you gain weight" | Randomized trials show no significant weight gain from combined pills. Water retention in early months is temporary. | Cleveland Clinic clinical review |
| "Birth control causes infertility" | 97% of women resume menstruation within 90 days. WHO confirms no infertility link. | WHO fact sheet; StatPearls |
| "All pills have the same clot risk" | Risk varies 3-fold between formulations. Low-dose levonorgestrel pills have the lowest combined-pill VTE risk. | JAMA 2025 (Yonis et al.) |
| "Mood changes are just in your head" | Large-scale studies document increased antidepressant use and depression diagnoses in HC users, especially adolescents. | Danish cohort of 1M+ women; 2025 review |
| "You need to take a break from the pill" | No medical reason to cycle off. Continuous use is safe long-term. | ACOG clinical guidance |
| "The hormonal IUD is just as risky as the pill" | The IUD has a VTE rate statistically identical to using no hormones (2.1 vs 2.0 per 10,000). | JAMA 2025 (Yonis et al.) |
Frequently Asked Questions
How long do birth control side effects last after starting?
Physical side effects like breakthrough bleeding, nausea, and breast tenderness typically resolve within the first three months. Mood-related side effects are less predictable — some improve as your body adjusts, while others persist for the duration of use. If side effects haven't improved after three months, that's a reasonable time to talk to your prescriber about switching formulations or methods.
Does the pill increase my risk of blood clots enough to worry about?
For most healthy, non-smoking women under 35, the absolute risk is small: roughly 8 extra VTE events per 10,000 users per year for combined pills. That said, the risk is real and higher with certain formulations. If you have additional risk factors (smoking, family history of clots, migraine with aura), your prescriber should discuss progestin-only or non-hormonal alternatives.
Can I take birth control pills long-term without health consequences?
Yes, for most women. The WHO and ACOG both confirm that long-term use is safe, and the protective effects against endometrial and ovarian cancer actually increase with longer use. The main considerations for very long-term use are the small cumulative increase in breast cancer risk (which returns to baseline after stopping) and the importance of periodic blood pressure monitoring.
Will stopping birth control cause a hormonal crash?
Some women experience temporary irregular cycles, acne flares, or mood shifts after stopping — often called "post-pill syndrome" in wellness spaces, though it's not a recognized medical diagnosis. What's actually happening is your hypothalamic-pituitary-ovarian axis restarting after being suppressed. Most women's cycles normalize within one to three months, and 97% menstruate within 90 days.
Which hormonal contraceptive has the fewest side effects overall?
The hormonal IUD consistently shows the mildest systemic side effect profile because it delivers progestin locally with minimal absorption into the bloodstream. Its VTE risk matches non-use, it doesn't appear to affect mood as strongly as systemic methods, and it doesn't suppress ovulation in most users. The trade-off is that insertion can be painful and some women experience irregular spotting in the first few months.
Related Articles
- Hormone Replacement Therapy (HRT) — Benefits, Risks, and Modern Evidence — A deep look at exogenous hormones later in life and how the risk-benefit calculus shifts after menopause.
- Estrogen Dominance: Symptoms, Causes, and How to Rebalance Naturally — What happens when estrogen gets out of proportion with progesterone, and lifestyle strategies that help.
- Perimenopause Symptoms and Natural Management Strategies — For women transitioning off contraception later in reproductive life, this covers what to expect.
- PCOS Natural Management — Diet, Supplements, and Lifestyle — Since the pill is frequently prescribed for PCOS, this guide covers what works alongside or instead of hormonal treatment.
- Seed Cycling for Hormone Balance — Does It Work? — An evidence-based look at this popular natural approach to supporting hormonal cycles.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











