Best Anti-Aging and Anti-Wrinkle Remedies
Best Anti-Aging and Anti-Wrinkle Remedies: The Evidence-Based Ultimate Guide

Most anti-aging advice online falls into two extremes. One side says wrinkles are inevitable and products are mostly marketing. The other says the right serum stack can erase a decade. Neither is accurate. The evidence is more practical: some interventions reliably slow visible skin aging, some produce modest improvements, and many are expensive distractions.
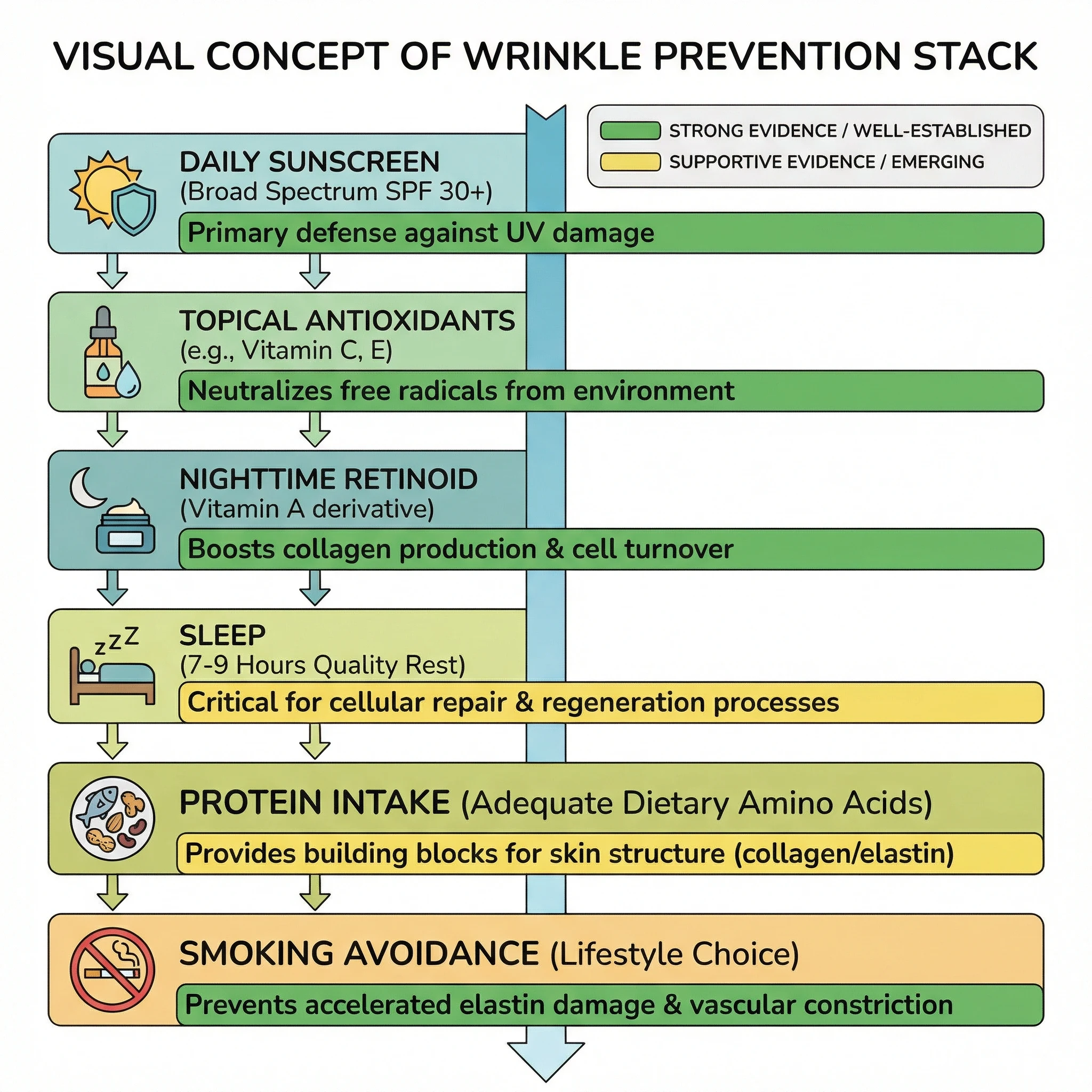
If you want the shortest version first, here it is. Daily sunscreen is foundational. Retinoids have the strongest topical evidence for photoaging. Vitamin C and niacinamide can help, but they are supporting players, not magic leads. Procedures can accelerate cosmetic change, but they do not replace long-term skin-health habits. Sleep, smoking status, and sun exposure patterns influence results more than product hype.
This guide focuses on what high-quality evidence actually supports, where uncertainty still exists, and how to build a routine that is boring enough to sustain for years. You will also see where common myths keep people spending heavily with little return. If you want broader UV protection context, these related guides can help: remedies for sun and UV skin damage, natural sunscreen options, and summer skin-protection habits.
Quick fact: The most reliable anti-wrinkle strategy is prevention plus consistency, not aggressive product cycling.
A 2013 randomized trial showed daily sunscreen slowed visible skin aging
When people ask for the single highest-return anti-aging habit, sunscreen is the answer. In the Nambour randomized trial, participants assigned to daily broad-spectrum sunscreen developed less detectable photoaging over time than those using sunscreen at their discretion (Green et al., Annals of Internal Medicine, 2013). That finding matters because it comes from prospective randomized evidence, not only laboratory mechanisms.
Sun exposure drives collagen breakdown through ultraviolet-induced oxidative stress and matrix remodeling. You may not notice this daily, but cumulative exposure creates the classic pattern: uneven tone, roughness, fine lines that become fixed lines, and texture changes around high-exposure zones like forehead, periorbital skin, and upper cheeks. Public-health guidance from CDC and MedlinePlus aligns with this: broad sun protection is not just skin-cancer prevention, it is also visible-aging prevention.
The practical problem is under-dosing. People often apply too little sunscreen, skip reapplication, or only wear it during intense summer sun. Aging biology does not care about seasons. Repeated low-dose exposure still accumulates. If you spend time outdoors daily, your anti-aging routine is only as good as your UV protection habits.
| Intervention | Evidence quality for wrinkle prevention | Typical real-world mistake | What to do instead |
|---|---|---|---|
| Daily broad-spectrum sunscreen | High relative to other topical prevention steps | Applying only on sunny beach days | Use daily on exposed skin, year-round |
| Protective clothing and shade timing | Strong mechanistic and public-health support | Relying on sunscreen alone for long exposure | Combine sunscreen with hats, shade, and timing |
| After-sun products | Low for true long-term prevention | Using after-sun care as primary strategy | Treat after-sun care as recovery, not prevention |
Why wrinkles form even in people with expensive routines
Wrinkles are not a single process. They are the visible endpoint of multiple biological changes happening at once: lower collagen synthesis, altered elastin architecture, reduced barrier resilience, repetitive facial movement, glycation stress, and external insults like UV and smoking. Intrinsic aging progresses in everyone. Extrinsic aging can be accelerated or slowed.
This distinction matters because anti-aging products mainly target extrinsic damage and skin remodeling windows. They cannot stop chronological aging, but they can improve trajectory. That is why two people at the same age can look very different based on long-term exposure history. One can have deeper etched lines with mottled pigmentation; another can have finer textural change with better elasticity preservation.
Smoking is one of the clearest modifiable accelerators. Twin-based evidence has linked smoking burden to greater facial aging and wrinkle severity (Okada et al., Plastic and Reconstructive Surgery, 2013). Earlier epidemiologic work also demonstrated additive effects between UV exposure and smoking on wrinkling risk (Ernster et al., Journal of the American Academy of Dermatology, 1995). For skin aging, smoking cessation is not a side recommendation. It is core treatment.
Sleep quality also matters more than many routines acknowledge. In a clinical study, poor sleepers showed signs of increased skin aging and slower barrier recovery (Oyetakin-White et al., Clinical and Experimental Dermatology, 2015). That does not mean sleep is a topical substitute. It means skin-repair biology is systemic, and product-only plans can plateau if sleep, stress, and behavior remain misaligned.
Retinoids remain the strongest topical remedy, but dose and tolerance decide success

Among over-the-counter and prescription topicals, retinoids consistently show the strongest anti-photoaging signal. Classic randomized trials demonstrated visible improvement in fine wrinkling and dermal matrix features with tretinoin use (Kligman et al., Journal of the American Academy of Dermatology, 1986). More recent reviews and meta-analyses support retinoid efficacy across photoaging outcomes, though differences exist by molecule, concentration, and tolerability profile.
Why retinoids work is straightforward: they influence keratinocyte turnover, collagen-related pathways, and epidermal organization over time. Why people fail on retinoids is equally straightforward: irritation, overuse, and inconsistent adherence. Many users start too aggressively, trigger barrier disruption, and abandon treatment before benefits appear.
A defensible approach is low-and-slow titration: two to three nights weekly at first, moisturizer support, and gradual increase as tolerated. Expect visible change in texture and fine lines over months, not days. If stinging, scaling, or persistent inflammation appears, stepping down frequency is usually better than quitting entirely.
| Retinoid strategy | Expected benefit window | Main tradeoff | Practical recommendation |
|---|---|---|---|
| Prescription tretinoin | Often strongest wrinkle/photoaging outcomes | Higher irritation potential | Medical supervision plus gradual initiation |
| Over-the-counter retinol | Moderate improvement with sustained use | Slower onset | Consistent nightly tolerance building |
| Short-cycle aggressive use | Usually poor due to dropout | Barrier damage and rebound sensitivity | Avoid intensity spikes; prioritize adherence |
Pregnancy planning changes risk tolerance. Clinical guidance from ACOG advises discussing retinoid exposure with your obstetric clinician and avoiding assumptions that all topical forms are automatically acceptable. If pregnancy is possible or planned, that conversation should happen before building a retinoid-centered routine.
Can vitamin C, niacinamide, and moisturizers actually move the needle?
Yes, but expectations must stay proportional. Vitamin C has biologic plausibility and clinical support for pigmentation and photodamage-related parameters in selected formulations. A 2023 systematic review found topical vitamin C can improve signs of photoaging, while also noting heterogeneity across studies and product compositions (de la Garza et al., Journal of Drugs in Dermatology, 2023).
Niacinamide also has meaningful supporting evidence. A double-blind randomized trial reported improvement in multiple facial-aging measures with topical niacinamide over 12 weeks (Bissett et al., Dermatologic Surgery, 2005). This is useful because niacinamide tends to be better tolerated than many actives and can fit sensitive-skin routines.
Moisturizers do not rebuild deep dermal architecture the way people imagine, but they can visibly reduce the appearance of fine lines by improving hydration, barrier function, and optical smoothness. For many adults, better barrier support is what allows continued use of evidence-based actives like retinoids without chronic irritation.
The highest-yield stack for most people is simple: morning broad-spectrum sunscreen plus antioxidant support, evening retinoid as tolerated, and barrier moisturizer both times. That approach usually beats ten-product routines with inconsistent use and frequent irritation resets.
Myth vs fact: the anti-wrinkle claims that waste money fastest
| Myth | Fact | Evidence direction |
|---|---|---|
| "Natural oils can replace sunscreen for wrinkle prevention." | No oil has equivalent evidence to daily broad-spectrum sunscreen for photoaging prevention. | Contradicted by prevention trials and public-health guidance |
| "If a product burns, it is working better." | Persistent irritation usually harms adherence and can worsen barrier health. | Supported by routine dermatology practice and retinoid tolerability data |
| "Collagen supplements erase established wrinkles." | Meta-analyses suggest modest improvements in hydration/elasticity in some groups, not dramatic reversal. | Promising but moderate-effect evidence |
| "You can out-serum poor sleep and smoking." | Behavioral drivers materially change skin-aging trajectory and response quality. | Supported by clinical and epidemiologic studies |
| "Expensive means clinically superior." | Formula, concentration, and adherence matter more than luxury branding. | Consistent with comparative dermatology outcomes |
Marketing language often blurs improvement categories. "Radiance" and "plumpness" can improve quickly through hydration. Structural wrinkle change usually requires longer timelines and better evidence-backed mechanisms. Distinguishing those endpoints helps avoid unnecessary product churn.
Dermatologist procedures and at-home care are not rivals, they are layers
At-home care and in-office procedures answer different questions. Topicals and habits shape long-term trajectory. Procedures can accelerate visible change for specific concerns such as dynamic lines, texture irregularity, pigment burden, or volume loss. Problems arise when people expect one category to replace the other.
For example, injectable neuromodulators target expression-related dynamic lines and often produce faster cosmetic change than skincare alone. Energy-based devices and resurfacing can improve texture and dyschromia, but they still require ongoing photoprotection and maintenance. Without maintenance, recurrence is predictable.
If budget is limited, the usual evidence-informed order is prevention and foundational topical care first, targeted procedures second. A patient who spends heavily on procedures but skips sunscreen and adherence often underperforms a patient with disciplined baseline habits and selective procedural escalation.
This is where clinical consultation pays off. A dermatologist can map whether your dominant issue is UV-associated texture, muscle-driven dynamic wrinkling, pigment, laxity, or inflammatory barrier instability. That diagnosis determines whether you need better routine design, prescription escalation, or procedure referral.
Before-and-after photos can mislead if you ignore timeline, lighting, and baseline risk
Many anti-wrinkle products look convincing online because images compress context. Lighting angle, makeup, camera distance, facial expression, and hydration state can create apparent \"results\" that are not structural change. Even honest marketers can accidentally overstate outcomes when photo conditions vary.
Clinically, useful tracking is simple and strict: same room, same time of day, no makeup, neutral expression, and identical camera distance every four weeks. Without this, you cannot tell whether your routine is working or whether you are seeing short-term optical shifts from hydration and lighting.
Baseline risk also changes interpretation. A 42-year-old with high cumulative UV exposure, irregular sleep, and active smoking may see slower gains than a 42-year-old with strong prevention habits. That is not product failure; it is biology plus exposure history. This is why personalized goals outperform generic promises like \"erase ten years in a month.\"
| Common tracking error | Why it distorts results | Better method |
|---|---|---|
| Different lighting between photos | Shadows can exaggerate or hide fine lines | Use the same location and lighting setup |
| Changing expression in comparison photos | Dynamic lines look worse with subtle muscle activation | Keep neutral face for baseline and follow-up |
| Weekly \"progress checks\" | Too short for true remodeling signal | Evaluate at 4-, 8-, and 12-week intervals |
| Adding multiple new actives at once | Impossible to identify what helps or harms | Introduce one major change at a time |
The 12-week routine that usually beats product hopping

Most anti-aging routines fail from inconsistency, not product insufficiency. A 12-week structure helps because it replaces impulse buying with measurable progression.
| Weeks | Primary goal | Core actions | How to judge progress |
|---|---|---|---|
| 1-2 | Barrier stabilization | Daily sunscreen, gentle cleanser, moisturizer, stop aggressive exfoliation | Less stinging, less visible dryness, no new irritation flares |
| 3-6 | Introduce remodeling | Add low-frequency retinoid nights, continue morning protection | Tolerable adaptation without persistent dermatitis |
| 7-10 | Supportive actives | Add vitamin C or niacinamide if tolerated, maintain consistent sunscreen dosing | Improved tone/texture, stable barrier, no routine overload |
| 11-12 | Reassess and personalize | Photographic comparison, adjust frequency, discuss prescription or procedure options if needed | Clear responder vs non-responder decision point |
Support behaviors matter during this phase. Hydration, sleep regularity, and smoking cessation improve the likelihood that topical therapy translates into visible change. If hydration habits are weak, this related guide can help structure basics: 11 ways to hydrate skin naturally.
Do not ignore mental load. If skin concerns begin driving compulsive mirror checking or social withdrawal, address that directly. Persistent appearance anxiety can overlap with mood symptoms, and support is warranted. For broader mental-health context, this article can be useful: depression and complementary health approaches.
When wrinkles are not the main issue and self-treatment should pause
Some presentations should trigger professional evaluation instead of more over-the-counter experiments: rapidly changing lesions, bleeding spots, non-healing patches, painful eruptions, severe persistent dermatitis after actives, sudden pigment shifts, or unilateral facial changes. Anti-aging routines should not delay diagnosis of potentially serious skin disease.
You should also seek clinician guidance if you have rosacea, eczema, melasma, or a history of post-inflammatory hyperpigmentation and want a retinoid-centered plan. These conditions are manageable, but strategy needs adaptation to reduce flare risk and avoid a cycle of irritation and abandonment.
In short, anti-wrinkle care is a long game. The goal is not maximal intensity. The goal is sustainable benefit with minimal harm.
Frequently Asked Questions
How long does it take to see wrinkle improvement from a good routine?
Many people notice hydration and texture improvement within a few weeks, but structural wrinkle change usually needs 8 to 24 weeks of consistent sunscreen and retinoid-centered care. Faster promises are usually cosmetic surface effects, not durable remodeling.
Is retinol enough, or do I need prescription tretinoin?
Retinol can work for many users, especially with good adherence and low irritation. Prescription tretinoin often has stronger data for photoaging, but tolerability and supervision matter. The better option is the one you can use consistently and safely.
Are collagen supplements worth adding for anti-aging?
Recent meta-analyses suggest possible moderate improvements in hydration and elasticity in some populations, but effects are not equivalent to sun protection plus retinoids. Supplements can be optional adjuncts, not core replacements.
Can I skip sunscreen if I mostly stay indoors?
If you receive meaningful daylight exposure through routine activity or windows, daily sunscreen remains a high-value prevention step. Indoor-only assumptions are often inaccurate in real life.
What if every active ingredient irritates my skin?
Start with barrier-first care, reduce frequency, and introduce one active at a time. If irritation persists, stop self-escalation and get clinician guidance. Ongoing inflammation can worsen outcomes and delay progress.
The bottom line most people need to hear
The best anti-aging and anti-wrinkle remedies are not mysterious. They are evidence-weighted habits done for years: daily broad-spectrum sun protection, retinoid use that your skin can tolerate, supportive actives with realistic expectations, and lifestyle choices that do not sabotage repair biology. Procedures can add speed and precision, but they do not replace fundamentals.
If your current routine is complex, expensive, and inconsistent, simplify first. A simple routine performed daily usually beats an advanced routine performed occasionally. In skin aging, consistency is a stronger predictor than novelty.
Sources
- Green AC et al. Reduced melanoma after regular sunscreen use: randomized trial follow-up (Ann Intern Med, 2013).
- Kligman AM et al. Topical tretinoin for photoaged skin (J Am Acad Dermatol, 1986).
- Mukherjee S et al. Topical tretinoin for treating photoaging: systematic review (Int J Dermatol, 2022).
- Park HJ et al. Efficacy and safety of topical tretinoin in photoaging: systematic review and meta-analysis (J Cosmet Dermatol, 2024).
- de la Garza E et al. Topical vitamin C and photoaging: systematic review (J Drugs Dermatol, 2023).
- Bissett DL et al. Topical niacinamide improves aging facial skin appearance: randomized controlled trial (Dermatol Surg, 2005).
- Pu SY et al. Oral collagen supplementation and skin aging: systematic review and meta-analysis of randomized controlled trials (Nutrients, 2023).
- Oyetakin-White P et al. Poor sleep quality and skin aging outcomes (Clin Exp Dermatol, 2015).
- Okada HC et al. Cigarette smoking and facial aging among twins (Plast Reconstr Surg, 2013).
- Ernster VL et al. Facial wrinkling in men and women by smoking and sun exposure (J Am Acad Dermatol, 1995).
- MedlinePlus. Aging changes in skin.
- MedlinePlus. Sun exposure.
- CDC. Sun Safety.
- ACOG. Skin Conditions During Pregnancy (retinoid counseling context).