Every Year, 800,000 Americans Have a Heart Attack — and Survivors Face a Grim Second Chapter
Surviving a heart attack feels like getting a second chance. But the numbers tell a sobering story: within five years of a first heart attack, roughly one in five survivors will experience a second cardiovascular event. That second event is often deadlier than the first, partly because the heart muscle has already been weakened and partly because the underlying conditions that triggered the initial attack rarely resolve on their own.
Standard secondary prevention — the medical term for preventing a repeat cardiac event — involves statins, blood thinners, blood pressure medications, and lifestyle modifications. These interventions have saved countless lives, but they leave a significant gap. Something between half and two-thirds of heart attack survivors still carry a risk factor that most cardiologists have only recently begun to measure with any urgency: insufficient vitamin D levels.
A randomized clinical trial presented at the 2025 American Heart Association Scientific Sessions has provided the first strong evidence that fixing this deficiency through a monitored, dose-adjusted approach can cut the risk of a second heart attack by half. The study, called TARGET-D, did not just hand patients a bottle of supplements. It tracked blood levels, adjusted doses, and pursued a specific therapeutic target — and that distinction turns out to be everything.
630 Patients, 8 Years, and a Finding That Redefines "Personalized" Supplementation
The TARGET-D trial, led by cardiovascular epidemiologist Heidi May, PhD, at Intermountain Health in Salt Lake City, enrolled 630 patients who had experienced a heart attack within the previous month. Enrollment ran from April 2017 to May 2023, and participants were followed through March 2025 for cardiovascular events.
Researchers split participants into two groups of roughly equal size. One group received standard care with no active management of their vitamin D levels. The other received what the researchers called "target-to-treat" vitamin D3 supplementation — a protocol designed to raise and maintain blood levels of 25-hydroxyvitamin D above 40 nanograms per milliliter (ng/mL).
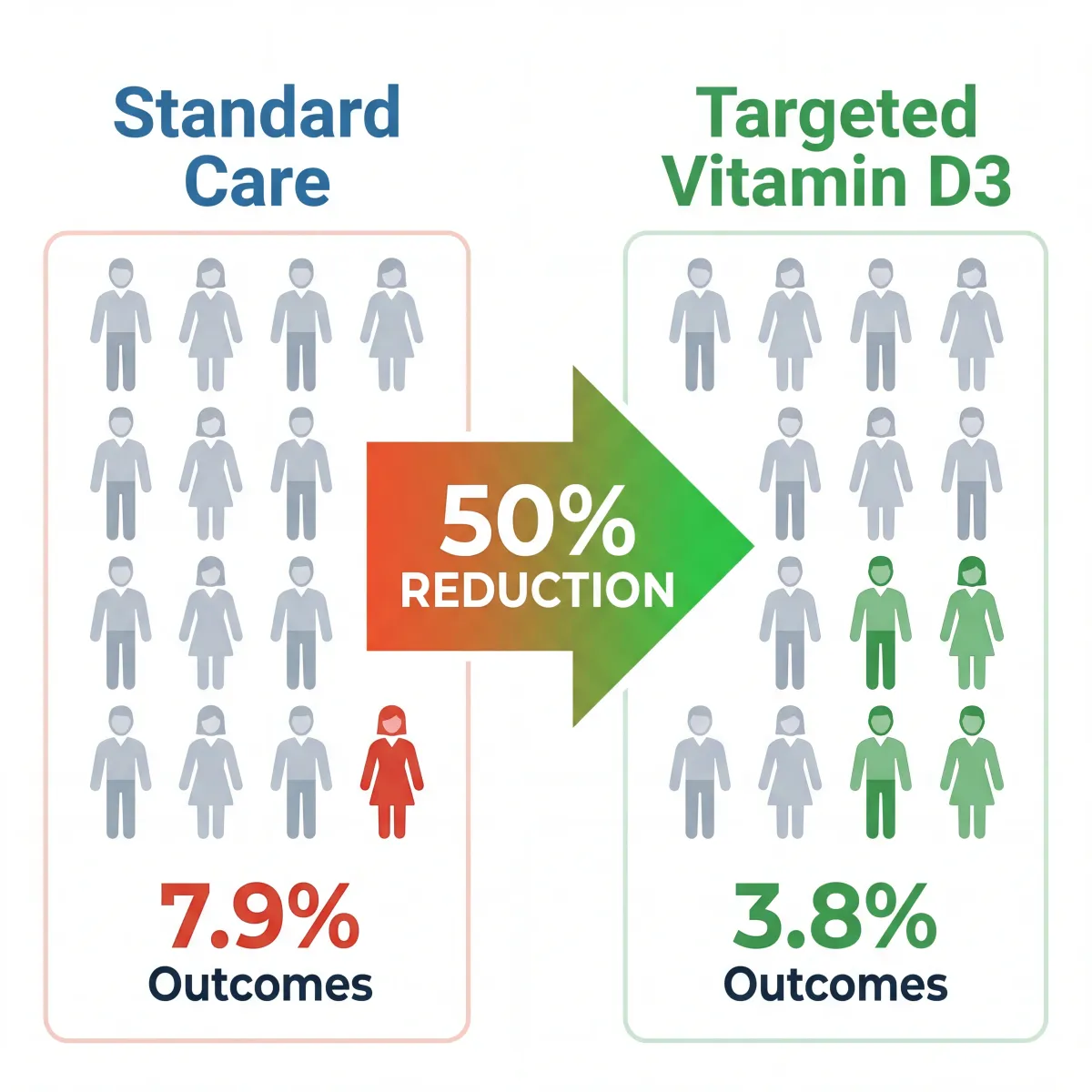
Key Finding: Heart attack survivors who received targeted vitamin D3 management experienced a recurrent heart attack rate of 3.8%, compared to 7.9% in the standard care group — a roughly 50% relative reduction in risk.
Here is what made this trial unique among vitamin D cardiovascular studies:
| Feature | TARGET-D Trial | Previous Vitamin D Trials |
|---|---|---|
| Population | Recent heart attack patients | Healthy general population |
| Dosing approach | Blood-level guided, dose adjusted | Fixed dose for everyone |
| Target blood level | >40 ng/mL (100 nmol/L) | No target specified |
| Monitoring frequency | Every 3 months until target, then annually | None or minimal |
| Starting dose range | Up to 5,000 IU/day (individualized) | 600-2,000 IU/day (fixed) |
| Result for MI prevention | ~50% reduction | No significant reduction |
Of the 630 trial participants, 107 experienced a major adverse cardiovascular event (MACE) — a composite that includes heart attack, stroke, heart failure hospitalization, or death. When researchers looked at MACE overall, they found no significant difference between the groups. But when they isolated recurrent heart attacks specifically, the vitamin D3 group showed a dramatic reduction: 3.8% versus 7.9%, which represents roughly half the risk.
The finding carries an important nuance. Vitamin D3 supplementation did not appear to prevent strokes or heart failure hospitalizations in this trial. Its protective effect was specific to preventing another heart attack — and that specificity actually strengthens the finding, because it suggests a targeted biological mechanism rather than a vague "general health" benefit.
Decades of Null Results Had One Critical Flaw
Before TARGET-D, the medical consensus was clear: vitamin D supplements do not prevent heart disease. That conclusion was based on multiple large, well-designed trials that collectively enrolled over 100,000 participants and consistently found no cardiovascular benefit from supplementation.
The largest of these, the VITAL trial published in the New England Journal of Medicine, randomized 25,871 healthy Americans to either 2,000 IU of vitamin D3 per day or placebo. After 5.3 years, the hazard ratio for major cardiovascular events was 0.97 — statistically indistinguishable from no effect at all. A 2022 meta-analysis of 18 randomized controlled trials involving 70,278 participants reached the same conclusion.
So why did TARGET-D find a benefit when these massive trials did not? Three critical design differences explain the discrepancy:
| Factor | Previous Trials (e.g., VITAL) | TARGET-D |
|---|---|---|
| Baseline vitamin D status | Many participants already sufficient | 85% had levels below 40 ng/mL |
| Dosing strategy | Same dose regardless of blood level | Dose titrated to achieve >40 ng/mL |
| Study population | Healthy people (primary prevention) | Recent heart attack survivors (secondary prevention) |
The Finnish Vitamin D Trial illustrates this problem with particular clarity. That 5-year study of 2,495 older adults found no cardiovascular benefit from supplementation — but the average baseline vitamin D level was already 75 nmol/L (30 ng/mL), well above the deficiency threshold. You cannot demonstrate a benefit from correcting a deficiency in people who are not deficient.
As a 2025 narrative review in Nutrients put it, the failure of randomized controlled trials to show cardiovascular benefit was largely due to "faulty study designs, such as enrolling participants with baseline 25(OH)D levels above 50 nmol/L." TARGET-D addressed this by enrolling patients who overwhelmingly had insufficient levels and then actively managing their supplementation to reach a therapeutic target.
Your Heart Has Vitamin D Receptors — and After a Heart Attack, They Matter
The finding that vitamin D3 specifically reduces recurrent heart attacks (but not strokes or heart failure) makes more biological sense than a generic cardiovascular benefit. The heart muscle itself contains vitamin D receptors, and these receptors become particularly relevant after an infarction damages the tissue.
Animal research has demonstrated that active vitamin D (1,25-dihydroxyvitamin D3) directly improves cardiac function after myocardial infarction. In a study published in Heart, Lung and Circulation, mice treated with active vitamin D after induced heart attacks showed less ventricular wall thinning and significantly better systolic function compared to untreated controls. The mechanism appears to involve modulation of cardiac progenitor cells — vitamin D slowed problematic cell proliferation and reduced expression of pro-fibrotic factors.
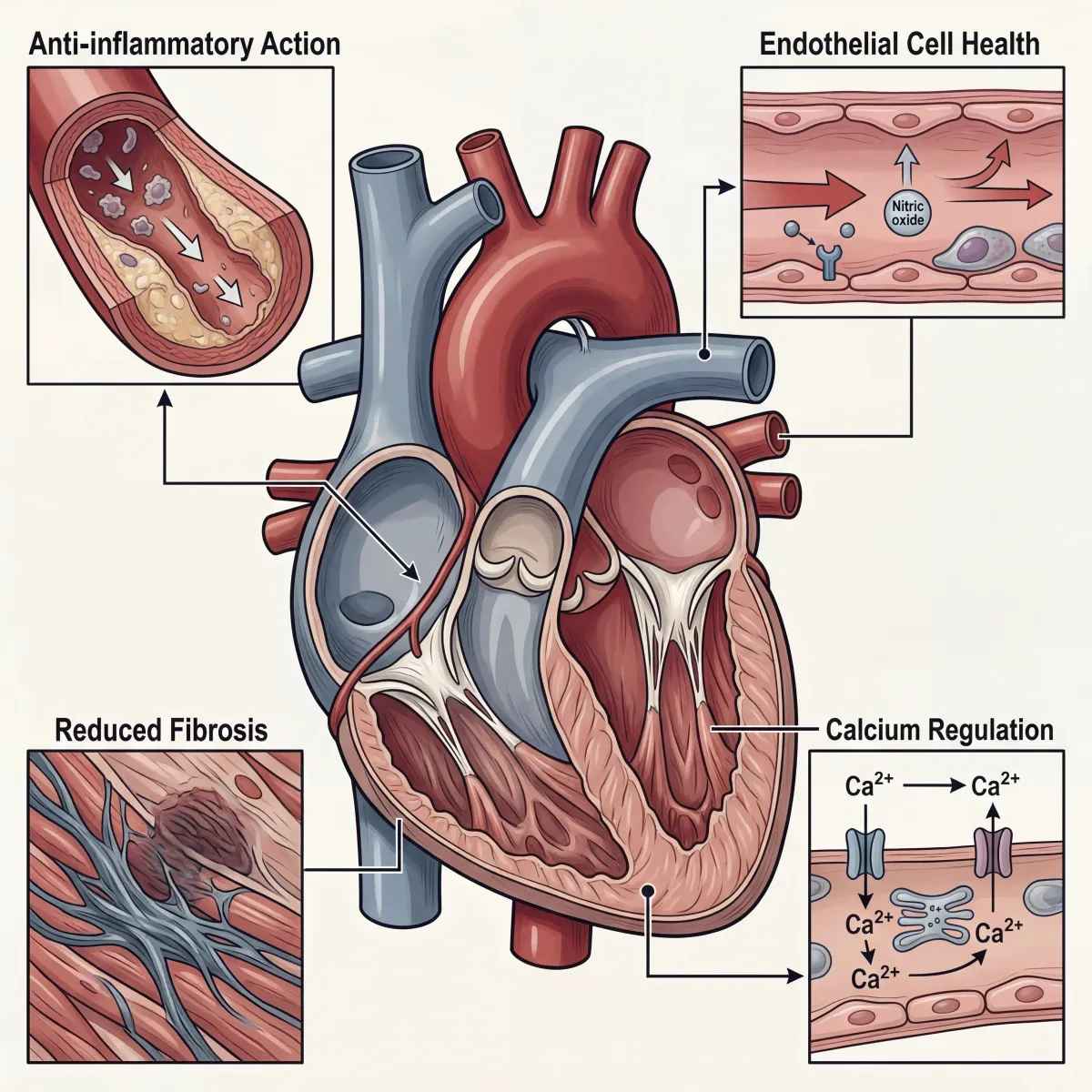
Several overlapping biological mechanisms help explain why maintaining adequate vitamin D levels might protect against a second heart attack:
- Anti-inflammatory action: Vitamin D suppresses inflammatory cytokines that drive atherosclerotic plaque instability — the process that typically triggers heart attacks. After a first event, inflammation levels remain elevated, making this especially relevant for survivors.
- Endothelial function: The endothelium (inner lining of blood vessels) depends on adequate vitamin D signaling to maintain proper function. Endothelial dysfunction accelerates plaque formation and reduces nitric oxide availability.
- Anti-fibrotic effects: After a heart attack, scar tissue (fibrosis) replaces damaged muscle. Excessive fibrosis can create the electrical and structural instability that leads to subsequent events. Vitamin D appears to modulate this process through TGF-beta pathway regulation.
- Renin-angiotensin system regulation: Vitamin D helps regulate the hormonal system that controls blood pressure and fluid balance. Dysregulation of this system is a major driver of post-MI complications.
There is also a compelling seasonal pattern that supports this biology. Cardiovascular events spike during late winter months, when vitamin D levels reach their nadir, and decline during summer when levels peak. This temporal correlation, documented across multiple countries and climate zones, adds another layer of evidence that vitamin D status and cardiac outcomes are mechanistically linked rather than merely coincidental.
What "Target-to-Treat" Actually Looks Like in Practice
The TARGET-D protocol was not simply "take more vitamin D." It was a structured clinical management strategy with regular monitoring and dose adjustments. Understanding the specific protocol matters, because it highlights why this approach worked when blanket supplementation did not.
Here is how the treatment arm operated:
| Step | Action | Details |
|---|---|---|
| 1. Baseline testing | Measure 25(OH)D blood level | Within one month of heart attack |
| 2. Initial dosing | Prescribe vitamin D3 based on level | 58.8% started at 5,000 IU/day |
| 3. Follow-up testing | Recheck blood levels | Every 3 months if below 40 ng/mL |
| 4. Dose adjustment | Increase or decrease dose | Until >40 ng/mL achieved |
| 5. Maintenance monitoring | Annual blood level check | Once target level is stable |
The fact that more than half of participants required 5,000 IU daily — roughly six to eight times the standard recommended intake of 600-800 IU — speaks to how inadequate typical supplementation guidelines may be for people recovering from heart attacks. The standard recommendations were designed primarily for bone health in the general population, not for cardiovascular protection in high-risk patients.
The monitoring component is equally important. A person taking 2,000 IU daily might achieve a blood level of 35 ng/mL or 55 ng/mL depending on their body weight, skin pigmentation, stress and cortisol levels, sun exposure, and genetic factors affecting vitamin D metabolism. Without testing, there is no way to know whether supplementation is actually correcting the deficiency.
85% of Heart Attack Patients Had Insufficient Vitamin D — Are You Among Them?
One of TARGET-D's most striking findings was just how common vitamin D insufficiency was among heart attack survivors: 85% entered the trial with blood levels below 40 ng/mL. This is consistent with global estimates that between half and two-thirds of the worldwide population has suboptimal vitamin D levels.
Several populations carry elevated risk for both vitamin D deficiency and heart disease simultaneously:
- Adults over 65: Aging skin produces less vitamin D from sunlight, and older adults tend to spend more time indoors. This age group also faces the highest heart attack risk.
- People with darker skin: Higher melanin levels reduce cutaneous vitamin D synthesis. The D-Health trial, a randomized controlled trial of 21,315 Australian adults, found that vitamin D supplementation reduced myocardial infarction risk by 19% (HR 0.81, 95% CI 0.67-0.98) — and the benefit was stronger in those already taking cardiovascular medications.
- People with obesity: Vitamin D is fat-soluble and gets sequestered in adipose tissue, reducing its bioavailability. This means heavier individuals need substantially higher doses to achieve the same blood levels.
- Those living at northern latitudes: Above approximately 37 degrees north latitude (roughly the line from San Francisco to Richmond, Virginia), sunlight during winter months is too weak to trigger adequate vitamin D production in the skin.
- Heart attack survivors already on cardiovascular medications: The D-Health trial found particularly strong benefits in this subgroup (HR 0.84, 95% CI 0.74-0.97), suggesting that vitamin D supplementation may complement standard cardiac medications rather than competing with them.

Worth noting: Having your vitamin D levels tested is a simple blood draw. The 25-hydroxyvitamin D test (also called 25(OH)D) is the standard measurement. If you have survived a heart attack, this test is inexpensive, low-risk, and — based on the TARGET-D findings — potentially high-value information.
What You Need to Know Before Taking Higher Doses
The TARGET-D trial reported no adverse outcomes from higher-dose vitamin D3 supplementation, which is consistent with the safety profile observed across every major vitamin D trial to date. The VITAL trial, D-Health trial, and Finnish Vitamin D Trial all found no excess adverse events compared to placebo.
That said, vitamin D supplementation above standard doses requires medical supervision, particularly for heart attack survivors who are typically taking multiple medications. According to Mayo Clinic, taking more than 4,000 IU daily without medical oversight can lead to hypercalcemia (excess calcium in the blood), which can cause heart rhythm disturbances — the opposite of what you want when recovering from a cardiac event.
Key drug interactions relevant to cardiac patients include:
- Digoxin: High-dose vitamin D can raise calcium levels, increasing the risk of dangerous heart rhythms in patients taking this heart medication.
- Diltiazem and other calcium channel blockers: Elevated calcium from excessive vitamin D can interfere with how these blood pressure medications work.
- Atorvastatin and other statins: Vitamin D may affect how the body processes certain cholesterol-lowering medications.
- Thiazide diuretics: These can reduce calcium excretion, and combined with high-dose vitamin D, may increase hypercalcemia risk.
The critical takeaway from TARGET-D is not "take 5,000 IU of vitamin D on your own." It is that a physician-monitored protocol with regular blood testing and dose adjustments produced meaningful cardiovascular protection in heart attack survivors. Self-dosing without monitoring defeats the entire purpose of the target-to-treat approach.
If you are interested in optimizing your heart health through evidence-based strategies, the first step is getting your levels tested and discussing the results with your cardiologist.
Frequently Asked Questions
Can vitamin D3 supplements prevent a first heart attack?
Based on current evidence, no. The VITAL trial (25,871 participants, 5.3 years) and multiple other large randomized controlled trials found no cardiovascular benefit from vitamin D supplementation in healthy people without prior heart disease. The TARGET-D trial's benefit was specific to people who had already experienced a heart attack and had documented vitamin D insufficiency. Primary prevention and secondary prevention appear to involve different biological dynamics.
How much vitamin D3 should heart attack survivors take?
There is no one-size-fits-all dose. In the TARGET-D trial, more than half of participants needed 5,000 IU daily to reach the target blood level of above 40 ng/mL, but individual needs varied widely based on body weight, baseline levels, and other factors. The essential element was not any specific dose but rather regular blood testing (25-hydroxyvitamin D) and dose adjustment to maintain adequate levels. This requires working with a physician.
What blood level of vitamin D should heart attack survivors aim for?
The TARGET-D trial targeted 25-hydroxyvitamin D levels above 40 ng/mL (100 nmol/L). This is higher than the 20 ng/mL (50 nmol/L) threshold that many laboratories use to define "sufficiency" for bone health. The standard sufficiency cutoff was never designed with cardiovascular protection in mind, and the TARGET-D findings suggest that 40 ng/mL may be a more appropriate therapeutic target for cardiac patients.
Is it safe to take 5,000 IU of vitamin D3 daily?
In the TARGET-D trial, no adverse effects were reported from higher-dose supplementation under medical supervision. However, the Mayo Clinic notes that sustained intake above 4,000 IU daily without monitoring can cause hypercalcemia. The safety of higher doses depends on regular blood testing and physician oversight — the same monitoring protocol that made the TARGET-D results possible.
Does this study mean my cardiologist should prescribe vitamin D?
The TARGET-D researchers themselves noted that larger confirmatory trials are needed before this becomes standard practice. However, getting your vitamin D levels tested after a heart attack is a reasonable conversation to have with your cardiologist, given the low risk and potential benefit of targeted supplementation. Many cardiology practices may start incorporating vitamin D testing into post-MI care as this evidence develops.
Related Articles
- Vitamin K2 and Arterial Calcification: Can This Overlooked Vitamin Protect Your Arteries? — How another fat-soluble vitamin plays a complementary role in cardiovascular protection.
- Sauna Bathing for Heart Health: What 20 Years of Finnish Research Actually Proves — Evidence-based strategies for reducing cardiovascular risk through regular heat exposure.
- Nitric Oxide Foods: The Complete Guide to Eating for Better Blood Flow and Lower Blood Pressure — Dietary approaches that support the same endothelial function vitamin D helps maintain.
- Strong Thighs Protect Your Heart: The Ultimate Guide to Leg Strength and Cardiovascular Health — The surprising connection between lower body strength and cardiac outcomes.
- Magnesium Types Explained (Glycinate, Citrate, Threonate) — Which to Take and When — Another essential mineral that works alongside vitamin D for heart and bone health.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.