What Happens When Bacteria Colonize the Wrong Part of Your Gut?
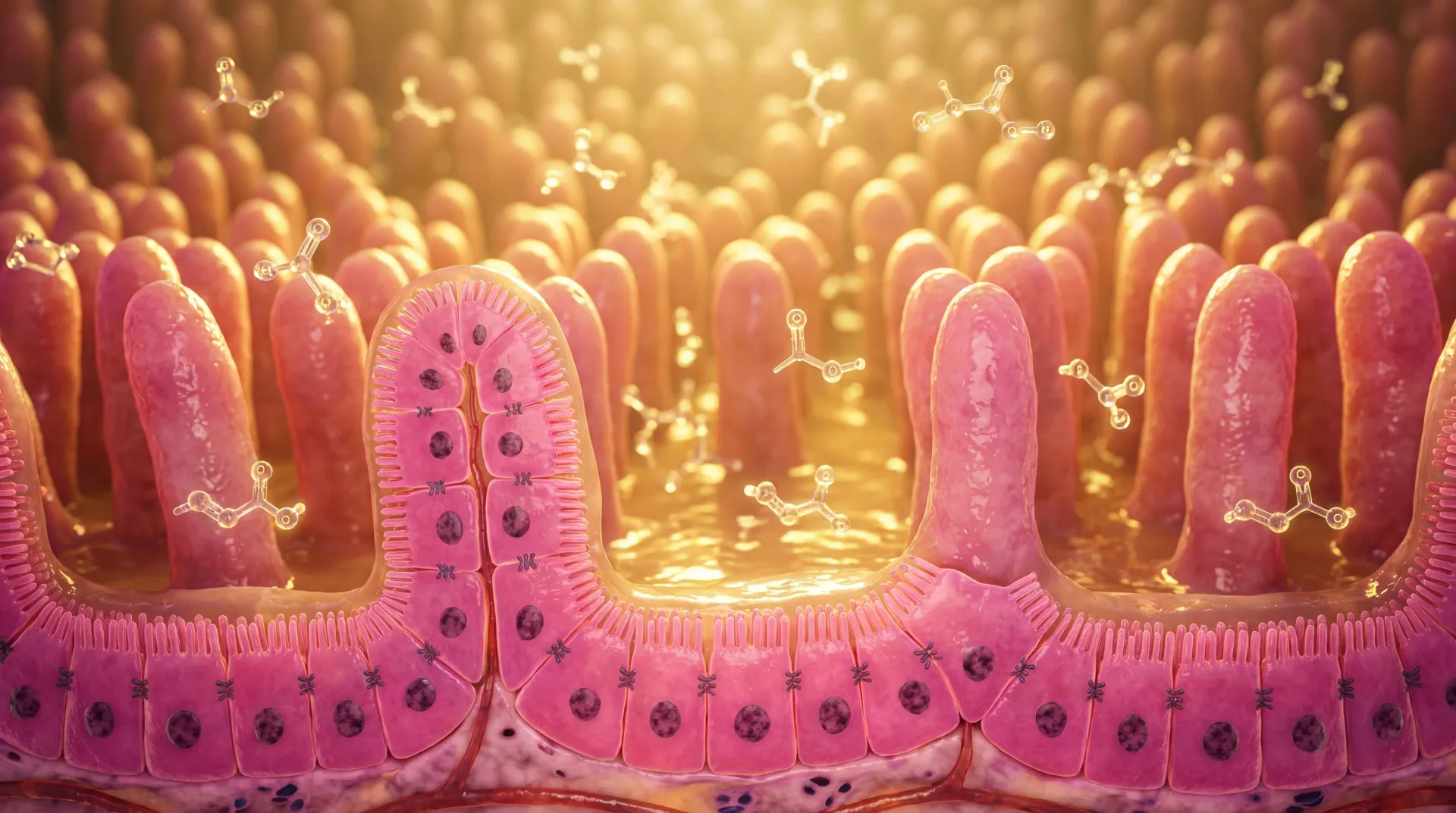
Your digestive tract is not a uniform environment. The stomach is intensely acidic, the large intestine teems with trillions of bacteria, and the small intestine — where most nutrient absorption occurs — normally houses fewer than 1,000 bacterial organisms per milliliter.
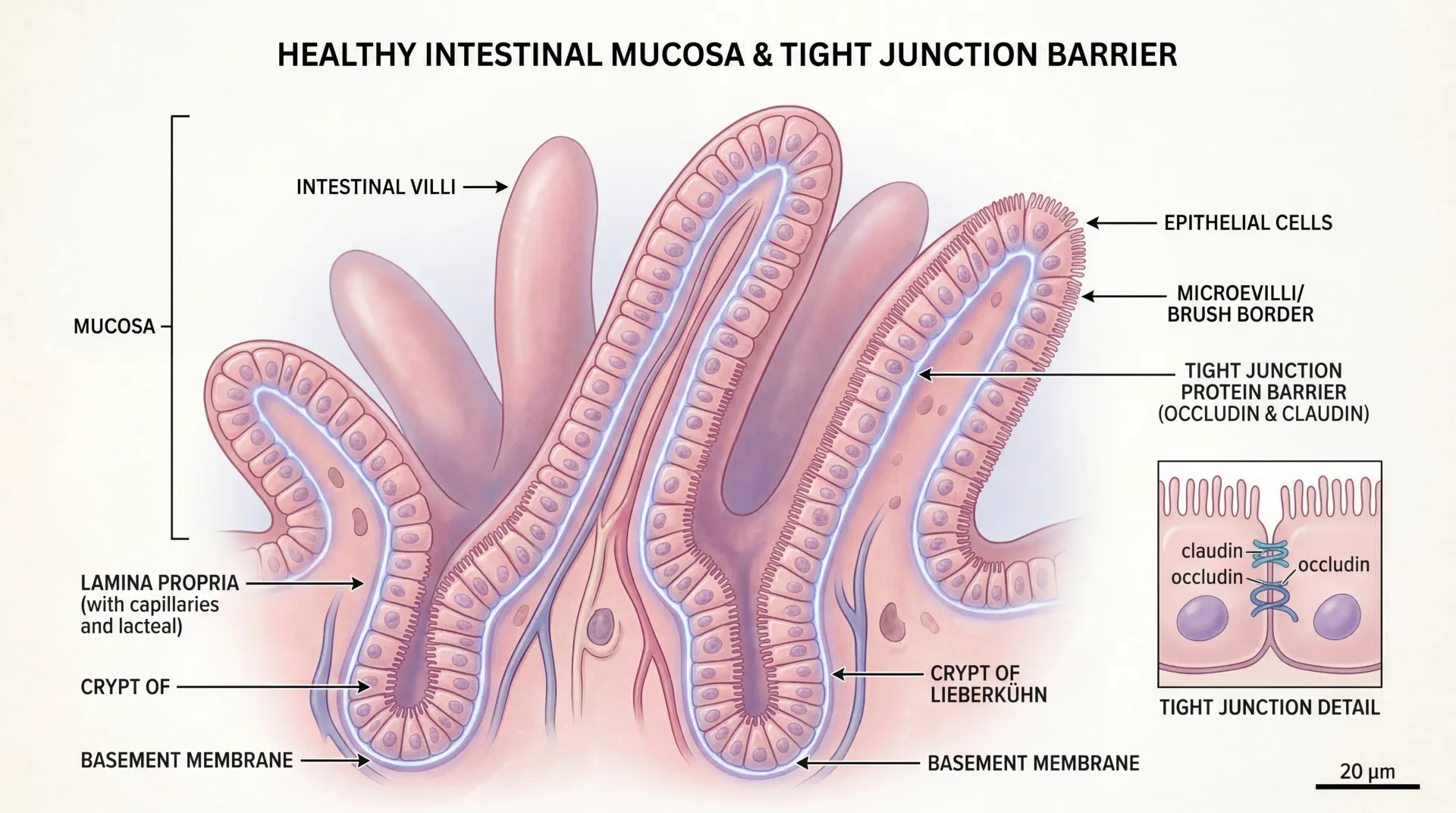
Small intestinal bacterial overgrowth, or SIBO, develops when colonic-type bacteria migrate into the small intestine and multiply beyond a threshold of approximately 10³ colony-forming units per milliliter. These bacteria ferment carbohydrates that should be absorbed, producing hydrogen, methane, and carbon dioxide gas. The gas causes bloating and distension, while the bacterial activity damages the intestinal lining and impairs nutrient absorption.
Prevalence estimates vary depending on the diagnostic method used and the population studied. General population estimates range from 2.5% to 22%, while elderly populations show rates between 14.5% and 15.6%. Even up to 13% of apparently healthy individuals with no digestive complaints test positive for SIBO on breath testing, suggesting the condition may exist on a spectrum rather than as a binary diagnosis.
Key Point: SIBO is not about having the wrong bacteria — it is about having normal bacteria in the wrong location. The small intestine relies on low bacterial counts to absorb nutrients effectively, and when that environment is disrupted, a cascade of digestive and systemic problems can follow.
Why SIBO Develops: Root Causes and Risk Factors
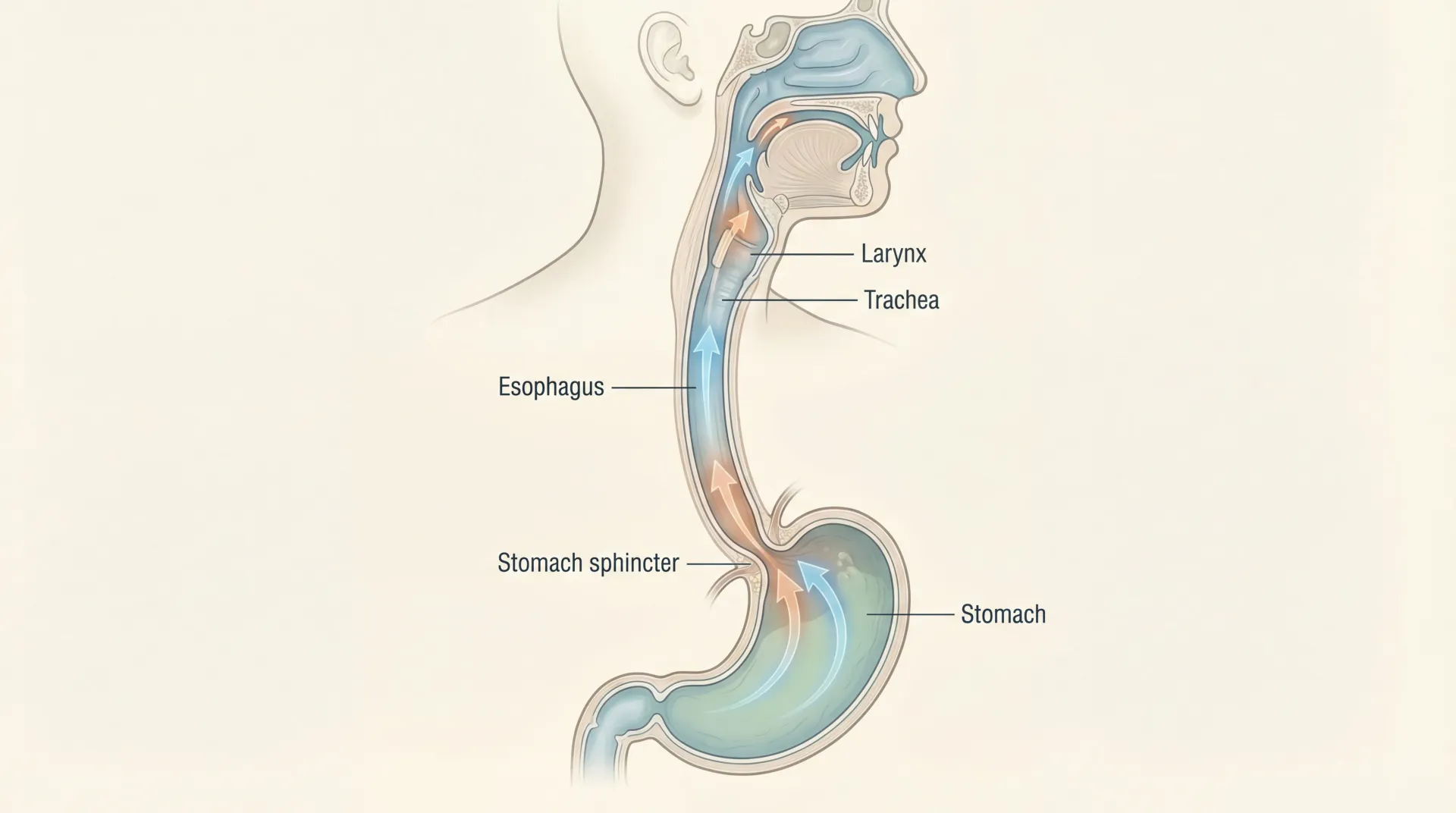
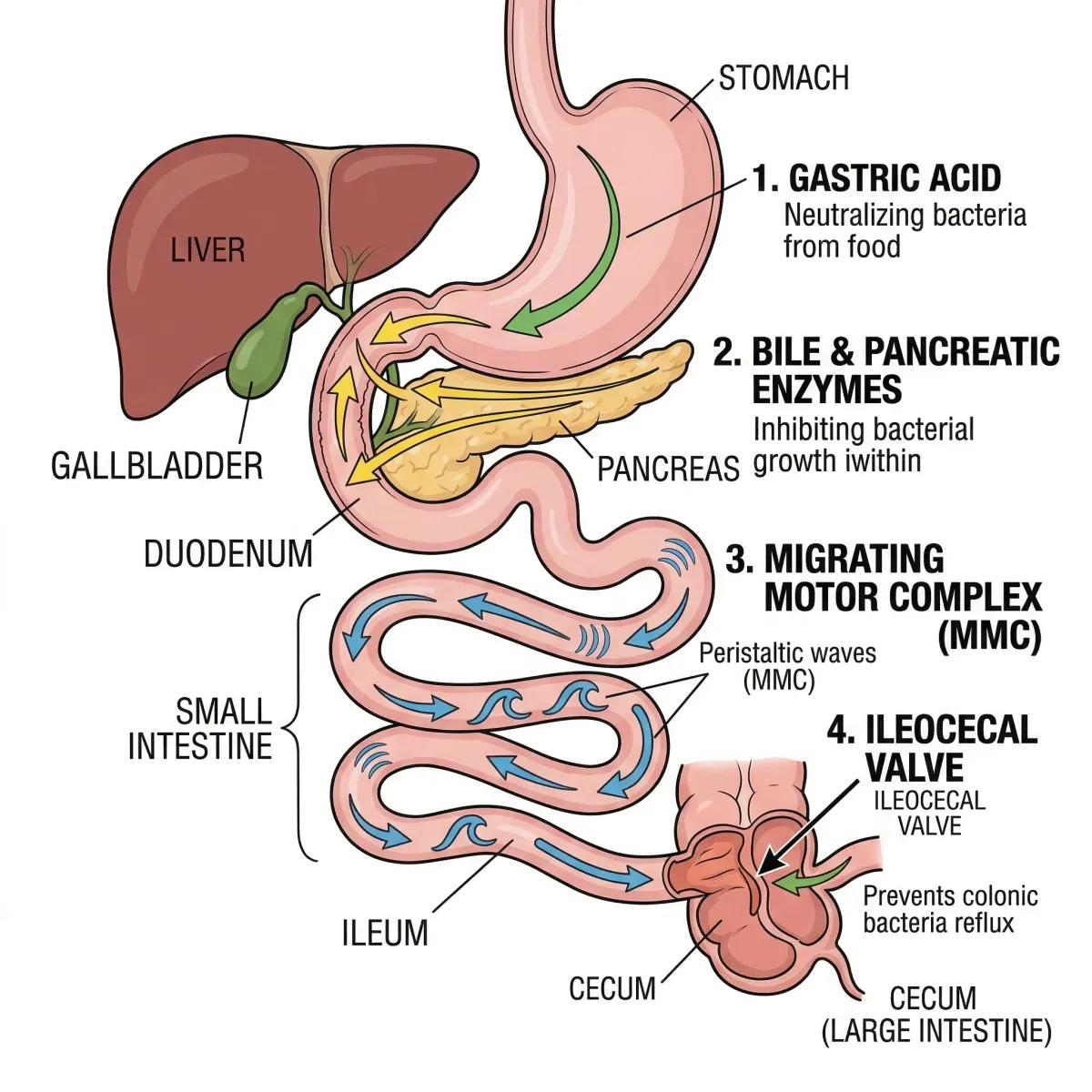
Your body maintains several layers of defense to keep bacterial populations in check within the small intestine. Gastric acid kills most ingested bacteria before they reach the small bowel. Bile and pancreatic enzymes provide additional antimicrobial effects. The migrating motor complex (MMC) — a cyclical pattern of intestinal contractions that occurs every 90 to 120 minutes during fasting — sweeps residual debris and bacteria downward toward the colon. The ileocecal valve acts as a physical barrier preventing backflow of colonic bacteria. When any of these mechanisms fail, SIBO can develop.
Motility disorders represent the single largest category of SIBO causes, with research showing that patients with small intestinal dysmotility face a 3.6-fold increased risk of developing the condition. Irritable bowel syndrome, diabetes-related neuropathy, scleroderma, and hypothyroidism all slow or disrupt the MMC, allowing bacteria to linger and proliferate. Together with chronic pancreatitis, motility disorders and IBS account for 80-90% of SIBO cases.
Medications play a significant and often underappreciated role. Proton pump inhibitors (PPIs) reduce gastric acid — the first line of defense against bacterial overgrowth. A meta-analysis of 19 studies found that PPI use increases SIBO risk by 70% (odds ratio 1.7). One study comparing acid-suppressing medications found that 53% of patients taking omeprazole developed bacterial overgrowth, compared with 17% taking the weaker acid suppressor cimetidine. Opioid medications and certain antibiotics can also impair motility and shift microbial balance in ways that favor overgrowth.
| Risk Factor | SIBO Prevalence or Risk | Mechanism |
|---|---|---|
| IBS | 10-84% (varies by study) | Dysmotility, altered MMC |
| Diabetes (with chronic diarrhea) | 43% | Autonomic neuropathy slows motility |
| Celiac disease | ~50-66% | Mucosal damage, altered motility |
| Hypothyroidism | >50% | Reduced gut motility |
| Liver cirrhosis | 31-68% | Portal hypertension, altered motility |
| PPI use | OR 1.7 (70% increased risk) | Reduced gastric acid barrier |
| Prior abdominal surgery | 62% (post-colectomy) | Structural changes, blind loops |
| IBD (Crohn's/UC) | 31% (5.25x controls) | Inflammation, strictures, surgery |
Structural abnormalities — surgical blind loops, small bowel diverticula, strictures, and adhesions — create pockets where bacteria accumulate undisturbed. A 2024 meta-analysis confirmed IBD patients carry a 5.25-fold higher SIBO risk, with Crohn's (32.2%) affected more than ulcerative colitis (27.8%).
Recognizing SIBO: Symptoms That Extend Beyond Bloating
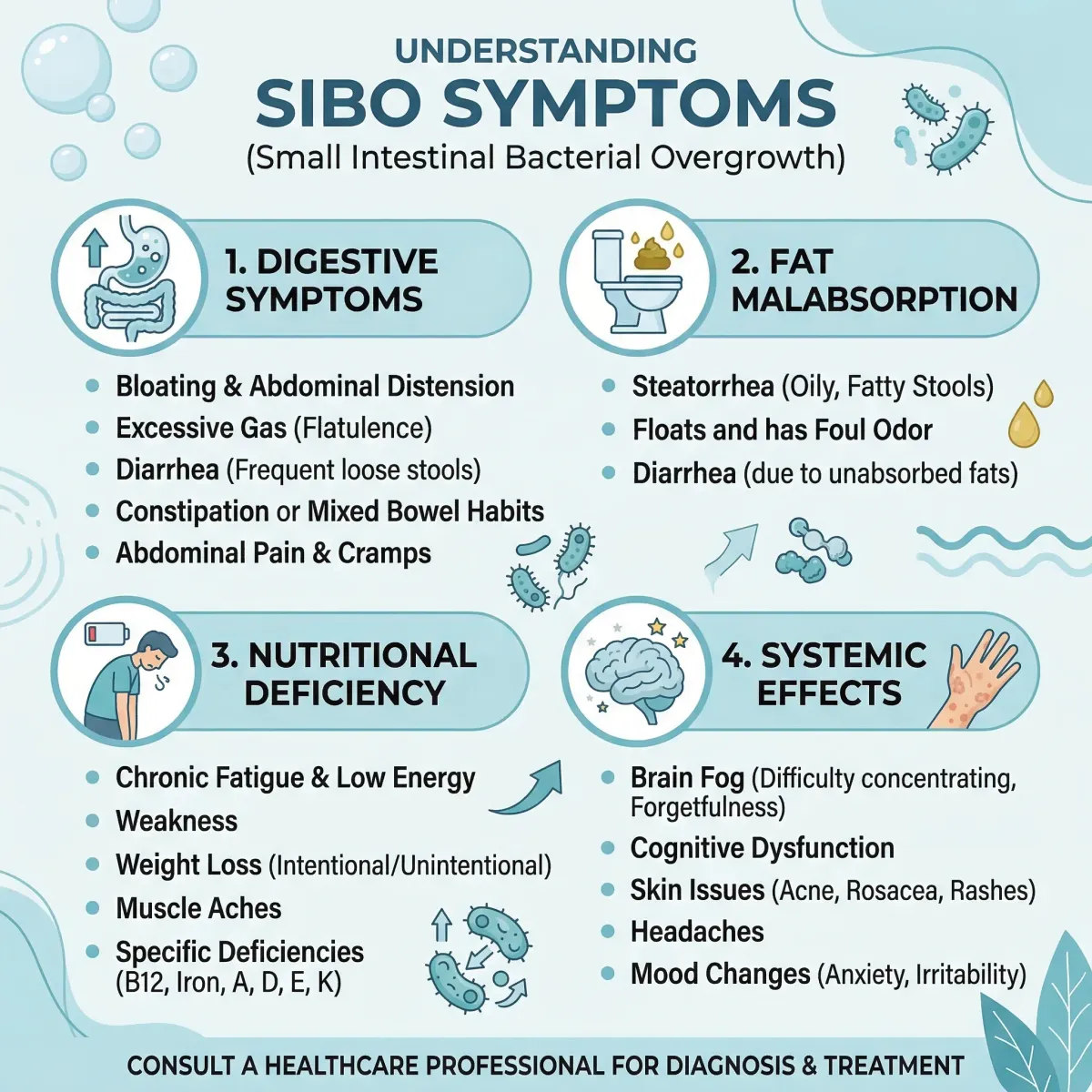
SIBO produces symptoms that overlap heavily with IBS, food intolerances, and other functional digestive disorders, making it one of the more frustrating conditions to pin down based on symptoms alone. The core complaints — abdominal bloating, gas, distension, and altered bowel habits — appear in more than two-thirds of SIBO patients, but these same symptoms describe dozens of other conditions.
The timing is a clue. Bloating tends to worsen progressively throughout the day as bacteria ferment incoming carbohydrates, often reaching its worst point in the evening. Many patients report that specific carbohydrate-rich meals reliably trigger symptoms within 30 to 90 minutes, which correlates with the transit time to the affected portion of the small bowel. Understanding how your microbiome influences gut-brain signaling helps explain why digestive distress from SIBO frequently co-occurs with mood and cognitive symptoms.
| Symptom Category | Specific Symptoms | Underlying Mechanism |
|---|---|---|
| Digestive | Bloating, gas, abdominal pain, diarrhea, constipation, nausea, belching | Bacterial fermentation of carbohydrates producing gas |
| Fat malabsorption | Oily/floating stools (steatorrhea), weight loss | Bacteria deconjugate bile salts, impairing fat digestion |
| Nutritional deficiency | Fatigue, weakness, numbness/tingling, muscle cramps | Impaired absorption of B12, iron, fat-soluble vitamins (A, D, E, K) |
| Neurological (rare) | Confusion, slurred speech, ataxia | D-lactic acidosis from bacterial metabolism |
Nutritional deficiencies develop because overgrown bacteria consume nutrients before you can absorb them. Vitamin B12 is particularly vulnerable — bacteria competitively uptake cobalamin, causing weakness, sensory ataxia, and paresthesia. Fat-soluble vitamins (A, D, E, K) become depleted when bacteria deconjugate bile salts needed for fat absorption. Iron and calcium deficiencies also develop in prolonged cases.
SIBO's reach extends beyond the gut. A 2024 review in Biomedicines documented elevated SIBO prevalence across seemingly unrelated conditions: 46% in acne rosacea patients, 48% in Alzheimer's disease, and 46% in Parkinson's disease. Whether SIBO contributes to these conditions or results from them remains unclear, but it suggests the intestinal bacterial environment has wider systemic effects than previously recognized. If you are managing conditions linked to chronic inflammation, understanding leaky gut syndrome and intestinal permeability provides important context for how bacterial overgrowth creates cascading problems.
How SIBO Is Diagnosed: Breath Tests and Their Limitations
SIBO diagnosis is imperfect. There is no validated gold standard diagnostic test. The condition has been recognized for decades, yet clinicians still work with imperfect tools that produce both false positives and false negatives at concerning rates.
The two main diagnostic approaches are small bowel aspirate culture and carbohydrate breath testing. Culture — where fluid is collected from the small intestine during endoscopy and tested for bacterial concentration — is the more direct method. A threshold of ≥10³ colony-forming units per milliliter is considered diagnostic. The problem is practical: the procedure is invasive, expensive, and agrees with breath testing only 65.5% of the time, suggesting one or both methods regularly miss the diagnosis or overcall it.
Breath testing is what most patients actually receive. You drink a measured dose of glucose or lactulose after an overnight fast, then breathe into collection tubes at intervals. If bacteria in the small intestine ferment the substrate before it reaches the colon, they produce hydrogen and methane that diffuse into your bloodstream and exit through your breath. Since carbohydrate fermentation by gut bacteria is the only source of hydrogen in the human body, elevated breath hydrogen reliably indicates bacterial activity — the question is where.

| Breath Test Type | Substrate | Positive Criteria | Sensitivity | Specificity |
|---|---|---|---|---|
| Glucose hydrogen | 75g glucose | Hydrogen ≥20 ppm above baseline within 90 min | 44% | 80-86% |
| Lactulose hydrogen | 10g lactulose | Hydrogen ≥20 ppm above baseline within 90 min | 31% | 80-86% |
| Methane | Either substrate | Methane ≥10 ppm at any point | Variable | Variable |
The 2017 North American consensus standardized criteria: hydrogen rise ≥20 ppm above baseline within 90 minutes, or methane ≥10 ppm. Glucose tests are more specific but only detect proximal overgrowth, since glucose gets absorbed before reaching the distal small bowel. Lactulose catches distal overgrowth but produces more false positives from rapid colonic transit.
Preparation is specific. Current guidelines recommend a 4-week washout from antibiotics and probiotics, 1 week off PPIs, 48 hours without motility drugs, and a 12-hour fast. Another complication: approximately 10-15% of people lack hydrogen-producing bacteria, which can produce false negatives regardless of preparation.
Note: A single negative breath test does not rule out SIBO. Given the low sensitivity of both glucose (44%) and lactulose (31%) breath tests, some gastroenterologists recommend testing with both substrates or combining breath testing with clinical assessment and a trial of treatment.
Treatment Approaches: Antibiotics, Herbal Options, and Emerging Therapies
Treating SIBO follows a three-part logic: reduce the bacterial overgrowth, repair nutritional deficiencies caused by malabsorption, and address the underlying condition that allowed overgrowth to develop. Most treatment discussions focus heavily on the first part — bacterial reduction — but lasting improvement requires attention to all three.
Rifaximin (brand name Xifaxan) is the most studied antibiotic for SIBO. A systematic review across 15 studies found it eradicated SIBO in 70.8% of patients, with adverse events in only 4.6% of cases. Rifaximin works primarily in the gut and is minimally absorbed into the bloodstream, which reduces systemic side effects. Standard dosing is 550 mg three times daily for 14 days.
A meta-analysis found a relative risk of improvement of 2.46 compared with placebo (49.5% vs 13.7% response), with a number needed to treat of 2.8. For methane-predominant SIBO (which tends to cause constipation rather than diarrhea), combining neomycin with rifaximin outperforms rifaximin alone.
The herbal alternative has gained traction after a Johns Hopkins study compared herbal antimicrobials to rifaximin. Herbal therapy achieved a 46% negative breath test rate versus 34% for rifaximin (P=.24, not significant), with fewer adverse events (2.7% versus 9%). The protocols used oregano oil, berberine, thyme oil, and wormwood. Among rifaximin non-responders, herbal rescue therapy achieved 57.1% response — comparable to triple antibiotic rescue at 60%.
| Treatment | Eradication/Response Rate | Duration | Adverse Events |
|---|---|---|---|
| Rifaximin | 60-71% eradication | 14 days typical | 4.6% |
| Herbal antimicrobials | 46% negative breath test | 4 weeks | 2.7% |
| Systemic antibiotics (various) | 51.1% breath normalization | 7-14 days | Variable, higher than rifaximin |
| Elemental diet | 85% symptomatic response | 2-3 weeks | 12% intolerance |
Berberine is under more rigorous investigation. The BRIEF-SIBO trial at Peking University is comparing berberine to rifaximin head-to-head (400 mg twice daily, two weeks). Early data suggests berberine may enhance beneficial gut bacteria like Bacteroides and Bifidobacterium — microbiome-supportive effects that antibiotics lack.
Nutritional repletion should not be an afterthought. B12 supplementation is frequently necessary, along with iron, calcium, magnesium, and fat-soluble vitamins (especially D and K) depending on malabsorption severity.
The SIBO-Diet Connection: Low-FODMAP and Elemental Protocols
Dietary modification plays a supporting role in SIBO management. It can reduce symptoms and limit bacterial fuel, but it is not a standalone treatment. The bacteria need to be reduced first, usually with antibiotics or herbal antimicrobials, and diet helps manage symptoms during and after that process.
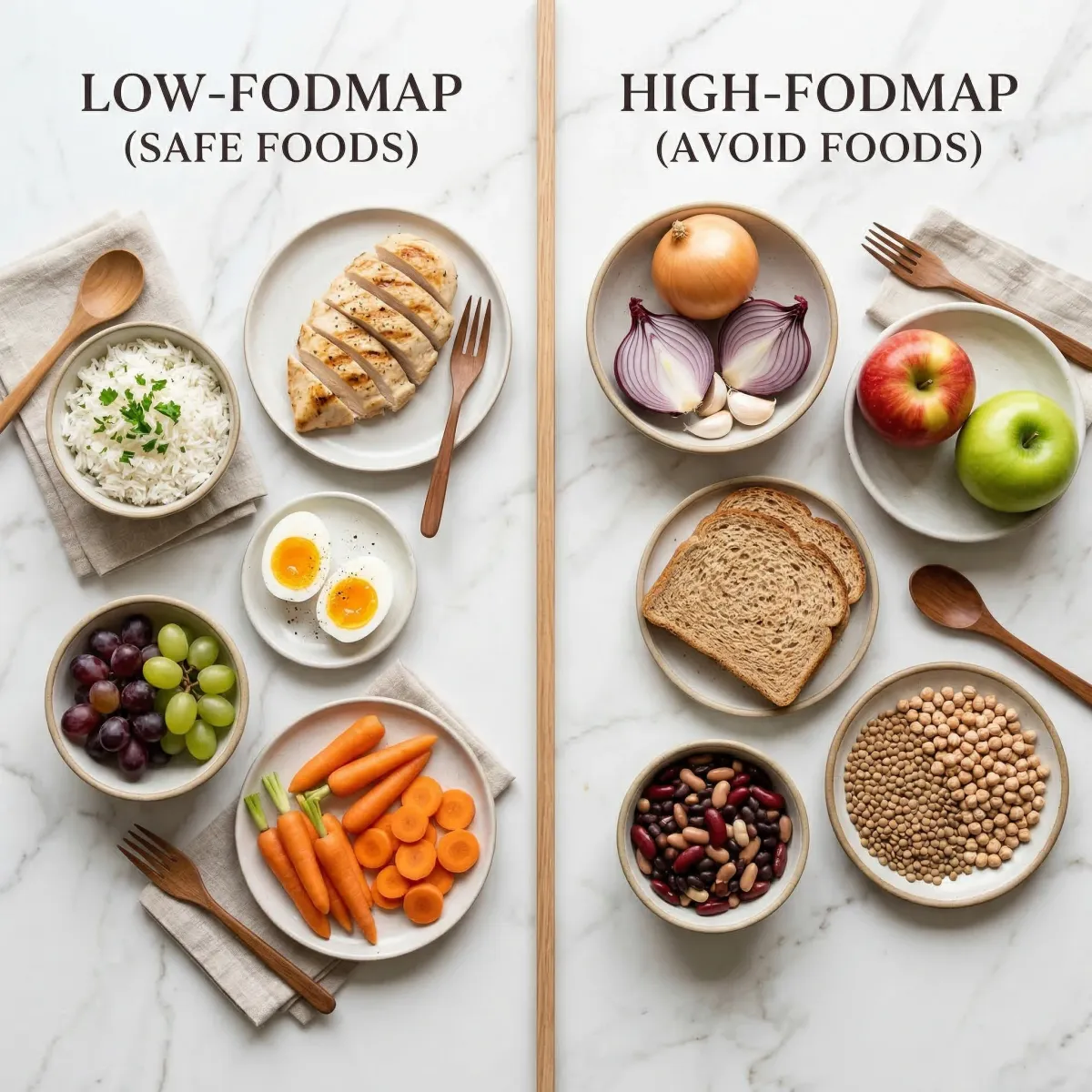
The low-FODMAP approach is the most widely recommended dietary strategy. FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are short-chain carbohydrates that bacteria ferment readily. Reducing FODMAP intake during the treatment phase — typically a 3 to 4 week elimination period — limits the fuel available to overgrown bacteria and can meaningfully reduce gas, bloating, and abdominal pain. If you are dealing with IBS alongside SIBO, the practical low-FODMAP guide for IBS covers the elimination and reintroduction process in detail.
| Category | Low-FODMAP (generally safe) | High-FODMAP (limit during treatment) |
|---|---|---|
| Fruits | Grapes, oranges, strawberries, blueberries | Apples, pears, cherries, watermelon |
| Vegetables | Carrots, cucumbers, tomatoes, zucchini | Onions, garlic, cauliflower, mushrooms |
| Proteins | Eggs, plain meats, poultry, seafood | Marinated/processed meats with additives |
| Grains | Quinoa, rice, oats (gluten-free) | Wheat, rye, barley |
| Dairy | Lactose-free options, hard cheeses | Milk, ice cream, soft cheeses |
| Sweeteners | Maple syrup (small amounts), sugar | Honey, sorbitol, xylitol, HFCS |
An important caution: strict FODMAP elimination should not extend beyond six weeks. Prolonged restriction can reduce microbial diversity in the colon and lead to nutritional gaps. After the elimination phase, foods are reintroduced one group at a time to identify personal triggers while restoring dietary variety.
The elemental diet is more aggressive: predigested liquid nutrition (amino acids, simple sugars, fats) for two to three weeks. Nutrients are absorbed before bacteria can ferment them, starving the overgrown population. A retrospective review of 124 patients achieved an 85% symptomatic response rate, though 12% could not tolerate the taste and monotony. This is typically reserved for patients who fail other treatments. For gut repair during reintroduction, bone broth's healing properties can complement the process.
Preventing Relapse: Why SIBO Keeps Coming Back
Recurrence is SIBO's biggest clinical problem. Approximately 45% of patients experience recurrent SIBO following antibiotic completion. Tracked over time, recurrence rates climb steadily — 12.6% at three months, 27.5% at six months, and 43.7% at nine months. One study found that average symptom improvement lasted only 22 days after a standard antibiotic course, and among rifaximin responders specifically, 84.4% experienced recurrence within 18 weeks.
The explanation is straightforward: antimicrobials reduce bacterial numbers but do not fix why bacteria accumulated. If the MMC remains sluggish, a PPI stays in the medication regimen, or a structural abnormality shelters bacteria, overgrowth returns once treatment stops.
Preventing relapse therefore means identifying and managing the root cause:
- Optimize motility: If the MMC is impaired, prokinetic agents (such as low-dose erythromycin or prucalopride) may help maintain the sweeping function that clears bacteria. Address underlying conditions affecting motility — thyroid function, blood sugar control in diabetes, and careful medication review.
- Review medications: Evaluate whether PPIs are truly necessary. Consider stepping down to H2 blockers where appropriate. Reduce or eliminate opioids when possible. Each of these medication classes independently increases SIBO risk.
- Meal spacing: The MMC only activates during fasting periods. Frequent snacking or grazing keeps it suppressed. Allowing 4 to 5 hours between meals gives the MMC time to complete its cleaning cycles.
- Address structural issues: Surgical correction of blind loops, stricture dilation, or adhesiolysis may be appropriate for patients with recurrent SIBO driven by anatomic abnormalities.
For patients who experience more than four episodes per year, prophylactic antibiotic cycling — 5 to 10 days every two weeks or monthly — may be considered, rotating antibiotic classes to mitigate resistance. The gut-heart axis research underscores why preserving microbial diversity matters even while treating SIBO.
Frequently Asked Questions
Can SIBO go away on its own without treatment?
Rarely. Because SIBO develops due to an underlying impairment — reduced motility, low stomach acid, structural abnormalities — the overgrowth tends to persist without intervention. Mild cases triggered by temporary factors (like a short antibiotic course) may resolve once the trigger is removed, but established SIBO typically requires antimicrobial treatment plus management of the root cause.
How long does it take to feel better after starting SIBO treatment?
Most patients notice symptom improvement within the first week of treatment. Full courses run 14 days for rifaximin or 4 weeks for herbal protocols. Nutritional deficiencies take longer to correct — often several months. Complete recovery of digestive function can take 3 to 6 months after successful eradication.
Is SIBO the same as IBS?
No, though they overlap significantly. IBS is a functional diagnosis based on symptom patterns, while SIBO is a measurable condition involving excess bacteria in the small intestine. Studies estimate that anywhere from 10% to 84% of IBS patients may have SIBO, depending on the diagnostic criteria used. When IBS patients with confirmed SIBO receive targeted antibiotic treatment, they respond at significantly higher rates (51.2%) than IBS patients without SIBO (23.4%), suggesting that SIBO may be driving symptoms in a substantial subset of IBS cases.
Are probiotics helpful or harmful for SIBO?
The evidence is mixed. Some meta-analyses found certain strains reduced hydrogen production, but other research suggests probiotics can colonize the small intestine and worsen overgrowth. Current guidance recommends treating SIBO first and considering strain-specific probiotics afterward to support recolonization — generic supplements are not likely to help.
What is the difference between hydrogen-dominant and methane-dominant SIBO?
The type of gas produced by the overgrown bacteria determines the dominant symptom pattern. Hydrogen-dominant SIBO typically causes diarrhea, while methane-dominant SIBO (sometimes called intestinal methanogen overgrowth, or IMO) tends to cause constipation because methane slows intestinal transit. The distinction matters for treatment — hydrogen-dominant SIBO responds well to rifaximin alone, while methane-dominant SIBO generally requires a combination of rifaximin plus neomycin for effective eradication.
Related Articles
- Low-FODMAP Diet for IBS: A Practical Step-by-Step Guide — The elimination diet most commonly recommended alongside SIBO treatment, with detailed food lists and reintroduction protocols.
- Leaky Gut Syndrome: Symptoms, Causes, and Evidence-Based Healing — How intestinal permeability connects to bacterial overgrowth and systemic inflammation.
- Gut-Brain Axis: How Your Microbiome Affects Mood and Cognition — The bidirectional communication between gut bacteria and your brain that explains why SIBO affects more than digestion.
- Bone Broth Benefits for Gut Healing, Joints, and Skin — Nutritional support for intestinal repair during and after SIBO treatment.
- The Gut-Heart Axis: How Your Microbiome Controls Cardiovascular Risk — Why microbial balance matters beyond digestion, including SIBO's links to cardiovascular health.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.