
What GLP-1 Drugs Actually Do to Your Muscles
A 2024 poll found that roughly 12% of U.S. adults have used an incretin-based drug for weight loss, with about 6% actively on treatment. Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) work by mimicking gut hormones that signal fullness, slow gastric emptying, and dial down appetite at the neurological level. The weight loss they produce is real and substantial. But it comes with a catch that gets less attention than it deserves.
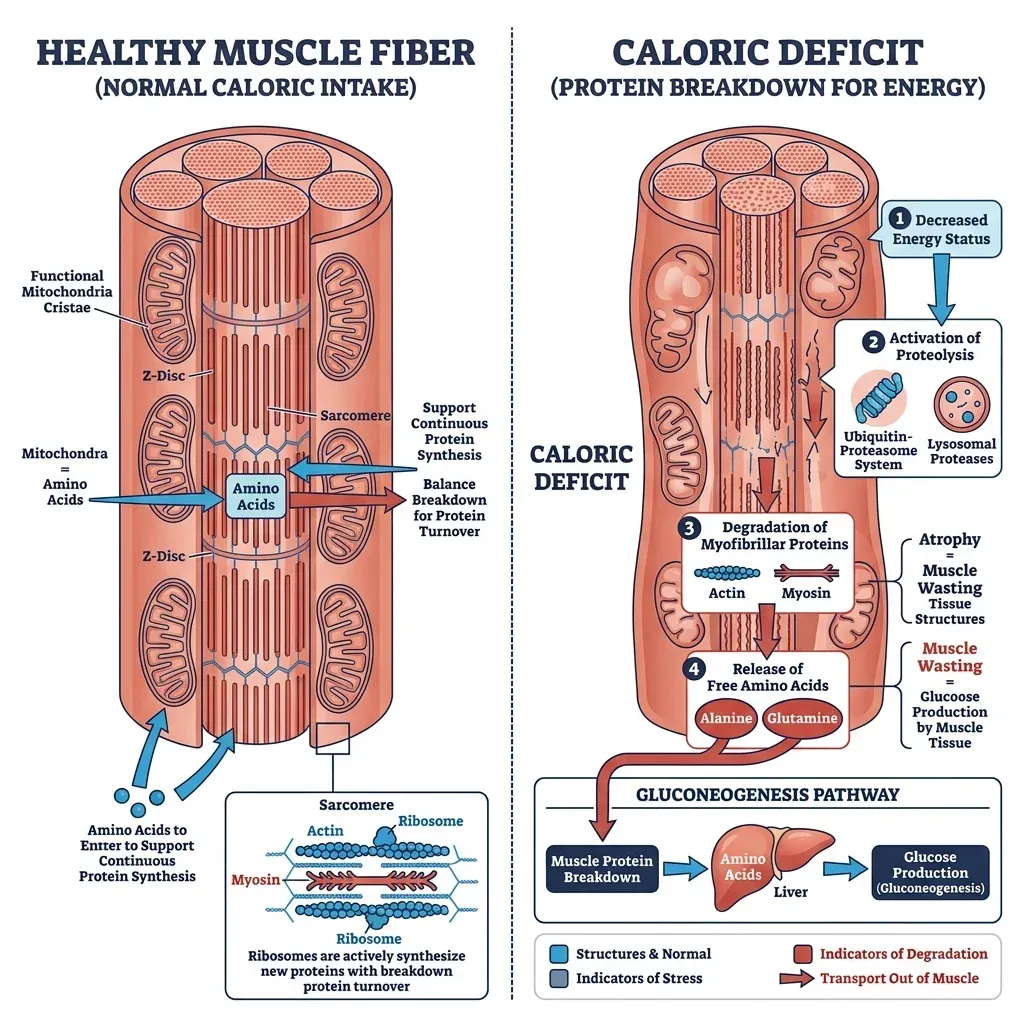
When your body runs a significant calorie deficit, it doesn't exclusively burn fat. Think of it like a company downsizing during a budget crunch. Fat is the obvious target, the bloated department everyone agrees can shrink. But the company also starts trimming support staff it actually needs. Your body does something similar: it breaks down muscle protein for glucose because the brain is a demanding organ that runs on glucose, and fat alone cannot be converted into glucose. That metabolic reality means some lean mass loss accompanies virtually every form of weight loss, from crash diets to bariatric surgery to GLP-1 medications.
Dr. W. Scott Butsch, an obesity medicine specialist at Cleveland Clinic, puts it plainly: "Muscle loss is related to the process of losing weight" — not some unique pharmacological effect of the drugs themselves. Mass General Brigham researchers echoed this at a recent Medical Grand Rounds: GLP-1 analogs don't show a uniquely high level of lean body mass loss compared to other weight loss approaches. We're just not accustomed to seeing weight loss this dramatic outside of surgical interventions.
A University of Utah study published in Cell Metabolism complicated the picture further. Katsu Funai's team gave semaglutide to mice and found that lean mass dropped about 10%, but most of the lost tissue came from organs like the liver — which shrank by nearly half — rather than skeletal muscle, which decreased only about 6%. But some muscles got weaker even when their size stayed roughly the same. Size and strength aren't the same thing, and current clinical trials don't routinely measure both. "We need these data in people," Funai said. Mouse physiology doesn't map directly onto humans, but the finding raises a question nobody has definitively answered yet.
The Numbers Behind GLP-1 Muscle Loss
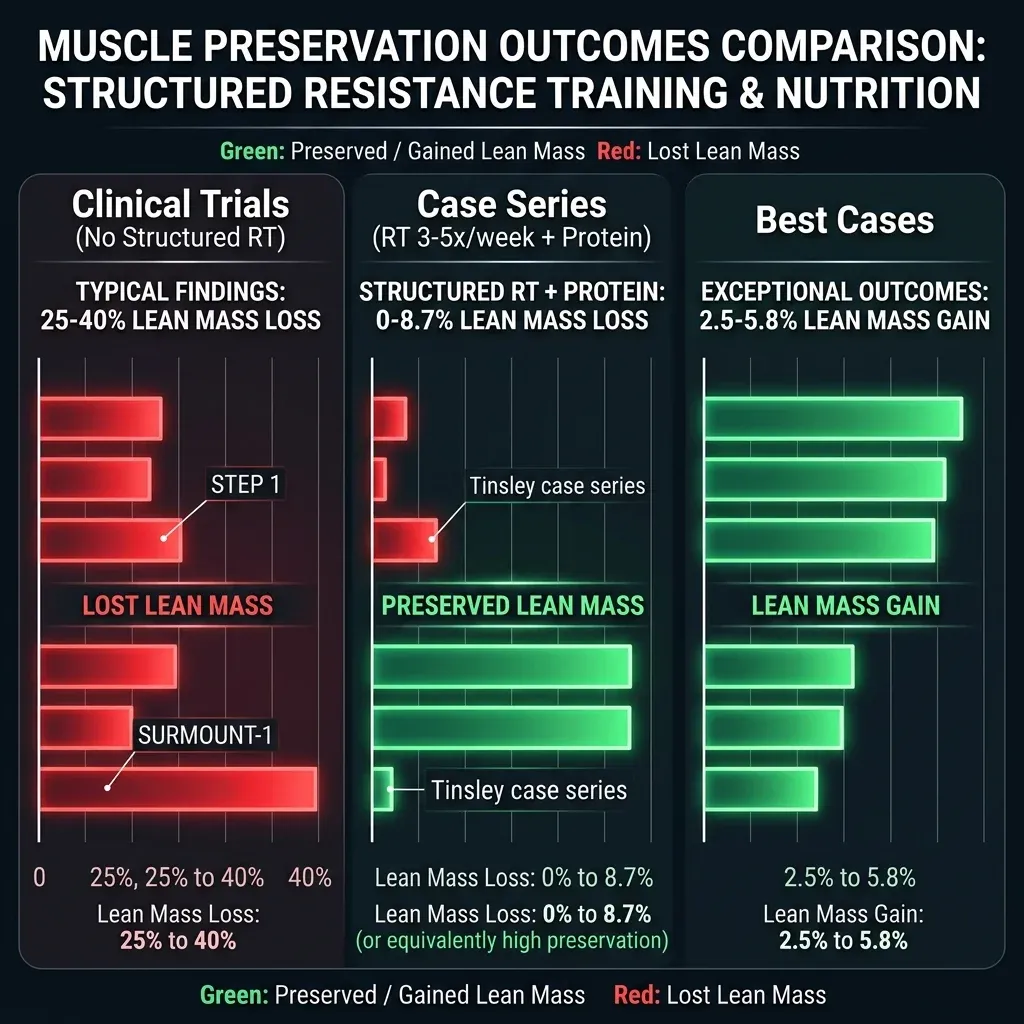
Two landmark trials set the baseline for what we know about body composition on these drugs. In the STEP 1 trial, 95 semaglutide-treated participants who underwent DXA body composition scans lost 6.9 kg of lean soft tissue alongside 10.4 kg of fat mass. That works out to roughly 40% of their total weight loss coming from lean tissue. In the SURMOUNT-1 trial testing tirzepatide, the ratio was better: 5.6 kg of lean loss versus 15.9 kg of fat loss, or about 26% lean.
A 2025 network meta-analysis pulling together data across multiple GLP-1RA and GLP-1/GIP receptor agonist drugs landed on a middle figure: approximately 25% of weight loss was lean mass. A separate systematic review put the range at 0% to 40% of total weight reduction, depending on the trial, the dose, and the patient population.
Key takeaway: On average, one quarter to one third of weight lost on GLP-1 drugs is lean tissue. That proportion is not fixed — it varies widely based on what else you're doing while on the medication.
The SEMALEAN study offered a more encouraging picture. This prospective study followed 106 patients on semaglutide 2.4 mg and found that lean mass declined about 3 kg at 7 months but then stabilized. Even more striking, handgrip strength — a functional measure that matters for daily life — actually improved by 4.5 kg at 12 months. The prevalence of sarcopenic obesity in the study group dropped from 49% at baseline to 33% at 12 months. This suggests the initial lean mass dip isn't necessarily a one-way trajectory.
One thing that gets lost in the muscle-loss panic: the proportion of your body that is lean mass can actually increase even as absolute lean mass drops. When someone goes from 56% body fat to 39% body fat, their remaining tissue is proportionally more muscular. The systematic review of semaglutide trials noted this explicitly — the proportion of lean mass relative to total body mass increased, "suggesting a positive overall outcome." The numbers need context to avoid unnecessary alarm.
Resistance Training: Your Most Powerful Countermeasure
Neither the STEP 1 nor SURMOUNT-1 trials included structured resistance training. Participants received lifestyle counseling with a goal of 150 minutes per week of physical activity, but as the research team behind a 2025 case series noted, SURMOUNT-1 explicitly stated that no specific strength training protocol was included. The lean mass numbers from those trials reflect outcomes without the single most effective tool for preserving muscle — and that gap changes everything.
Dr. Grant Tinsley at Texas Tech University and Dr. Spencer Nadolsky published a case series in 2025 documenting three patients who prioritized resistance training and protein intake during GLP-1 treatment. The results diverge sharply from trial averages.
| Patient | Drug | Weight Loss | Fat Mass Lost | Lean Tissue Change | RT Frequency |
|---|---|---|---|---|---|
| Case 1 (42F) | Tirzepatide | -33.0% | -53.4% | -6.9% (8.7% of loss) | 3x/week |
| Case 2 (42F) | Semaglutide | -26.8% | -61.6% | +2.5% (gained) | 5x/week |
| Case 3 (52M) | Semaglutide/Tirzepatide | -13.2% | -46.9% | +5.8% (gained) | 3x/week |
Compare that to the STEP 1 average where 40% of weight lost was lean tissue. Case 1, despite losing a third of her body weight on tirzepatide, lost only 8.7% as lean mass. Cases 2 and 3 actually built muscle while losing significant fat. Case 2 is particularly remarkable: she lost 26.8% of her body weight and gained lean tissue simultaneously.
All three patients trained consistently: resistance work 3-5 days per week targeting all major muscle groups (legs, hips, back, chest, shoulders, arms, abdomen), sessions lasting 30-45 minutes, at a reported intensity of 7-8 out of 10. They also mixed in cardio — walking, cycling, running — but the resistance component appears to be the differentiator. Earlier research by Villareal et al., published in the New England Journal of Medicine, found that exercise programs including resistance training were particularly effective at reducing thigh skeletal muscle loss during weight loss, compared to aerobic exercise alone.
A trial by Lundgren et al. demonstrated that adding an exercise program to liraglutide treatment preserved fat-free mass and potentiated fat loss, with a follow-up study showing that exercise participants maintained better weight and body composition a full year after stopping treatment. So the benefits compound over time.
If you take away one thing from this guide: start lifting. Resistance training is considered the most potent nonpharmacological stimulus for attenuating muscle loss and inducing skeletal muscle growth. Bodyweight exercises count. Resistance bands count. You don't need a gym membership to apply progressive resistance to your muscles.
Protein Requirements on GLP-1 Medications
GLP-1 drugs suppress appetite. That's the entire point. But the downstream consequence is that when you eat less overall, you tend to eat less protein too — and protein is the raw material your muscles need to rebuild after training. Dr. Kais Rona, a bariatric surgeon at MemorialCare, explained the mechanics: "Proteins are the building blocks of muscle tissue, and inadequate protein intake results in the breakdown of muscle."
The standard Recommended Dietary Allowance for protein is 0.8 g per kilogram of body weight per day. That number is a floor for preventing deficiency in sedentary, healthy adults. It was never designed for people losing significant weight while trying to preserve muscle. Multiple experts and guidelines converge on higher targets for GLP-1 users.
| Source | Recommended Protein Intake | Context |
|---|---|---|
| JAMA Internal Medicine MEAL Plan | 1.0-1.5 g/kg/day | Moderately active GLP-1 patients |
| Bariatric surgeon recommendation (Rona) | 1.2-1.5 g/kg/day | GLP-1 users generally |
| Case series patients (Tinsley) | 0.7-1.7 g/kg/day (body weight) or 1.6-2.3 g/kg/day (fat-free mass) | Patients who preserved/gained lean mass |
| Cleveland Clinic | 0.8-1.0 g/kg/day (minimum) | General starting point |
The JAMA guidance gets specific about timing and approach: begin each meal with 20-30 grams of protein from sources like fish, beans, chickpeas, or tofu. That protein-first strategy makes sense when your appetite is suppressed — you hit the nutrient your muscles need most before you fill up. If appetite is extremely low, protein shakes with at least 20g per serving can fill the gap.

One insight from the Tinsley case series deserves attention: expressing protein targets relative to body weight gets misleading as someone loses substantial weight. A person starting at 140 kg eating 1.0 g/kg/day gets 140g protein. At 95 kg, that same formula gives only 95g. The case series authors suggest that expressing protein intake relative to fat-free mass — around 1.6-2.3 g per kg of FFM — may be more appropriate in the context of obesity and substantial weight loss. That target stays more stable as fat drops away.
Research presented at ENDO 2025 by Dr. Melanie Haines from Massachusetts General Hospital found that among 40 semaglutide patients, those who lost the most muscle were older adults, women, and those who ate less protein. The protective effect of adequate protein intake showed up even in this small sample.
Supplements and Nutritional Strategies That Support Lean Mass
Beyond protein quantity, several supplemental strategies have emerging evidence behind them — though the research specifically in GLP-1 patients remains early-stage.
Creatine Monohydrate
Two of the three patients in the Tinsley case series supplemented with creatine monohydrate at 5 grams per day. Creatine is the most well-studied sports supplement in existence, with decades of evidence supporting its role in muscle strength and lean mass during resistance training. It works by replenishing phosphocreatine stores in muscle cells, giving you marginally more capacity for high-intensity effort.
No published RCT has tested creatine specifically alongside GLP-1 drugs in humans. But its mechanism doesn't depend on the weight-loss pathway — it supports the training stimulus that protects muscle. For someone doing resistance training on a GLP-1 medication, the rationale for 3-5g daily creatine monohydrate is strong based on general exercise science.
Ketone Esters
A team at the University of Alberta led by Jason Dyck found that pairing semaglutide with a drinkable ketone ester supplement protected both skeletal and cardiac muscle in obese mice while achieving the same fat loss. The mechanism centers on mitochondria: semaglutide appears to impair mitochondrial function in muscle, and ketones protect these energy factories from that impairment.
This aligns with what Mass General researchers described: ketosis blocks the glucose-alanine cycle, which means it blocks the extrusion of branched-chain amino acids from muscle. Ketones feed the brain directly, reducing the body's need to cannibalize muscle for glucose production.
Dyck's team has secured funding for human clinical trials, but those results are not yet available. Ketone ester supplements exist commercially, though they're expensive and not particularly palatable. This is promising science that's one step short of clinical recommendation.
The Basics That Matter
Christine Goukasian, a registered dietitian with UCLA Health's weight management program, emphasizes that patients on GLP-1 drugs need a well-balanced diet including lean protein, fruits, vegetables, and whole grains. Hydration is equally critical: the JAMA Internal Medicine guidelines recommend 2-3 liters of fluid daily, mainly water, with water-rich foods like cucumbers and watermelon filling gaps. Dehydration worsens muscle cramps and fatigue, compounding the challenge of maintaining a training routine.
Goukasian made a point worth repeating: "I hear patients say, 'It's great. I'm not eating because I'm not hungry.' That's wrong. We want you to still eat, because we want you to be nourished. We just want you eating the right things."
When Muscle Loss Becomes a Medical Concern
Losing a few kilograms of lean mass during 15-20% weight loss isn't inherently dangerous for most people. But context determines risk. A 35-year-old with plenty of muscle reserves faces a different situation than a 68-year-old who's already losing muscle from aging.
Fat-free mass loss on GLP-1 drugs can reach 15-40% of total weight lost. Meanwhile, normal age-related fat-free mass decline is only about 8% per decade. When GLP-1 medication accelerates that trajectory in someone who's already on the downslope, the gap between metabolically healthy and sarcopenic can close fast.
Dr. Katsu Funai at the University of Utah flagged this directly: "The loss of physical function is a strong predictor of not just quality of life but longevity", and adults over 60 carry higher baseline risk for both muscle loss and reduced mobility.
A 2025 review in Current Nutrition Reports identified several high-risk populations that warrant special attention: older adults, patients with chronic kidney disease, liver disease, and inflammatory bowel disease. These groups are already predisposed to sarcopenia, and the muscle-depleting effect of rapid weight loss stacks on top of their existing vulnerability.
Bone density adds another layer. A PMC review noted that a 10% reduction in body weight is associated with a 2.2% decrease in lumbar and total hip bone mineral density. For postmenopausal women or older men already at fracture risk, aggressive weight loss without bone-protective measures — calcium, vitamin D, weight-bearing exercise — creates compounding problems.
A University of Virginia research team published a paper in the Journal of Clinical Endocrinology & Metabolism finding that GLP-1 drugs significantly reduce body weight but with no clear evidence of improving cardiorespiratory fitness (VO2max). Their analysis of nearly 400,000 individuals found that cardiorespiratory fitness was far superior to overweight or obesity status for predicting mortality risk. Once fitness was factored in, body weight alone failed to predict death risk. That finding should give pause to anyone focused exclusively on the scale.
Zhenqi Liu, MD, at UVA School of Medicine, said what clinicians are thinking: "Some patients literally told me that they felt that they were losing muscle or muscle was slipping away from them while they were on these medications. This is a serious concern." The American Diabetes Association now recommends screening for malnutrition and low muscle mass risk before starting GLP-1 medications and promoting adequate protein and exercise throughout treatment.
Building Your GLP-1 Muscle Preservation Plan
Not all interventions carry equal weight. Mass General researchers reported that combining a high-protein diet and consistent exercise with GLP-1 treatment produced the greatest benefit in preserving bone and muscle mass, compared to diet alone or protein alone. Each element helps independently, but the combination is what shifts outcomes from "significant lean mass loss" to "minimal lean loss or even muscle gain."
The Three-Tier Protocol
Tier 1 — Resistance Training (non-negotiable)
- Minimum 2-3 sessions per week, 30 minutes each
- Target all major muscle groups: legs, hips, back, chest, shoulders, arms
- Progressive overload: bodyweight, bands, free weights, or machines
- Intensity: work hard enough that the last 2-3 reps of each set are genuinely difficult
- Start at medication initiation, not after muscle loss has already occurred
Tier 2 — Protein Optimization
- Target 1.0-1.5 g protein per kg body weight daily (most expert recommendations converge here)
- Begin each meal with 20-30g protein
- Use protein supplements if appetite makes whole-food intake difficult
- As you lose weight, recalculate targets — consider using fat-free mass as the reference
Tier 3 — Supportive Measures
- Creatine monohydrate: 3-5g daily
- Hydration: 2-3 liters per day minimum
- Vitamin D and calcium if at bone density risk
- Gradual dose titration of the GLP-1 medication — slower weight loss gives your body time to adapt
| Intervention | Evidence Level | Expected Impact |
|---|---|---|
| Resistance training 3-5x/week | Strong (case series + exercise science) | Reduce lean loss from 25-40% to under 10% of weight lost |
| Protein 1.2-1.5 g/kg/day | Strong (multiple expert guidelines) | Provides raw material for muscle protein synthesis |
| Creatine 3-5g/day | Moderate (strong for exercise, not GLP-1 specific) | Supports training intensity and muscle cell hydration |
| Ketone ester supplements | Preclinical only (mouse data) | Protects mitochondria; human trials pending |
| Bimagrumab + semaglutide | Early clinical | Preserves muscle pharmacologically; not yet available |
The JAMA Internal Medicine guidance offers a three-step progression that works for beginners: first, build to 150 minutes of moderate activity weekly starting with just 10 minutes daily; second, add strength training 2-3 times per week; third, maintain 30-60 minutes daily activity alongside continuing strength work. This graduated approach is more sustainable than jumping straight into an aggressive program while your body is adjusting to a new medication.
Monitor your progress beyond the scale. Body composition scans (DXA or bioimpedance), grip strength tests, and functional measures like how easily you can stand from a chair without using your hands all provide information that a scale number misses entirely. If you're losing weight but your squat is getting stronger, your lean mass is probably fine. If you're losing weight and struggling to open jars, that's a different conversation to have with your provider.
Frequently Asked Questions
Does Ozempic directly cause muscle loss?
No. GLP-1 drugs like Ozempic don't target muscle tissue through their pharmacological mechanism. Muscle loss occurs because of the caloric deficit and weight loss the drugs produce, not because of the drugs themselves. Any method of weight loss — dieting, surgery, medication — carries the same risk of lean mass reduction. The difference with GLP-1 drugs is the magnitude and speed of weight loss, which can amplify lean tissue losses when patients aren't actively working to preserve muscle.
How much muscle loss is normal on GLP-1 medications?
In clinical trials without structured resistance training, lean mass loss ranged from 0% to 40% of total weight lost, with a meta-analysis average around 25%. With consistent resistance training and adequate protein intake, published case series data shows this figure can drop to under 9% of weight lost — and some patients gained lean mass despite losing 13-27% of body weight.
What is the recommended protein intake while on Ozempic?
Expert recommendations converge around 1.0-1.5 grams of protein per kilogram of body weight daily for moderately active GLP-1 patients. Starting each meal with 20-30 grams of protein ensures you hit essential amino acid thresholds even when appetite is suppressed. If eating sufficient protein through whole foods proves difficult, a protein shake with at least 20 grams per serving can help bridge the gap.
Should I be concerned about bone density loss on GLP-1 drugs?
Weight loss from any cause affects bone density. A 10% reduction in body weight is associated with a 2.2% decrease in lumbar and total hip bone mineral density. Older women, postmenopausal women, and people with existing bone density concerns should discuss screening with their doctor before starting GLP-1 therapy. Weight-bearing exercise, adequate calcium, and vitamin D supplementation all help mitigate bone loss during weight reduction.
Can supplements alone prevent muscle loss on Ozempic?
Supplements support but don't replace the fundamentals of resistance training and adequate protein. Creatine monohydrate (3-5g daily) has strong general evidence for supporting muscle during exercise. Ketone esters showed protective effects in mouse studies, but human trials haven't been completed yet. No supplement can compensate for a sedentary lifestyle or inadequate protein intake.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











