
The pitch arrives the way most postpartum pitches now arrive: a sponsored Instagram reel, a group chat, a wellness clinic email. A small weekly injection or a powder in morning coffee will put your hormones back where they belong. The implication is that motherhood broke something a peptide can fix.
What the marketing rarely mentions is how thin the safety record is. Almost every peptide new mothers are offered — BPC-157, TB-500, sermorelin, CJC-1295, kisspeptin, even compounded GLP-1 blends — has not been formally studied in lactating women. The honest answer to "is it safe while I'm breastfeeding" is, in most cases, "nobody knows, because the trial has never been run." That is a different statement from "it's safe."
The Postpartum Hormonal Landscape: What Actually Crashes After Delivery
"Postpartum hormones" gets treated like one event. It is a sequence — overlapping, irregular, sometimes lasting two years — and the sequence is the only way to know which symptoms are normal recovery and which are signs of something specific.
The first crash is the obvious one. Within hours after delivery, estrogen and progesterone drop sharply, a shift that ACOG identifies as a likely trigger for early mood symptoms. Allopregnanolone — a progesterone metabolite that modulates GABA receptors and acts as an endogenous antidepressant — falls along with it. DynaMed describes this allopregnanolone collapse as a leading hypothesis for postpartum depression; the new oral PPD drug zuranolone is built on replacing it.
The second event runs on a slower clock. Postpartum thyroiditis affects roughly 5% to 10% of postpartum women, according to StatPearls, and it hides in plain sight because its symptoms — fatigue, mood swings, weight fluctuations, hair shedding — overlap with caring for a newborn. The classic course is biphasic: a thyrotoxic phase usually arriving 1 to 4 months after delivery, then a hypothyroid phase between 4 and 8 months, then recovery. Johns Hopkins notes that 4 in 5 women return to normal thyroid function within 12 to 18 months, but 20% to 30% develop permanent hypothyroidism, and Cleveland Clinic adds that roughly 20% of those who have had it develop it again in a later pregnancy.
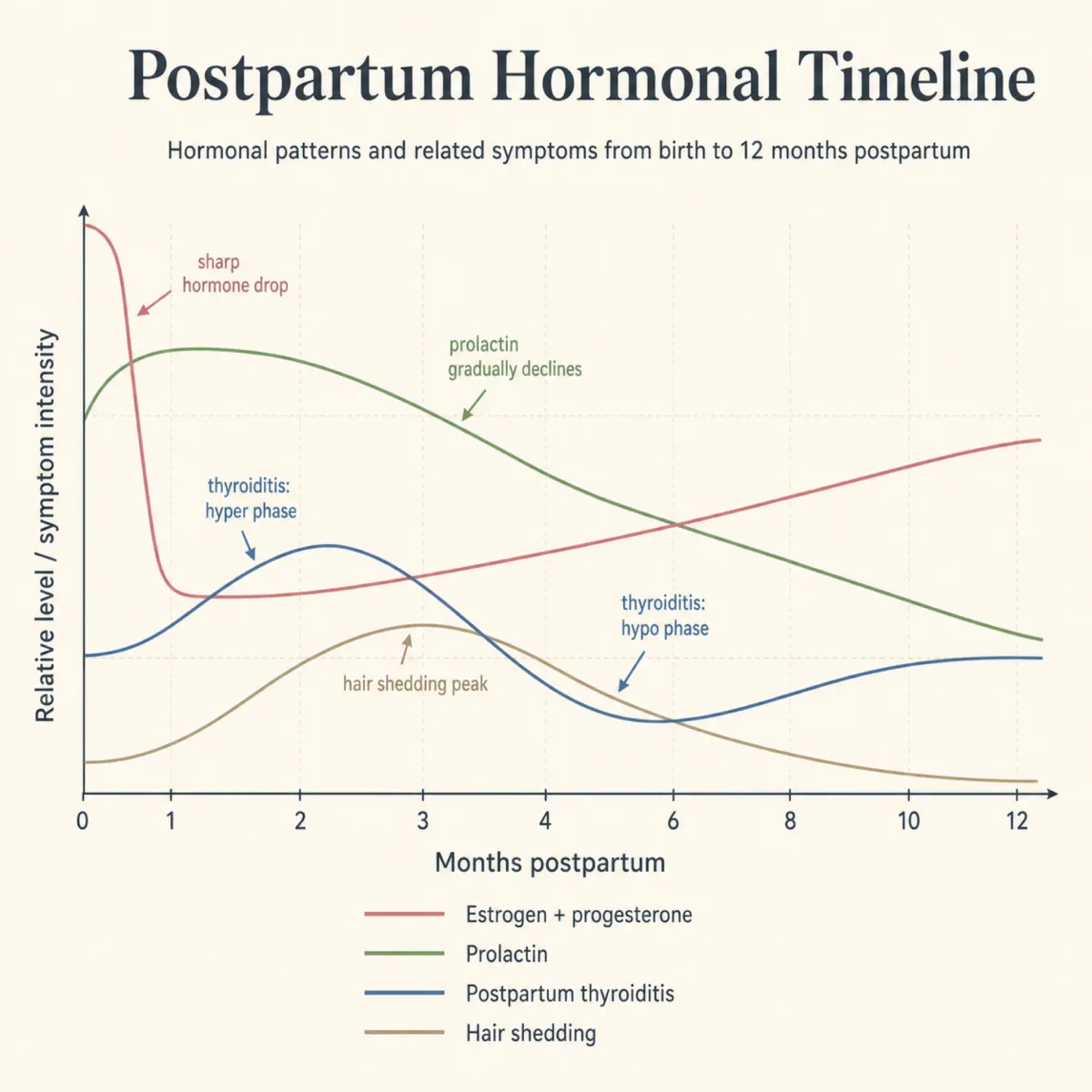
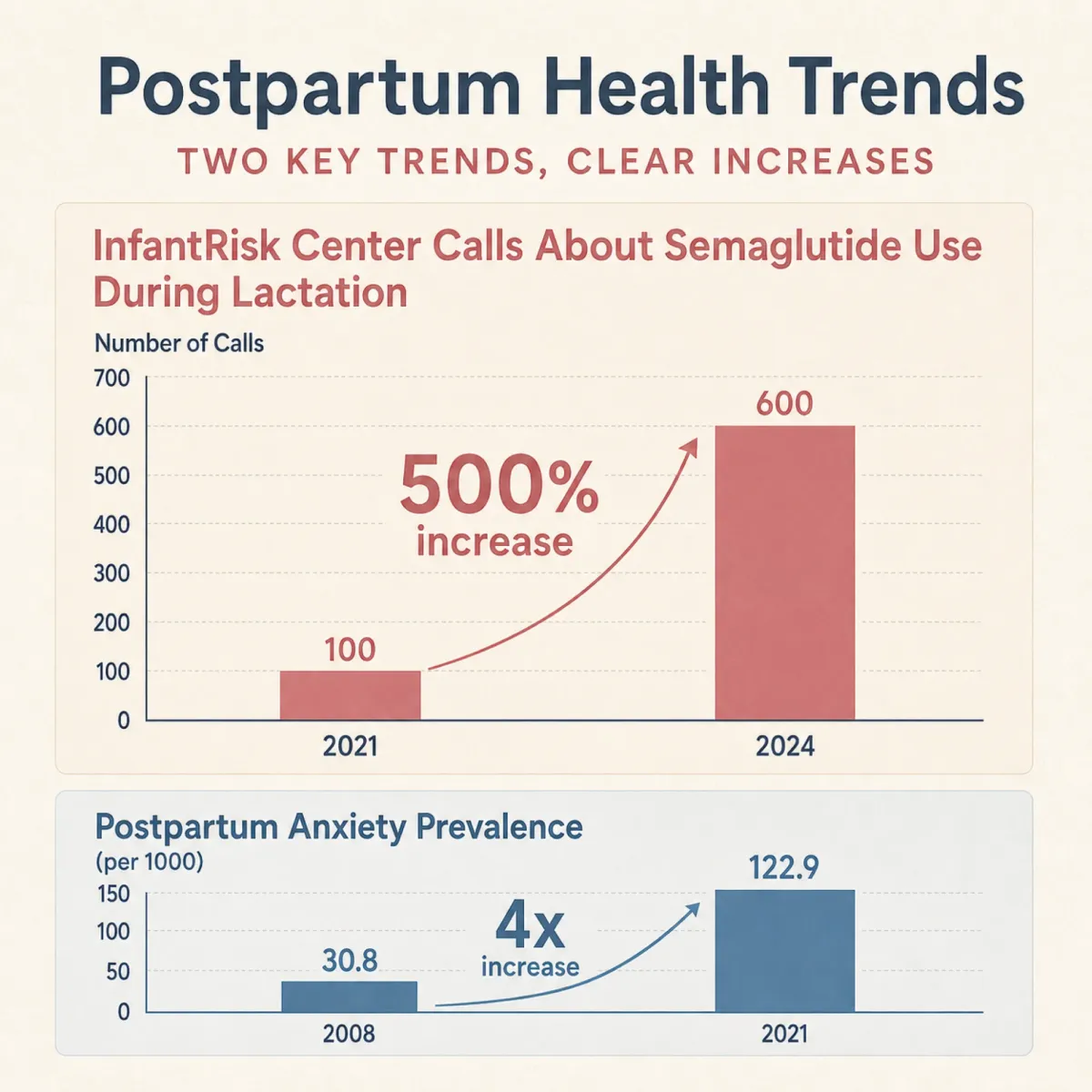
The third event is mood. The 2024 SMFM workshop summary in AJOG reports that up to 1 in 5 childbearing people experience a perinatal mental health condition and that mental health conditions, including suicide and overdose, are the leading causes of death in the first postpartum year. A U.S. cohort study summarized by OPQIC found new-onset postpartum anxiety in 5.8% of mothers within 12 months, with prevalence quadrupling between 2008 and 2021.
Telogen effluvium typically begins about 3 months after delivery and resolves within 6 to 12 months, driven by the same estrogen withdrawal that ends the prolonged growing phase pregnancy gave your hair. Skin changes — melasma, acne, stretch-mark hyperpigmentation — follow their own curve.
Lactation itself is a peptide-rich state. A study in the British Journal of Nutrition found that breastfeeding mothers between 3 and 6 months postpartum had baseline plasma PYY concentrations of 100.3 pg/ml versus 73.6 pg/ml in non-lactating mothers, with prolactin running more than four times higher. Your body is already running its own peptide protocol.
The Lactation Safety Data Gap: Why Almost No Peptide Has Been Studied in New Mothers
Pregnant and lactating women are excluded from almost every clinical trial. That exclusion is meant to protect them, but it means the prescribing line for any newer compound is some variant of "safety in pregnancy and lactation has not been established" — a phrase that tends to read as more reassuring than it should.
For BPC-157, the consumer health reference InnerBody is direct: "The safety of BPC-157 in pregnant or nursing individuals hasn't been established or investigated in research." The World Anti-Doping Agency has banned BPC-157 since 2022. Even a commercial vendor acknowledges that no studies confirm how either peptide interacts with estrogen, progesterone, or menstrual cycles, and that risks during breastfeeding "remain completely unstudied."
The Tampa wellness clinic Formation Med, in a piece titled "Who Should Avoid Using Peptides," lists pregnant or nursing mothers alongside cancer patients and those with kidney disease. When clinics with a financial stake in selling peptides are this clear, the recommendation deserves to be taken seriously.
Eric Topol, the Scripps Research cardiologist, devoted an essay titled "The Peptide Craze" to the broader picture: "The peptide craze is unfounded. The evidence base for use of these drugs, either for off-label indications or as non-approved drugs, is wanting." TB-500 accelerated dormant tumor growth in animal experiments. Growth-hormone-releasing peptides like CJC-1295, Ipamorelin, and Tesamorelin carry a theoretical cancer risk. Sermorelin, often marketed as "FDA-approved," was approved in 1997 and withdrawn in 2008.
What New Moms Are Actually Trying: A Survey of Forum Trends and Telehealth Pitches
The trend is measurable. A 2024 Nutrients study reported that drug-information calls about semaglutide use during lactation to the InfantRisk Center at Texas Tech University increased by more than 500% between 2021 and 2024. Postpartum mothers are calling academic medical centers about taking a GLP-1 while breastfeeding in numbers that have multiplied five-fold in three years.
The marketing at the practitioner level is striking. A Maryland women's health clinic sells what it calls the "Wolverine Blend" — a stack of 10 mg BPC-157 with 10 mg TB-500. In its own FAQ, the clinic explains that "clinics specifically highlight Wolverine Blend for women dealing with joint pain, recovery after childbirth or surgery, and high-demand training." Two questions later, the same FAQ lists pregnancy and breastfeeding as "poor candidates." Both statements sit on the same page; the contradiction is left for the patient to resolve.
At the higher end, Topol describes a Los Angeles "private health club" called LIVV that sells peptide menus including kisspeptin and KPV through an $85,000 premium membership or a $10,000 initiation fee plus $995 a month, with per-injection costs in the hundreds of dollars.
The mom-forum side looks different. A representative thread on r/postpartumprogress shows the pattern: a new mother asks if "hormonal balance supplements" are safe while breastfeeding, says her doctor told her there isn't enough data, and gets a mix of cautionary replies and brand suggestions. The supplements named are mostly herbal — myo-inositol, Wishgarden tinctures, St. John's Wort — not injectable peptides. The injectable trend is concentrated in influencer-adjacent and telehealth spaces, not the everyday breastfeeding community.
The Safer Tier: Food-Derived Peptides, Collagen, and Glycine
The peptide most postpartum mothers are reaching for and the peptide with the strongest safety record while breastfeeding are the same compound, and it is collagen.
The InfantRisk Center — the institutional source most U.S. clinicians use for medications-in-lactation guidance — addressed this directly in a September 2025 review. Their position: collagen is "a natural part of the human diet and body, and it's generally considered safe during breastfeeding. Because it is broken down into amino acids and small peptides during digestion, its impact on breast milk is likely minimal." They cite Ballard 2013, which found that moderate changes in maternal protein intake do not significantly affect milk protein content.
Two caveats matter. Most collagen studies are not breastfeeding-specific, and dietary supplements are not regulated for purity or potency the way medications are. The InfantRisk authors recommend third-party-tested brands and name several — Needed, Fullwell, Vital Proteins. A competing collagen brand reaches the same conclusion, with the caveat that vendors have an interest in saying their product is safe.
The mechanism is why this peptide sits in a different category. Hydrolyzed collagen is broken into peptide fragments during processing, and gastric proteases break the fragments down further into amino acids. Almost nothing recognizable as the original peptide reaches your bloodstream intact, and almost nothing reaches breast milk in a form that behaves differently from the protein in fish or bone broth. Glycine and glutamine share this profile. Bone broth, eggs, fish with skin, and leafy greens all support endogenous collagen synthesis.
Whether collagen does what the marketing claims for postpartum hair regrowth is a separate question. The Hopkins page on telogen effluvium does not list collagen among recommended interventions, suggesting patience, balanced nutrition, and consultation with a dermatologist about biotin or low-level laser therapy. The safety case is strong; the efficacy case is suggestive but thin.
The High-Risk Tier: Peptides Postpartum Women Should Approach With Extreme Caution
This category is everything else: BPC-157, TB-500, sermorelin, CJC-1295, Ipamorelin, kisspeptin, thymosin alpha-1, AOD 9604, Selank, Semax, Tesamorelin, Epitalon. The common feature is the absence of any human randomized clinical trial in lactating or recently postpartum women.
The GLP-1 family deserves a more nuanced treatment because the data picture has shifted. The traditional position, per the 2024 CMAJ summary, is that "lactating patients should avoid taking GLP1RAs" because of the paucity of human data. Two recent studies have begun to soften that stance on drug transfer specifically.
The Diab et al. study in Nutrients measured semaglutide in milk samples from 8 women using high-resolution mass spectrometry and did not detect the drug in any sample; worst-case projected relative infant dose was 1.26%, well below the 10% safety threshold. A more recent InfantRisk Center analysis reports tirzepatide was undetectable or barely detectable at doses up to 5 mg, with no observed effects in the breastfed infants studied.

On the narrow question of drug transfer to the infant, that is reassuring. But it is not the only question. The InfantRisk authors are clear that the larger concern is maternal nutrition. Lactation typically requires more energy than late pregnancy — about 2,000 calories per day plus an additional 250 for milk production — and GLP-1 medications can drop calorie intake by up to 39%. A breastfeeding mother whose appetite drops below the threshold for milk production risks losing her supply, becoming nutrient-deficient, and producing milk that is missing micronutrients. The InfantRisk recommendation is to wait until the infant is at least 7 months old, ideally 9 to 12. A Northside Hospital Q&A takes a more conservative line, saying GLP-1s are "not recommended during the postpartum period if you are breastfeeding."
For non-GLP-1 peptides, the picture is much simpler and less reassuring: no human breastfeeding studies exist. None of these compounds has been measured in human breast milk because the study has not been funded.
The Telehealth Prescribing Loophole: How Compounding Clinics Reach Postpartum Patients
The compounding pharmacy loophole is what makes postpartum exposure so wide. When the FDA designated semaglutide as in shortage, compounding pharmacies were permitted to produce custom-mixed versions, often at lower price points than brand-name Ozempic or Wegovy. Those compounded versions are still prescribed widely through telehealth.
The Northside Hospital Q&A with Dr. Jyoti Manekar spells out the risk: "Compounded GLP-1s ... are not FDA-approved or regulated for consistency, purity or efficacy, and some do not use the same salt form, which may affect how the drug works. There have been recent concerns about contaminants, incorrect dosing, or inactive ingredients, which is why, as a physician, I would advise caution with compounded versions, especially during sensitive periods like postpartum."
The same dynamic applies to compounded BPC-157, TB-500, and growth-hormone-releasing peptides sold through wellness clinics. InnerBody warns that "research-grade peptides ... are not intended for use in humans, and their safety can't be guaranteed." A compounded vial bought online has no FDA-verified potency and no guarantee that the label matches what is in the syringe.
The economic incentive is real. A monthly peptide subscription generates revenue in a way that a recommendation to wait six months does not. Patient demand plus prescriber willingness plus absent regulation produces a market in which postpartum women receive prescriptions for compounds with no lactation safety data, often without the prescriber knowing the patient's breastfeeding status, calorie intake, or thyroid function.
When and How to Consult Your OB or Primary Care Doctor Before Trying Anything
If something feels off in the first postpartum year — mood, energy, sleep, hair, weight, milk supply, anxiety — call your OB or primary care doctor before you call a wellness clinic. Several of the most common causes are treatable in ways that peptides are not.
If your symptoms include fatigue, mood changes, weight gain, dry skin, or low milk supply, the first test on the table should be a thyroid panel. StatPearls notes postpartum thyroiditis is frequently underrecognized because its symptoms overlap with those of being a new parent. The American Thyroid Association, the Endocrine Society, and ACOG all recommend evaluating thyroid function in any postpartum patient diagnosed with postpartum depression. A simple TSH and free T4 measurement clarifies the picture.

If your symptoms are predominantly mood, the data make the case for early intervention. The SMFM workshop summary is blunt: more than 50% of birthing parents with postpartum depression go undiagnosed, approximately 85% do not receive treatment, and 95% to 97% are not treated to remission. SSRIs in pregnancy and postpartum, when adjusted for the underlying condition, are not associated with congenital anomalies or developmental abnormalities, and the levels in breast milk are generally very low. ACOG describes three established treatments: zuranolone (a 14-day course requiring a breastfeeding pause), antidepressants, and talk therapy, often in combination. None are peptides, and all have substantially better lactation safety records than the unstudied compounds marketed online.
For weight retention, the conversation is harder because it touches body image at a vulnerable moment. Research shows postpartum weight retention averages 0.5 to 3.8 kilograms at 2.5 years, that one live birth raises the risk of becoming obese by roughly 110%, and that weight loss at 6 months is the strongest predictor of long-term retention. Those numbers do not mean the answer is a compounded GLP-1 within the first 6 months. Per InfantRisk and Northside, GLP-1s should be deferred until lactation is established or finished.
The questions worth asking your provider before starting any peptide are concrete. Is there a contraindication based on my thyroid status, my mental-health history, or my breastfeeding status? Has this compound been studied in breastfeeding women, and if not, what does that mean? Is the source pharmaceutical-grade or research-grade? What is the plan if my milk supply drops? A clinic that cannot answer those questions in plain language is a clinic that should not be writing the prescription.
Frequently Asked Questions
Can I take collagen peptides while breastfeeding?
Yes, generally. The InfantRisk Center states collagen is broken down into amino acids and small peptides during digestion, so its impact on breast milk is likely minimal. Choose a third-party tested brand.
Are BPC-157 and TB-500 safe after I give birth?
Nobody knows, because the studies have not been done. InnerBody states BPC-157's safety in pregnant or nursing individuals has not been established or investigated, and commercial vendors of the BPC-157 / TB-500 stack list breastfeeding as a contraindication. Treat marketing claims with skepticism and the contraindication as the more reliable information.
I think I might have postpartum thyroiditis. What should I do?
Call your OB and ask for a TSH and free T4 blood test. PPT affects 5%-10% of postpartum women and is often missed because symptoms — fatigue, mood changes, hair loss — overlap with normal postpartum recovery. Treatment is straightforward: beta-blockers for the thyrotoxic phase, levothyroxine for the hypothyroid phase if needed. Roughly 4 in 5 women return to normal thyroid function within 12 to 18 months.
If GLP-1s do not transfer into breast milk, why are doctors still telling me to avoid them while nursing?
Because drug transfer is only one of the safety questions. Diab et al. in Nutrients suggests semaglutide and tirzepatide do not reach the infant through breast milk in meaningful amounts. The bigger concern is maternal nutrition — GLP-1s can reduce calorie intake by up to 39%, and lactation requires roughly 2,000 calories a day plus 250 more for milk production. InfantRisk recommends waiting until the infant is at least 7 months, ideally 9-12.
Is zuranolone a peptide?
No. Zuranolone is a synthetic analog of allopregnanolone, a progesterone metabolite that modulates GABA receptors. Per DynaMed, it is the first FDA-approved oral medication specifically for postpartum depression, given as a 14-day course. It does pass into breast milk, so ACOG advises a planned breastfeeding pause during treatment plus 1 week after the last dose.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.











