39,000 men died by suicide in one year. Most never sought help.
In 2022, 39,282 men died by suicide in the United States, accounting for nearly 80% of all suicide deaths that year. Men die by suicide at roughly four times the rate of women. Among men over 65, that ratio climbs to six times. For men aged 25 to 34, the rate has risen 34% since 2010.
Behind every one of those numbers is someone who went quiet. A coworker who seemed fine on Friday. A friend whose texts just stopped.
Depression alone affects over 6 million American men each year, yet it goes undiagnosed at far higher rates than in women. The reason is not biological mystery. It is a recognition problem. Men's depression tends to look different from the clinical textbook version. Instead of sadness and withdrawal, men more commonly show anger, irritability, aggression, substance misuse, and risk-taking behavior. A doctor scanning for tearfulness and low appetite will miss the guy who just punched a wall and drank a twelve-pack. The symptoms are real, but the clinical framing was built for a different presentation.

The treatment gap puts this in context. According to NAMI's 2023 data, only 45.9% of U.S. men aged 18 and older with a mental illness received any treatment in the preceding year. Nearly 1 in 10 men experience depression or anxiety, and fewer than half get help.
Standard screening tools may undercount men entirely. The Illinois Department of Public Health notes that male symptoms tend to be more "externalized" -- anti-social behavior, aggression, substance abuse -- compared to the internalized patterns like withdrawal and appetite loss that instruments such as the PHQ-9 were designed to detect. Men also default to distraction: excessive exercise, media binges, oversleeping. None of that flags on a standard depression questionnaire.
The screening tools were built for symptoms that skew female. Men slip through the diagnostic net, get told they do not have a problem, and that confirms the belief they should not have sought help in the first place. A feedback loop with no obvious exit.
The threefold trap that keeps men silent
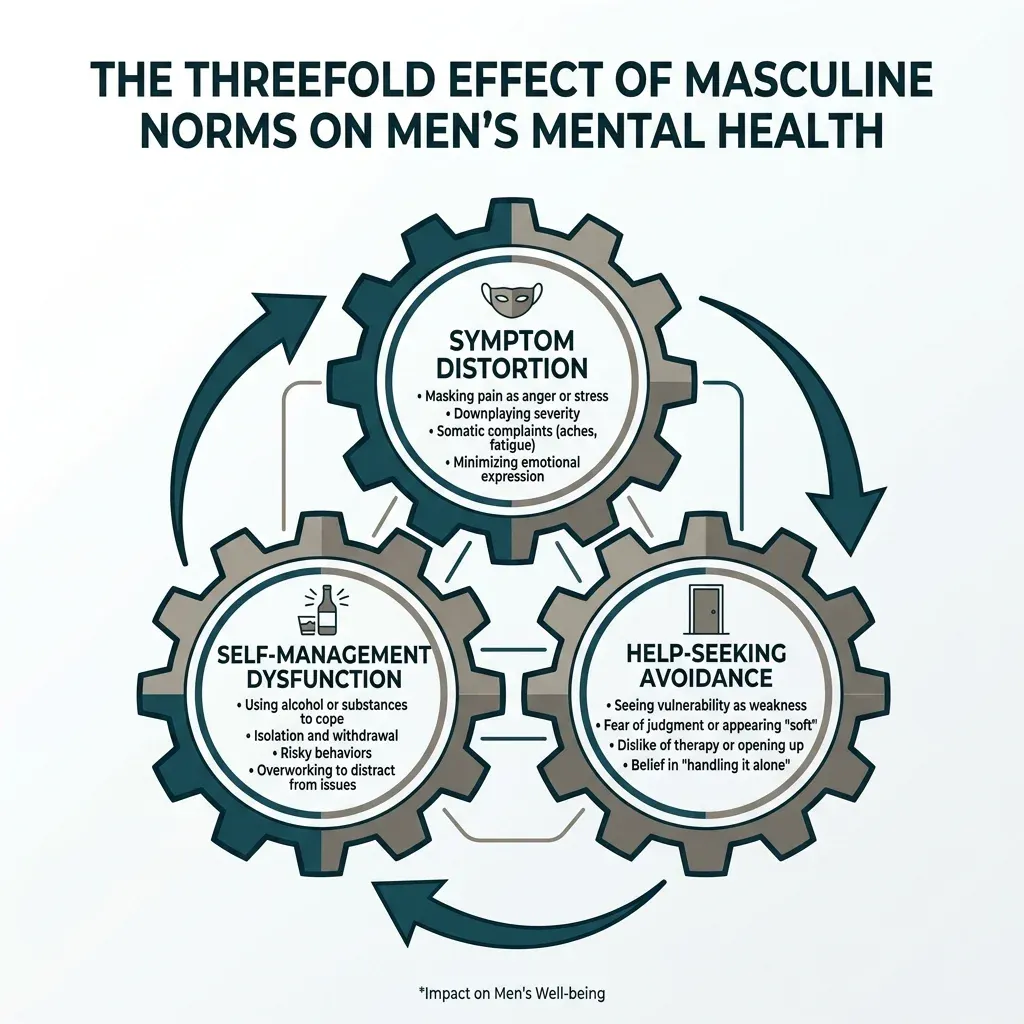
Researchers Zac Seidler, Andrew Dawes, and Simon Rice reviewed 37 studies on masculinity and depression help-seeking and found that traditional masculine norms create what they called a "threefold effect." Conformity to those norms distorts how men experience symptoms, how they feel about getting help, and how they manage symptoms on their own. Each layer reinforces the others.
Think of a smoke detector wired backward. The alarm does not go off when smoke fills the room. Instead it signals that everything is fine. That is roughly what happens when a man has been socialized to interpret emotional pain as weakness. The pain stays. It just gets reclassified as something to push through.
A larger 2025 systematic review by Leshata Mokhwelepa and Gsakani Sumbane, covering 47 studies across multiple countries, confirmed two patterns. First, masculinity worsens mental health through emotional suppression. Second, the fear of being perceived as weak creates active avoidance of help-seeking across cultures.
A separate scoping review published in the Journal of Mental Health Counseling sorted these barriers into three buckets: masculinity and identity conflicts, male attitudes and behaviors (self-reliance, poor mental health literacy, substance use as coping), and problems with psychological services themselves, including the perception that therapy is a "feminized" space. That last category gets less attention, but clinicians ignore it at their patients' expense.
There is also a clinical term for something men experience but rarely have language for: normative male alexithymia. It describes the difficulty men have recognizing and naming their own emotions -- not because of a neurological deficit, but because they have been trained since childhood to suppress emotional awareness. You cannot seek help for something you cannot identify.
The racial dimension compounds all of this. CDC data shows that among men aged 18 to 44 with daily anxiety or depression, non-Hispanic Black and Hispanic men (26.4%) were roughly 40% less likely than non-Hispanic White men (45.4%) to use mental health treatments. Cultural stigma stacks on top of gender stigma. The barriers multiply rather than add.
A 36% jump in two years
Something shifted during the pandemic. According to the CDC's National Health Interview Survey, mental health treatment among men aged 18 to 44 rose from 13.1% in 2019 to 17.8% in 2021, a statistically significant 36% increase. Women's treatment rates also climbed, from 23.8% to 28.6%, but the male increase was proportionally larger from a much lower base.
The 2025 systematic review by Mokhwelepa and Sumbane observed a "growing tendency in the number of men seeking emotional help" during the pandemic, citing research by Ellison and colleagues that documented this shift in real time. Isolation stripped away the usual escape routes. No office to disappear into, no bar afterward, no game on the weekend. What was left was whatever had been building underneath.
The cultural conversation shifted too. Movember released survey data in 2021 showing that four out of five Canadian men planned to prioritize their mental health, ranking it above career and romantic relationships.
Institutional recognition played a part. The American Psychological Association released its first-ever guidelines for psychological practice with boys and men in 2019, formally acknowledging what researchers had been saying for years: psychotherapy had been designed around women's patterns of engagement, and men needed different approaches.

A 36% increase from 13.1% still means only 17.8% of men in that age group got treatment. The movement is real, but calling it solved would be absurd. Most men who need help still are not getting it.
Forget the couch: what therapy for men actually looks like
The image of lying on a leather couch and talking about your childhood may be the single biggest misconception keeping men away from treatment. Modern evidence-based therapy, particularly the approaches that work well for men, looks nothing like that.
Research consistently shows that men respond better to structured, action-oriented therapy than to open-ended emotional exploration. Effective therapists working with men tend to set clear goals, build concrete skills, and track measurable progress. Less confessional, more like working with a coach who understands how your brain works.
Cognitive behavioral therapy (CBT) works well for men because it is built around identifying distorted thinking patterns and replacing them with more accurate ones. It is systematic and evidence-based, which appeals to men who want to understand the logic behind what they are doing. Dialectical behavior therapy (DBT) adds emotional regulation skills and is particularly effective when self-destructive behavior is part of the picture.
| Therapy type | Best for | What it involves |
|---|---|---|
| CBT | Depression, anxiety, negative thought patterns | Identifying and restructuring distorted thoughts with structured exercises |
| DBT | Emotional regulation, self-destructive behavior | Skills training in distress tolerance, emotional management, mindfulness |
| IFS | Anger management, suppressed emotions | Understanding internal "parts" (protector, manager, exile) and their roles |
| Coaching-style | Men new to therapy | Goal-setting, emotional vocabulary building, progress tracking |
One approach gaining traction with men is Internal Family Systems (IFS) therapy. IFS frames the psyche as made up of distinct "parts," each serving a protective function. The "firefighter" jumps into action with anger or substances when something painful surfaces. The "manager" tries to prevent pain through control and self-criticism. The "exile" holds the painful emotions that both other parts are working to suppress. For men who have spent years believing their anger is a character flaw or their sadness is weakness, learning that these are protective mechanisms -- not defects -- can change how they relate to themselves.
Clinicians have also found that changing the language of therapy helps. Explaining the process up front, using coaching terminology, and teaching emotional vocabulary as a skill (rather than assuming men already have it) removes a real barrier. You would not hand someone a wrench and expect them to rebuild an engine without explaining what each tool does. Emotional literacy works the same way.
When strength gets redefined
There is a persistent belief that traditional masculinity and mental health treatment are incompatible. The research tells a more complicated story.

The 2025 systematic review found something that complicates the simple "masculinity is toxic" narrative. Some traditional masculine traits -- perseverance, strong work ethic, and resilience -- actually helped coping when men reframed therapy as a challenge to overcome rather than an admission of failure. Men who viewed recovery as proving their resilience, aligning with what researchers described as "heroic" masculinity, were more likely to stick with treatment.
Iman Sagar-Ouriaghli and colleagues identified specific behavior change techniques that measurably improved male help-seeking in their 2019 systematic review. The effective interventions shared common elements: role models who demonstrated that seeking help was compatible with masculinity, psychoeducational material that improved mental health literacy, tools for recognizing and managing symptoms, active problem-solving tasks, and content that built on positive masculine traits like responsibility and strength.
That last point is worth sitting with. The most effective programs did not try to dismantle masculinity. They worked with it. They reframed therapy as an act of responsibility rather than vulnerability, and men responded.
| Myth | What the evidence says |
|---|---|
| Therapy means you're weak | Men who reframe therapy as demonstrating resilience have better treatment adherence |
| Men don't benefit from therapy | CBT, DBT, and IFS show strong outcomes for men when approaches match their engagement style |
| Real men handle it themselves | Self-reliance without treatment leads to substance misuse and worsening symptoms in research |
| Only severe cases need therapy | Early intervention produces better outcomes; therapy works for everyday stress and relationship issues |
Finding a therapist without the runaround
The practical barrier nobody warns you about is how annoying it is to actually find a therapist. It is not one phone call. It is often a dozen. Many therapists do not return voicemails. Waitlists stretch for months. Insurance directories list providers who stopped accepting new patients years ago.
Start with your primary care doctor. The NIMH recommends this as the first step because your doctor can screen for underlying conditions, prescribe medication if appropriate, and refer you to a psychologist, psychiatrist, or clinical social worker. This also gets mental health into your medical record, which matters for insurance continuity.
Insurance matters more than people realize. CDC research found that among insured men aged 18 to 44, there was no statistical difference in treatment rates between racial and ethnic groups. But among uninsured men in the same age range, White men were three times as likely as Black and Hispanic men to access treatment. Insurance closes the cost barrier, and the effect goes further: it nearly eliminates the racial treatment gap.
If cost is a concern, look into community mental health centers, sliding-scale therapists, and university training clinics where supervised graduate students provide therapy at reduced rates. Many employers also offer Employee Assistance Programs (EAPs) that provide several free sessions.
When evaluating therapists, ask about their experience working with men and their therapeutic approach. A therapist who leads with "Tell me about your feelings" on day one may not be the right fit. Look for someone who can explain their process, set goals with you, and adjust their style. Trying two or three before committing is normal.
Your first session: what to expect
The first session is mostly intake. The therapist will ask about your history, current symptoms, and what brought you in. You do not need a speech prepared. "I've been angry a lot and I don't know why" is a perfectly good starting point.

A few things about the first session tend to surprise men. The therapist probably will not give you advice right away. They are building a map of your situation first. They will not judge you for not having the right words either -- normative male alexithymia means most men have not been taught emotional vocabulary, and a good therapist knows how to teach it.
If the first session feels awkward, that is normal. You would not expect to be good at any new skill on the first attempt. Give it three sessions before deciding whether it is working. By session three, you will have a sense of whether the therapist's style matches what you need.
| Before your first session | What to do |
|---|---|
| Write down what's bothering you | Even a few bullet points helps your therapist understand the core issues |
| Check insurance coverage | Call your insurer and ask which mental health providers are in-network |
| Ask about the therapist's approach | Most offer a free 15-minute consultation call; use it to ask about their style |
| Know your crisis resources | 988 Suicide and Crisis Lifeline: call, text 988, or chat at 988lifeline.org |
One more thing worth knowing: therapy is confidential. What you say stays between you and your therapist, with narrow exceptions involving imminent danger. Your employer will not know. Your friends will not know. Your insurance company gets a diagnosis code, not session transcripts.

The systematic review by Sagar-Ouriaghli identified exposure to male role models as one of the behavior change techniques that improved help-seeking among men. Hearing that another man -- someone they could identify with -- had gone to therapy and come out better for it carried real weight in the research. If you have been through it, talking about it might be the most useful thing you do for the men around you.
Frequently asked questions
How do I know if I need therapy or if I'm just going through a rough patch?
If the rough patch has lasted more than two weeks and is affecting your sleep, work, relationships, or substance use, it is worth talking to someone. You do not need a diagnosed condition to benefit from therapy. Men who show up early tend to need fewer sessions and recover faster than those who wait until things reach a crisis.
Will my therapist try to make me talk about my feelings the entire time?
Not if they are good at working with men. Evidence-based approaches like CBT and DBT are structured around problem-solving, skill-building, and changing specific thought patterns. A competent therapist will adapt to your communication style rather than forcing a framework that does not fit.
What if I can't afford therapy?
Check your insurance first -- the Mental Health Parity Act requires insurers to cover mental health treatment at the same level as physical health. If you are uninsured, community mental health centers offer sliding-scale fees, and university training clinics provide reduced-cost therapy with supervised graduate students. Many employers also offer free EAP sessions.
Is online therapy as effective as in-person therapy?
For most conditions treated with talk therapy, yes. Research published during and after the pandemic shows that telehealth therapy produces comparable outcomes to in-person sessions for depression and anxiety. Online therapy also removes a practical barrier: the logistics of physically showing up during business hours.
How long will I need to be in therapy?
It depends on what you are working on. CBT for specific issues like anxiety or depression typically runs 12 to 20 sessions. Some men come weekly for a few months, then shift to monthly check-ins. Others find that a short course gives them the tools they need and they stop. There is no minimum contract.
Medical Disclaimer
This article is for informational and educational purposes only and is not medical advice, diagnosis, or treatment. Always consult a licensed physician or qualified healthcare professional regarding any medical concerns. Never ignore professional medical advice or delay seeking care because of something you read on this site. If you think you have a medical emergency, call 911 immediately.